
Sevgi Anar Ozdinc ( Healthy Science Faculty, Physical Therapy and Rehabilitation Department, Turkey. )
Fatma Nesrin Turan ( Medical Faculty Bioistatistic Division, Trakya University, Edirne, Turkey. )
July 2016, Volume 66, Issue 7
Original Article
Abstract
Objective: To investigate the effects of ballet training on foot structure and the formation of the medial longitudinal arc in childhood, and the association of body mass index with structural change secondary to ballet training.
Methods: This study was conducted at Öykü Ballet and Dance School and Trakya University, Edirne, Turkey, from September 2007 to November 2008, and comprised girl students who were taking ballet classes, and a group of those who were not taking such who acted as the controls. Static footprints of both feet of all participants were taken with an ink paedogram. Parameters evaluated from footprints included foot length, metatarsal width, heel width and medial longitudinal arch. The relationship between the parameters, the ballet starting age, training duration and body mass index was investigated.
Results: Of the 67 participants, there were 36(53.7%) in the experimental group and 31(48.3%) in the control group. The difference between age, height, weight and body mass index between the two groups was insignificant (p>0.05). The average ballet starting age was 6.47±1.55 years and duration was 4.36±2.002 years. Positive correlations were found between body mass index and foot length, metatarsal width, heel width, medial longitudinal arch contact width and halluxvalgus angle; between ballet starting age and metatarsal width, heel width; between duration of training and foot length, metatarsal width and hallux valgus angle (p?0.05 each).
Conclusion: Evidence supporting the effect of ballet education in children on foot anthropometric measurements and medial longitudinal arc development could not be found.
Keywords: Foot, Medical Longitudinal Arch, Ballet Training. (JPMA 66: 869; 2016)
Introduction
Foot health and biomechanics are a significant issue in ballet. The human foot is a biological masterpiece. It is strong enough to bear body weight and flexible enough to adapt to the floor. Deviations in sequencing affect the whole body posture. While walking, it has responsibility for the absorption of ground reaction forces (GRF), adaptation to the floor and forward movement.1
Foot consists of 28 bones, numerous ligaments and muscles and 3 basic foot arches which are medial longitudinal, lateral longitudinal and transverse. The foot arch is very important in terms of foot structure and biomechanics. Most scientific researches focus on medial longitudinal arch (MLA). Low MLA reduces hindfoot stability and forces calcaneus to valgus, causing tendon laxity, tiredness and load distribution to the medial axis.1,2 Many factors contribute to change in MLA, such as age, gender, genetics, shoes, body weight, flexibility and muscle force.3-8
A high arch cannot absorb shock, and it increases the incidence of ankle sprain. The control of foot structure is even more difficult with a low arch. Feet with a low arch cause more pronation while walking, and this might increase the risk of overuse injuries.1,3,9 Additionally, foot-related deformities result in biomechanics problems, stress breaks and decreased performance in upper segments, such as foot ankle, knee and hip.1,9-11 MLA and other foot arches appear when a child starts to walk, and the age up to six years is critical. It has been claimed that foot structuring continues up to 14 and even 16 years, even though it might be slower.6,7,12-14
There are several measurements of the foot structure such as height of MLA, hallux valgus angle (HVA) or various foot indices. In the present study, length, width, proportion and index were used for evaluating foot structure.
The current study was planned to determine whether foot structure and MLA development are affected by a training programme that forced regular intrinsic and extrinsic muscle use in children who attended ballet school. Body mass index (BMI) of the participants was also assessed to relate it with structural change secondary to ballet training.
Subjects and Methods
This study was conducted at Öykü Ballet and Dance School and Trakya University, Edirne, Turkey, from September 2007 to November 2008, and comprised girl students who were taking ballet classes while a group of those who were not taking such classes acted as the controls. In the experimental group, students who had been studying for at least two years were included. In the control group, participants of matching age who did not perform any sporting or special physical activity were included. Those with pre-existing health conditions (e.g. rheumatic and musculoskeletal problems) or previous surgeries were excluded from both groups. Informed consent was obtained from the participants\\\' families. Ethical approval was obtained from the institutional committee.
The experimental group undertook a training programme twice a week for an hour and for eight months for training duration each year. Through a socio-demographic questionnaire, they were asked about their age, height, weight, their age when they started ballet and how long they had been dancing. After including BMI as a parameter, a static footprint method was applied to both feet of all participants by the same person with an ink paedogram, which is one of the most reliable methods.7,8,15 All measurements for both groups were taken in the afternoon between 3:00 and 5:00 p.m. Furthermore, all measurements for the experimental group were taken before ballet training. Footprint measurements were taken by using a ruler, a goniometer and mathematical calculations.
Parameters evaluated from footprints (Figure):2,7,15-18 footlength, AB width, AC width, BC distance, DE distance, DF distance; EF distance, heel width (HJ distance), K (HVA), R (metatarsus angle); M=Foot angle, Foot Index=AB/foot length×100; FE/DE, GD distance (if the G point was a lateral D point, a negative value was given); and AC/HJ, DE/HJ (Staheli index), AC-AB.
Measurements were repeated three times to avoid any bias. The two groups were compared by calculating the arithmetic average of all parameters and their standard deviations.
Additionally, the correlation between BMI in all participants, ballet starting age (BSA) and duration and foot anthropometric parameters was evaluated. Statistical evaluation was made using STATISTICA AXA 7.1 statistic programme. After evaluating the compliance of measurable data to normal distribution using a sample Kolmogorov-Smirnov test, a t-test was used in the independent group for those showing normal distribution, and a Mann-Whitney U test was used for those not showing normal distribution. To evaluate the relationship between variables, a Spearman\\\'s rank-order correlation (Spearman\\\'s rho) analysis was used. Median values, arithmetic average and standard deviation were measured for descriptive statistics. P<0.05 was considered significant.
Results
Of the 67 participants, there were 36(53.7%) in the experimental group and 31(48.3%) in the control group. The difference between age, height, weight and BMI between the two groups was insignificant (p>0.05). The average BSA was 6.47±1.55 years (median: 6; interquartile range [IQR] 4-11) and mean duration was4.36±2.002 years (median: 4; IQRL 2-11 years).
The difference between the foot anthropometric values of both groups was also statistically insignificant for all parameters (Table-1)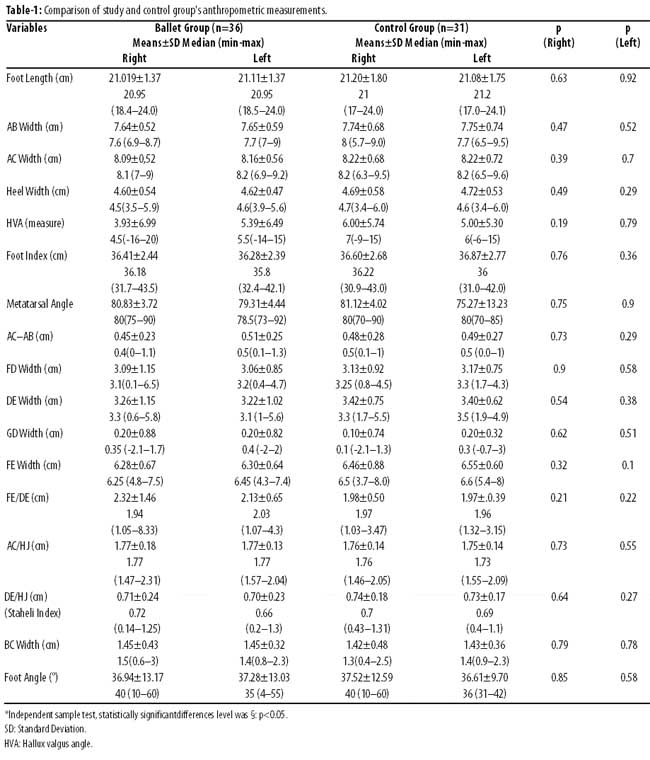
A positive correlation with BMI was found for both feet in terms of length, AB, AC, DE, HJ, FE and HVA.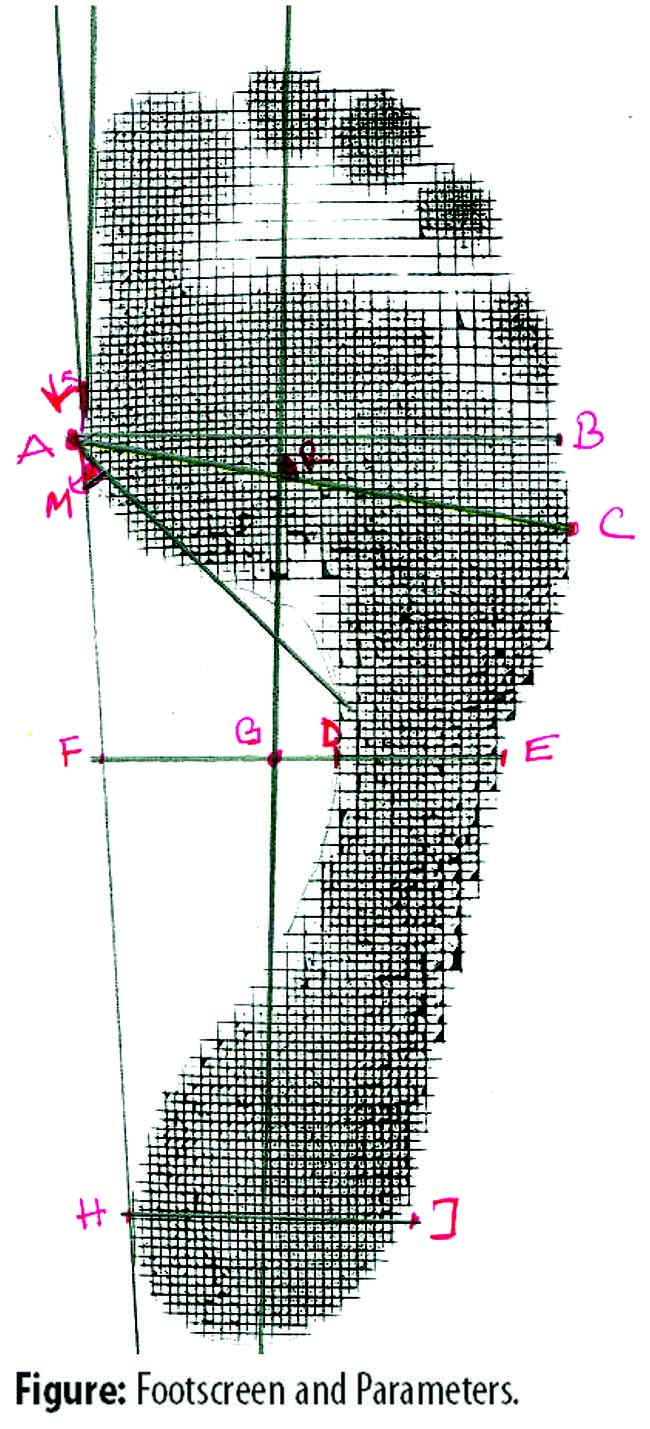
For both feet, a positive correlation was found between FE, AC, heel width and BSA, and a negative correlation was found between AC/HJ ratio and BSA, but only for the right foot (p<0.05). A positive correlation between ballet duration and (right) foot length, AC and HVA and (left) AB, AC, HVA and FE parameters was found (Table-2)
A positive correlation close to the significance limit was found between foot angle, especially on the right and ballet duration (p= 0.055).
Discussion
The footprint method is a sensitive method to detect foot morphology and disorders.7,8,14,19 There are various evaluation formulas used in this method. For example, at the highest level MLA, if the width of the part touching the ground (FD) is 1cm and below, it is considered flat foot; if the part touching the ground (DE) is 1cm or below, it is evaluated as high arch.6 Another simple formulation is as follows: if the proportion of the long arch width to heel width DE/HJ is above 0.7, it is evaluated as pesplanus (Staheli Index).15,19,20 Foot angle is the angle between the deepest part of the metatarsal MLA and medial longitudinal line; 0-29.9 degrees flat, 30-34.9° low, 35-41° borderline and 42° up are evaluated as a normal foot.14,16,21 It is emphasised that the active use of foot muscles has a positive effect during the development of MLA. Two studies about this issue are very striking. A study found BMI and flat foot lower in children who use their muscles more actively by playing on the ground than those living in cities.17 Another study found that wearing closed shoes earlier than six years of age can increase pesplanus incidence by decreasing the use of intrinsic foot muscles.6
In this study, no significant differences were found in the MLA parameters between groups. This result was due to insufficient training time. All parameters were better in the experimental group, but they were all below the significance limit.
A positive correlation was found between BMI and (in both feet) foot length, AB, AC, heel width, DE and FE parameters and (right foot only) HVA. HVA was also within significance limit for the left foot.
This increase of BMI in the width and length of the foot corresponds with the literature.22-24 Increase in the distance between AC and AB, which means a widening in the metatarsal area, corresponds with an increase in the HVA that complies with a hallux valgus deformity formation mechanism. There was scant literature on the relationship between hallux valgus and BMI (obesity).24 In a meta-analysis published in 2012, it was shown that sufficient evidence could not be proposed.24 The parallel increase in DE distance to BMI signals a decrease in MLA, or, in other words, an increase in the pesplanus inclination. As emphasised in many studies, the increase in BMI is a risk factor for pes planus.4,16
The incidence of pesplanus was observed to be the highest at age six and lowest at age 11 and above (p<0.05). It was stated that this percentage is 28.5% among boys and 35.5% among girls. The tendency of pesplanus during the preschool period was shown to be 52% with boys and 36% with girls. As children get older, the incidence of pesplanus decreases (0-3 > 3 > 6 years of age).6,7,13
The heredity factor showed that the pesplanus percentage is 16.1%; it is 5.6% in those without a family history14 (p=0.001).
A positive correlation was found between BSA and FE as well as AC and heel width in both feet. A negative correlation was found between AC/HJ and the left foot only (respectively; (p<0.05).
There is a distinctive increase in foot width, especially in heel width, when BSA is late. A positive correlation was observed in both feet between the duration of ballet and foot length and AC and HVA. On the left foot, AB and FE parameters were also correlated. A higher training period is always related to higher age. A higher age is always correlated to longer feet in children.
Keeping in mind that children continue to grow during ballet duration, a significant relationship was found between increases in ballet duration and width (especially in the metatarsus area), length parameters and the HVA. AB and AC distances accompanied the increase in HVA angle, which complies with the literature. Additionally, it proves the claims that loads made on the forefoot are risk factors for hallux valgus deformity.24 Additionally, a relationship in the significance limit (p=0.055) was found between the duration of ballet and foot angle on the right foot. We consider that the increase in the duration of ballet and/or getting older causes an increase in the metatarsus angle and in MLA, and it signals that exercise (ballet) might have an effect on the development of MLA. A correlation between MLA height and evertor muscles was found in a study conducted on elite gymnastics.25
Conclusion
Evidence supporting the effect of ballet education in children on MLA formation could not be found. Late BSA and limited duration were considered risk factors. A relationship was found between BMI, BSA, ballet education duration, width measurements and HVA. Ballet education and the increase in BMI were found to be risk factors for hallux valgus deformity. The study must be repeated with professional ballerinas. Future studies must be planned to prove the relationship between ballet training and foot structure and function as cohort investigations.
Disclosure: Our study was presented in XV, Advances of Physiotherapy and Rehabilitation Congress in April 2014, Ankara.
Conflict of Interest: None.
Funding Source: None.
References
1. Hillstrom JH, Song J, Kraszewski PA, Hafer FJ, Mootanah R, Dufour BA, et al. Foot type biomechanics part 1:Structure and function of the asymptomatic foot. Gait Posture 2013; 37: 445-58.
2. Pauk J, Ihnatouski M, Najafi B. Assessing plantar pressure distribution in children with Flatfoot arch application of the Clarke angle. J Am Podiatr Med Assoc 2014; 104: 622-32.
3. Demneh SE, Jafarian F, Melvin JMA, Azadinia F, Shamsi F, Jafarpishe M. Flatfoot in school-age children. Prevelance and associated factors. Foot Ankle Spec 2015; 8:188-93.
4. Aras U, Bek N, Yakut Y. The relationship between body weight and foot deformities in children of different ages. Turkey Clin J Pediatr 2010; 19: 30-7.
5. Chen CK, Tung HC, Yeh JC, Yang FJ, Wang HC. An Investigation of the factors affecting flatfoot in children with delayed motor development. Research in Developmental Disabilities 2014; 35: 639-45.
6. Abolarin T, Aiyegbusi A , Tella A , Akinbo S. Predictive factors for flatfoot: The role of age and footwear in children in urban and rural communities in South West Nigeria. The Foot 2011; 21:188-92.
7. Chang HJ, Wang HS, Kuo LC, Shen CH, Hong WY, Lin CL. Prevalence of flexible flatfoot in Taiwanese school-aged children in relation to obesity, gender and age. Eur J Pediatr 2010; 169: 447-52.
8. Chen CK, Tung HC, Yeh JC, Yang FJ, Kuo FJ, Wang HC. Change in flatfoot of preschool-aged children: a 1-year follow-up study. Eur J Pediatr 2013; 172: 255-60.
9. Faria A, Gabriel R , Abrantes J, Brás R, Moreira H. The relation of body mass index, age and triceps-surae musculotendinous stiffness with the foot arch structure of postmenopausal women. Clin Biomech (Bristol, Avon) 2010; 25: 588-93
10. Levinger P, Murley SG, Christian J, Barton JC, Cotchett PM, McSweeney RS, et al. A comparison of foot kinematics in people with normal- and flat-arched feet using the Oxford Foot Model. Gait Posture 2010; 32: 519-23.
11. Atamturk D. Relationship of flatfoot and high arch with main anthropometric variables. Acta Orthop Traumatol Turc 2009; 43: 254-9.
12. Lokumcu F, Yorgancioglu Z, Rezan, Ceceli E. The Relationship between flexible pesplanus and lower extremity rotational deformities in children. J Physical Med Rehab Sci 2003; 6: 11-5.
13. Pfeiffer M, Kotz R, Ledl T, Hauser G, Sluga M. Prevalence of flat foot in preschool-aged children. Pediatrics 2006; 118: 634-9
14. Nikolaidou ME, Boudolos DK. A footprint-based approach for the rational classification of foot types in young schoolchildren. The Foot 2006; 16: 82-90.
15. Mickle KJ, Steele JR, Munro BJ. Is the foot structure of preschool children moderated by gender? J Pediatr Orthop 2008; 28: 593-6.
16. Adoracio Villarroya M, Manuel Esquivel J, Tomas C, Buenafe´ A, Moreno L. Foot structure in overweight and obese children. Int J Pediatr Obes 2008; 3: 39-45.
17. Cetin A, Sevil S, Karaoglu L, Yucekaya B. Prevalence of flat foot among elementary school students in rural and urban areas and at suburbs in Anatolia. Eur J Orthop Surg Traumatol 2011; 21: 327-31.
18. Aktas N. Examination of foot structure of adult Turkish women and men with plantogram. Edirne 1991. 29-33. [not found]
19. PlumaromY, Imjaijitt W, Chaiphrom N. Comparison between Staheli Index on Harris mat footprint and talar first metatarsal angle for the diagnosis of flatfeet. J Med Assoc Thai 2014; 97: S131-5.
20. Gün K, Saridogan M, Uysal O. The correlation between footprint and radiographic measurements in flatfoot. Turk J Phys Med Rehab 2012: 58: 283-7.
21. Stavlas P, Grivas BT, Michas C, Vasiliadis E, Polyzois V. The evalution of foot morphology in children between 6 and 17 years of age: A cross-sectional study based on footprints in a Mediterranean population. J Foot Ankle Surg 2005; 44: 424-9.
22. Song J, Kane R, Tango ND, Veur SS, Furmato J, Komaroff E, et al. Effects of weight loss on foot structure and function in obese adults: A pilot randomized controlled trial. Gait Posture 2015; 41: 86-92.
23. Menz HB, Roddy E, Thomas E, Croft PR. Impact of hallux valgus severity on general and foot specific health-related quality of life. Arthritis Care Res (Hoboken) 2011; 63: 396-404.
24. Butterworth PA, Landorf KB, Smith SE, Menz HB. The association between body mass index and musculoskeletal foot disorders: A systematic review. Obes Rev 2012; 13: 630-42.
25. Aydog ST, Ozcakar L, Tetik O, Demirel HA, Hasçelik Z, Doral MN. Relationship between foot arch index and ankle strength in elite gymnasts: A preliminary study. Br J Sports Med 2005; 39: e13.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: