
Amna Faruqi ( Department of Physiology, Ziauddin University, Karachi, Pakistan. )
Syed Imran Ahmad ( Department of Cardiology, Ziauddin University, Karachi, Pakistan. )
Syed Tousif Ahmed ( Department of Physiology, Ziauddin University, Karachi, Pakistan. )
July 2016, Volume 66, Issue 7
Original Article
Abstract
Objective: To study QT parameters in Thalassaemia Major patients and their association with serum ferritin levels.
Methods: This cross-sectional study was conducted at Ziauddin University, Karachi, from February 2013 to September 2014, and comprised patients of Thalassaemia Major. Participants\\\' serum ferritin levels were determined and electrocardiography was performed. Data was analysed using SPSS 20.
Results: Of the 135 participants, 68(50.4%) were in the 7-14 years age group and 69(51%) were males. Significant prolongation of QT, corrected QT interval and increased QT dispersion was observed in patients with serum ferritin levels more than 2,500 nanogram/millilitre (p<0.001 each). These measurements of corrected QT and QT dispersion had a positive linear correlation with serum ferritin levels (r=0.760 and 0.786).
Conclusion: Electrocardiography could be a useful means for the pre-clinical detection of cardiac involvement due to iron overload in Thalassaemia Major patients.
Keywords: Thalassaemia major, TM, Iron overload, Cardiac iron, Ferritin, QT interval. (JPMA 66: 799; 2016)
Introduction
Beta Thalassaemia Major (TM) is an inherited disease in which the patient requires regular blood transfusions (BTs).1,2 As a consequence of repeated BTs, iron overload (IO) starts to take place.3 Deposition of iron in the heart leads to cardiac complications which are the main causes of death in such patients.4 A clinical evaluation of these patients is not useful to detect this pathology in its early phase because IO of the heart becomes clinically apparent only when sufficient damage to the heart has taken place. Magnetic resonance imaging (MRI) is the gold standard for pre-clinical detection of IO in the heart of patients who have an, otherwise, normal cardiac function.5 However, many countries, including Pakistan, do not have easy availability of cardiac MRI T2* facilities. And even if available, they are extremely costly and time consuming. Early detection of cardiac IO and early commencement or stepping up of chelating treatment is important for the health and
life of patients. Studies have been conducted to determine the usefulness of electrocardiography (ECG) in detecting cardiac IO, with variable results. In Pakistan, to the best of our knowledge, no study has been conducted on the electrocardiographically observed changes in Beta TM patients and their association with iron load.
The current study was planned to investigate a non-invasive, cost-effective and readily available method for the early detection of cardiac involvement due to IO, because once clinical manifestations of cardiomyopathy appears, it is not possible to reverse the damage that has occurred.
We electrocardiographically observed QT parameters and their association with serum ferritin levels.
Patients and Methods
This cross-sectional study was conducted at Ziauddin University, Karachi, Pakistan, from February 2013 to September 2014, and comprised diagnosed patients of Beta TM who were selected using simple random convenient sampling from the Fatimid Foundation, Karachi. Diagnosis was based on the usual haematological criteria of peripheral blood film and haemoglobin (Hb) electrophoresis. Minimum age was seven years. Patients were receiving at least eight BTs per year (defined as chronic current transfusion therapy6). Those who did not give consent, suffered any other haemoglobinopathy, acute illness, some known congenital or acquired heart disease(e.g. coronary artery disease, hypertension, congestive cardiac failure, arrthymias, heart blocks.), or were using drugs that lengthen the QT interval (e.g. antidepressants, antihistamines, antibiotics etc) were excluded. Patients who had used antiarrthymics (e.g. Amiodarone) in the preceding six months were also excluded, as were patients with thyroid, renal or severe liver disease, diabetes mellitus (DM) and bone-marrow (BM) transplantation. After getting approval from the institutional review committee, patients were studied just prior to receiving BT. History of the patients\\\' height, weight, pulse rate and blood pressure were all noted.
Electrocardiography was performed using ECG machine 901 (Zhuhai Kaden Yasen Medical Electronics Co., Ltd) at a paper speed of 25mm/sec. All intervals and axes were taken from standard ECG software and the intervals were double-checked manually by the principal investigator. Heart rate was calculated from the average RR interval of the lead II tracings.7 For each lead, three consecutive QT intervals were measured and averaged.3 QT dispersion (QTd), the difference between the longest and shortest QT intervals, was calculated.8 Corrected QT interval (QTc) was calculated using Bazett\\\'s formula (QTc =QT/pR-R interval).3,7,8
An analysis of serum ferritin was performed by Chemiluminescent Micro-particle Immuno-Assay (CMIA) technology using automatic immunoanalyser (ARCHITECT i2000SR; Abbott Laboratories). The normal range of serum ferritin (SF) was taken as 18-323 ng/ml.7
Severity of IO was defined by serum ferritin, which is the most commonly-used parameter for this purpose.9 Therefore, patients were divided into three groups. Group I had patients with SF< 2,500ng/ml; Group II had patients with SF levels ranging from 2,500-5,000ng/ml; and Group III had patients with SF>5,000ng/ml.
SPSS 20 was used for data analysis. For categorical variables, frequencies and percentages were calculated. For quantitative variables, mean with standard deviation was calculated, and Student\\\'s t-test was applied to determine significance. Pearson\\\'s correlation test was applied to study the association between SF, QTc and QTd. P<0.05 was considered significant.
Results
Of the 135 patients, who were aged between seven and 30 years, 68(50.4%) were in the 7-14 age group. Males constituted 69(51%) of the participants.
The mean ferritin level was 6062.61±3641.796ng/mL. There was no significant difference in terms of gender (p=0.366).
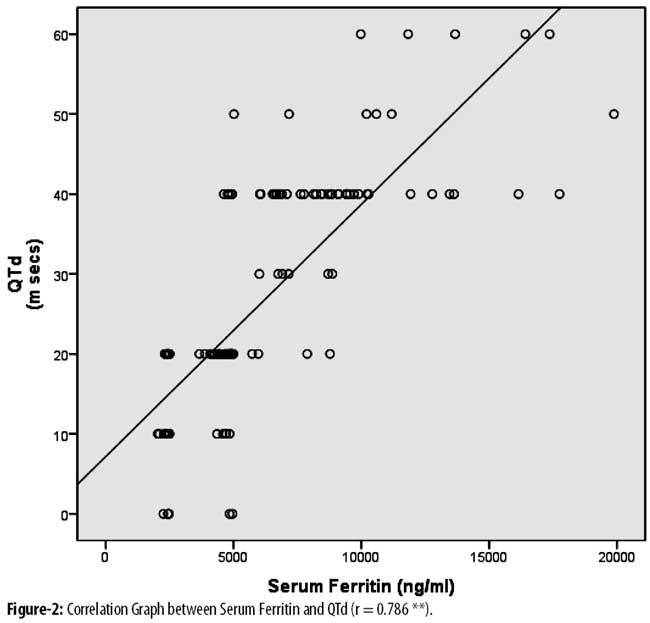
Group I included 33(24.5 %) patients; Group II 48(35.5%); and Group III comprised 54(40%) patients. QT, QTc and QTd were all significantly increased in Group II (p=0.0014; p=0.0001; p=0.0001) and Group III (p=0.0001 each) when compared with Group I (Table-1)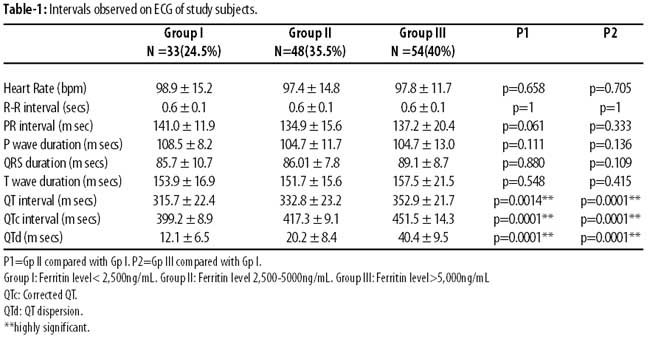
There was no significant difference in other intervals among the three groups (p>0.05). Moreover, increasing age was significantly associated with QT prolongation in females (p=0.025) (Table-2)
A significant positive linear relation was observed between SF level, QTc and QTd (p=0.01) (r=0.760 and r=0.786) (Figures-1,2)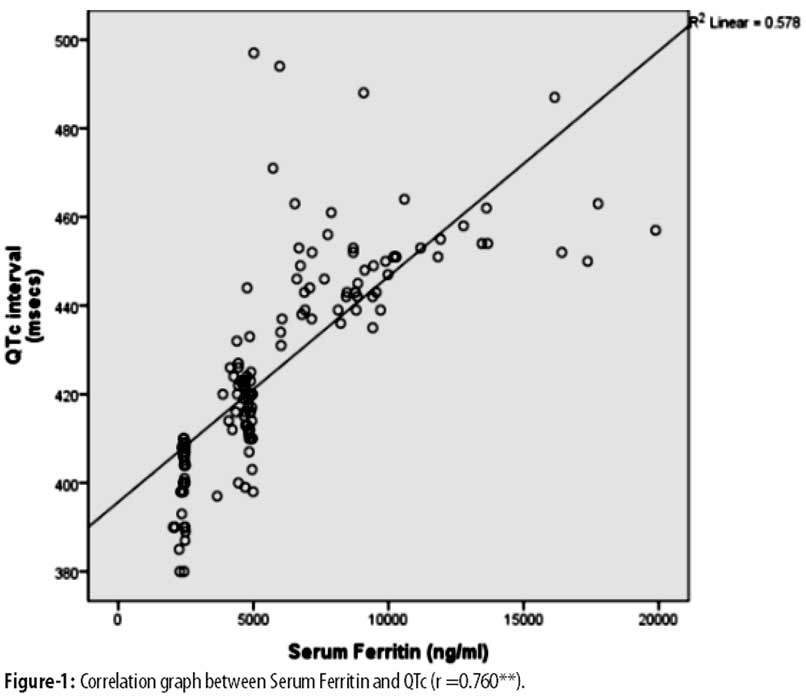
Discussion
Involvement of the heart in Beta TM is a significant problem which results in increased morbidity and mortality. Patients getting regular BT receive about 20 times the customary intake of iron. This excess is the main cause of subsequent damage to the heart, endocrines, liver and other organ tissues.7
TM patients show a markedly poor survival rate after the first decade of life.10,11 Similar results were obtained in ours and some previous studies.11,12 A better prognosis for survival without cardiac disease is seen in TM patients receiving regular BT, in which SF levels remain below 2,500ng/ml.13 The mean SF of our subjects was higher than that recorded in other studies and this may be the possible reason for the increased frequency of cardiac complications in our population and lower life expectancy. Lower mean SF levels have been recorded in various studies.1,11,14 The high mean SF of our study sample may be due to the difference in the standard of health care being provided to our patients, non-affordability of chelation therapy by many, and a poor availability of infusion pumps. However, a study conducted in India recorded a much higher level.15
The QT interval is a means of identifying ventricular depolarisation and repolarisation. Its prolongation predicts a higher risk of fatal arrthymias and sudden demise.1 High intracellular iron causes disturbance in the function of the sodium channels responsible for the upstroke (depolarisation) of the cardiac action potential. On the other hand, the delayed rectifier potassium and calcium channel modification may be responsible for repolarisation abnormalities.9,16
QTd is representative of variability of ventricular repolarization17 and is an indicator of non-homogeneity of the myocardial repolarisation.7 An increased QTd value is a predictor of cardiac morbidity and mortality.6 In addition to causing dysfunction of ion channels, iron deposition in the myocytes also causes them to hypertrophy, and become ischaemic.18 This iron deposition followed by fibrosis is seen to occur in a non-uniform pattern in the heart, causing the myocardium to lose its homogeneity and be reflected as an increased QTd.19
In our study, prolongation of QT and QTc and an increase in QTd was observed in patients with high SF levels. These results were in accordance with previous studies.3,6,7,18,20,21
However, two studies apparently showed conflicting results,1,8 noting that conventional QT and dispersion parameters were prolonged in TM patients as compared to the controls, but statistical significance was not observed. A plausible explanation may be that since their patient group had a mean SF level well below the internationally accepted prognostic cut-off value of 2,500ng/mL,10 it was probably not high enough to produce significant changes in QT, QTc and QTd. Therefore, we may conclude that the results obtained in these studies were in accordance with our lowest SF group. Although the SF level in that group was higher than these two previous studies, it was still below the prognostic cut-off point, hence did not show QT prolongation like our higher SF groups.
Our study demonstrated a highly significant, positive linear correlation between SF level, QTc and QTd, showing that increasing SF levels may lead to greater level of iron deposition in the heart, ultimately giving rise to increasing extent of cardiac involvement. Previous studies concur with these results.5,7,21
One of the limitations of our study was a small sample size, Moreover, due to budgetary constraints, we did not have an age- and gender-matched healthy control group.
Conclusion
Significant QT changes which correlated strongly with SF levels maybe indicative of early cardiac iron deposition. ECG could serve as a useful means for preclinical detection and monitoring of cardiac complications in patients of TM.
Acknowledgements
We are grateful to Dr Farah Ahmed statistical assistance, and to Principal Investigator Dr Amna Faruqi for financial assistance.
Disclosures: None.
Conflict of Interest: None.
Funding: None.
References
1. Farahani B, Abbasi M , Khaheshi I, Paydary K. "Evaluation of QT interval in b thalassemia major patients in comparison with control group." Heart views. 2012; 13: 42-45.
2. Ansari S, Shamsi T, Ashraf M, Bohray M, Farzana T, Khan T, et al. "Molecular epidemiology of b-thalassemia in Pakistan: far reaching implications." Int J MolEpidemiol Genet. 2011; 2: 403-408.
3. Kayrak M, Acar K, Gul E, Ozbek O, Abdulhalikov T, Sonmez O, et al. "The Association between Myocardial Iron Load and Ventricular Repolarization Parameters in Asymptomatic Beta-Thalassemia Patients." Advanchematol. 2012 (2012). Article ID 170510.6 pages.
4. Wood J. "Cardiac iron across different transfusion-dependent diseases." Blood rev. 2008; 22: 14-21.
5. Quraishi M, Lawson S, Gill P. "Electrocardiography as a prognostic tool for identifying the development of heart failure in patients with b-thalassaemia: a retrospective cohort study." Prim Care Cardivasc J. 2008; 1: 51-4
6. Detterich J, Noetzli L, Dorey F, Bar-Cohen Y, Harmatz P, Coates T, et al. "Electrocardiographic consequences of cardiac iron overload in thalassemia major." Am J Hematol. 2012; 87: 139-144.
7. Sayed S, Aly B, El-Hakim A, Omar S, Amin A. "The early cardiac involvement in patients with b-thalassemia major." Egypt Heart J. 2013; 65: 243-249.
8. Garadah T, Kassab S, Mahdi N, Abu-Taleb A, &Jamsheer A. "QTc interval and QT dispersion in patients with thalassemia major: electrocardiographic (EKG) and echocardiographic evaluation." Clin Med Insights Cardiol. 2010; 4: 31-37.
9. Lekawanvijit S., Chattipakorn N. "Iron overload thalassemic cardiomyopathy: iron status assessment and mechanisms of mechanical and electrical disturbance due to iron toxicity." Can J Cardiol. 2009; 25: 213-218.
10. Borgna-Pignatti C, Rugolotto S, Stefano P, Zhao H, Cappellini MD, Vecchio GC, et al. "Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine." Haematologica. 2004; 89: 1187-1193.
11. Riaz H, Riaz T, Khan MU, Aziz S, Faizan-ullah, Rehman A, et al. "Serum ferritin levels, socio-demographic factors and desferrioxamine therapy in multi-transfused thalassemia major patients at a government tertiary care hospital of Karachi, Pakistan. BMC Res Notes 2011; 4: 287-91.
12. Mohammad SJ, Al-Lami FH , Hussein MQ .Electrocardiographic changes among beta-thalassemic major patients in ibn al-baladi thalassemia center-Baghdad. Al - Kindy Col Med J 2013; 9: 36-42.
13. Olivieri NF, Nathan DG, MacMillan JH, Wayne AS, Liu PP, McGee A, et al. Survival in medically treated patients with homozygous ?-thalassemia. N Engl J Med 1994; 331: 574-8.
14. Ikram N, Hassan K., Younas M, Amanat S. Ferritin levels in patients of Beta Thalassemia major. Int J Pathol 2004; 2: 71-4.
15. Choudhry VP, Pattit HP, Saxena A, Maiaviya AN. Deferiprone, efficacy and safety. Indian J Pediat 2004; 71: 213-6.
16. Aessopos A, Berdoukas V, Tsironi M. The heart in transfusion dependent homozygous thalassaemia today-prediction, prevention and management. Eur J Haematol 2008; 80: 93-106
17. Ulger Z, Aydinok Y, Levent E, Gurses D, Ozyurek AR. Evaluation of QT dispersion in b thalassaemia major patients. Am J Hematol 2006;81: 901-6.
18. Kolnagou A, Yazman D, Economides C, Eracleous E, Kontoghiorghes GJ. Uses and limitations of serum ferritin, magnetic resonance imaging T2 and T2* in the diagnosis of iron overload and in the ferrikinetics of normalization of the iron stores in thalassemia using the International Committee on Chelation deferiprone/deferoxamine combination protocol. Hemoglobin 2009; 33: 312-22.
19. Pepe, A, Positano V, Capra M, Maggio A, Pinto C, Spasiano A, et al. Myocardial scarring by delayed enhancement cardiovascular magnetic resonance in thalassaemia major. Heart 2009; 95: 1688-93.
20. Russo V, Rago A, Panone B, Papa AA, Di Meo F, Mayer MC, et al. Dispersion of repolarization and beta?thalassemia major: the prognostic role of QT and JT dispersion for identifying the high?risk patients for sudden death. Eur J Haematol 2011; 86: 324-31.
21. Laudanski K., Ali H, Himmel A, Godula K, Stettmeier M, Calvocoressi L. The relationship between serum ferritin levels and electrocardiogram characteristics in acutely ill patients. Exp Clin Cardiol 2009; 14: 38-41.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: