
William W. T. Manser ( Department of Biochemistzy, The Aga Khan University Medical College, Karachi. )
M. Altaf Khan ( Department of Microbiology, Karachi University, Karachi. )
K. Zaki Hasan ( Baqai Medical College, Karachi. )
October 1989, Volume 39, Issue 10
Original Article
Abstract
Blood copper, zinc, magnesium and lead levels were determined by atomic absorption spectroscopy for 15 males and 16 females suffering from depression, 6 males and 1 female with mental retardation and 3 males and 4 females with seizure disorders. They were all under no medication and belonged to low income groups. No difference in copper levels was found between the sexes in any of the groups. The levels in all the groups were significantly higherthan in the normals. In depressives, males had significantly higher zinc levels than females and only female depressives had significantly different (lower) levels from normals. In both depressives and normals, males had higher magnesium levels than females but no group of patients had significantly different levels from normals. Lead levels were significantly higher in female depressives and for those with seizure disorders than for controls. At least one metal abnormality was found in 21(67.7%) depressive, 5 (71.4%) of those with mental retardation and 6 (85.7%) with seizure disorders (JPMA 39 : 269, 1989).
INTRODUCTION
Lead is associated with a whole host of neurological, physiological and behavioural problems, and some of the important points concerning these have been briefly discussed previously1. In cases of depression one would expect blood copper levels to be the opposite to those in hyperexcitability2, namely, that these levels should be lower than normal. Both high3 and low levels2,4 have been reported for schizophrenics. For mental retardation,wehavefoundnoliterature references but in those with seizure disorders excitory neurotransmitter functions dominate and copper levels should be raised2. On the basis of high zinc levels being associated with hyperexcitability2, depression should predictably be associated with zinc deficiency. In fact, this has been found not only for depression4 but also for thought disorders and schizophrenia3,4 and also in neuronal undevelopment due to maternal or infant malnutrition2. Seizure disorder cases would be expected to have high zinc levels2. Raised blood levels of magnesium are associated with CNS depression4 and schizophrenias have variously been reported as being associated with either high5,6, low7 or normal levels8,9. We have found nothing reported for those with mental retardation, but those with seizure disorders should have low levels4. We have found no satisfactory explanation in the literatureas to how these metal abnormalities are connected to the disease states.
MATERIALS, EQUIPMENT AND METHOD
Estimation of copper, zinc and magnesium on whole blood was by atomic absorption spectroscopy, and details of the method and selection of control subjects has been described in Part I of this series10. Lead was estimated similarly to copper and zinc.
Patients
Patients belonged to the low income groups attending the outpatients neuropsychiatric clinic at the Jinnah Postgraduate Medical Centre, Karachi for the first time. They were under no medication at the time of blood sampling. They were of three categories, those suffering from depression (15 males and 16 females), those with mental retardation (6 males and one female), and those suffering from seizure disorders (3 males and 4 females). As the second and third groups were small, results for these were not considered by sex.
Statistical Analysis
Distribution of metal levels in every case was non-Gaussian. Therefore the Student’s ‘t’ test for significance of difference was invalid and the Wilcoxon Rank Sum Test was used. Regression analysis was performed as previously.10
RESULTS
Relevant information concerning blood levels of copper, zinc and magnesium for the patients is given in Tables I-VI
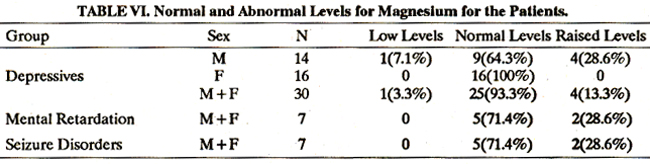
together with that for the normal subjects reported previoussly.10 Ten (5 males, 5 females) of the 31 patients (32.3%) with depression had no blood metal abnormality (Table VII)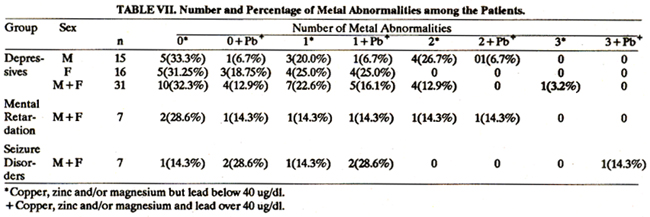
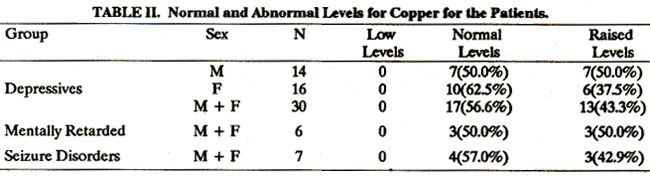
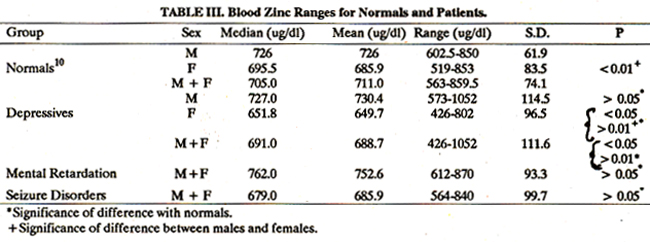
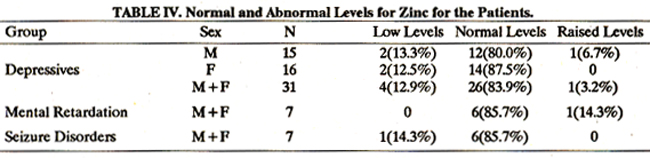
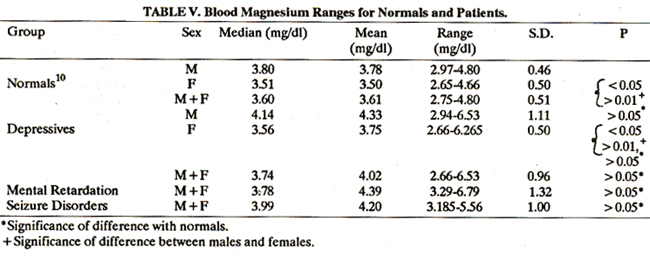
and 21 (10 males, 11 females) or 67.7% had at least one. Four patients (1 male, 3 females) or 12.9% had lead levels of 40 ug/dl or over with no other metal abnormality and five (1 male, 4 females) or 16.1% had lead plus one other metal abnormality. One male had three metal abnormalities: copper, zinc and magnesium. Lead levels of 40 ug/dl or over were taken as “abnormal”, although levels of over 25 ug/dl should really be regarded as "elevated"11. For other metals, “abnormal” meant a high or low blood level Of the seven patients with mental retardation, two (28.6%) had no metal abnormality, five (71.4%) had at least one abnormality including one (14.3%) with an abnormal lead level only and two others with lead plus at least one other metal abnormality. Of the seven with seizure disorders, the corresponding figures were one (14.3%), six (85.7%), two (28.6%) and three (42.9%) respectively. The levels of all four metals were abnormal in one male. As in the normals, there was no significant difference in blood copper levels between the sexes in the depressive group. Levels were significantly higher, as were those with mental retardation (p < 0.01) and with seizure disorders (0.05> p >0.01) than the normals (Tables land!!). Male depressives had significantly higher zinc levels than female patients (0.05> p >0.01) as in normals (Tables III and IV). There was no significant difference in the levels between male patients and normal males but levels for female, and male and female patients combined were significantly lower than for the corresponding normals (0.05> p >0.01). For mental retardation and seizure disorders, levels were not significantly different to those of normals. Male depressives had significantly higher blood magnesium levels than female patients (0.05 > p >0.01) as in normals (Table V and VI) but there was no significant difference bysex between patients and normals. Levels were not significantly different to normals in mental retardation and seizure disorders. Females in the depressives group had higher lead levels than males (p = 0.05). There was no significant difference between the levels for male patients and controls, but female patients had higher levels than the corresponding controls (0.05> p >0.01) as did males and females combined (p = 0.05). Eight (2 males, 6 females) of the 31 patients (25.8%) had abnormal levels (at or above 40 ug/dl). The 7 patients with mental retardation did not have significantly higher levels than controls, although 3 males (42.9% of the total) had abnormal levels. Levels were significantly higher for the 7 with seizure disorders (p = 0.01) and 2 males and 3 females (71.4% of the total) had abnormal levels. Regression analysis was carried out as previously1° results being in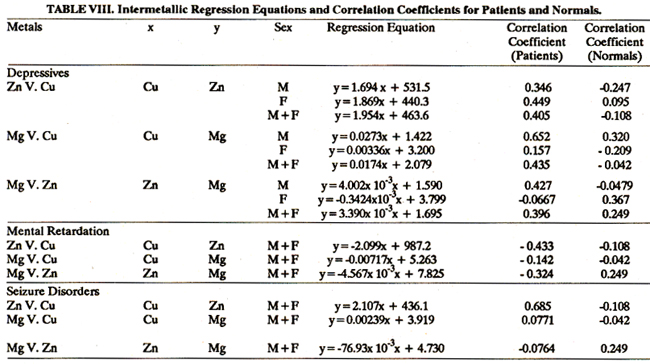
Table VIII and metal abnormalities on an individual basis and grouped accordingto diagnosis or manifestations of disease arc in Table IX.
DISCUSSION
Contrary to expectations2 (see introduction), blood copper levels for the depressives group of patients were significantly higher than those found previously10 for normals (Table I & II). In fact, no patient bad a low level and 13 (7 males and 6 females) of the 31(41.9%) had raised levels. Males had significantly higher zinc levels than females as in normals, but only females had the expected lower levels than normals, as in the literature2. Two males and two females had low levels but one male bad a raised level (Tables III & IV). There was no significant difference from normals in blood magnesium levels although 4 males had the expected raised levels (Table V & VI) as in the literature4. Blood lead levels were significantly higher for females than males, which was the opposite in the controls, but only female patients had higher levels than the corresponding controls. Among the patients, only2males(13.4%) but 6 females (373%), a total of 8 (25.8%) had abnormal levels whereas in the controls there were 10 males (303%) and only 3 females (10.3%) or 21.0% of the 62 subjects. The seven patients with mental retardation had significantly higher blood copper levels than normals, three of them having raised levels. Zinc and magnesium levels were not significantly different from normals, tower levels of the former being expected, according to previous reports2. No one had a low zinc level; in fact, one had a raised level. Two had raised magnesium levels. Although 3 males had abnormal blood lead levels, overall, levels were not significantly different from con-trots. The seven seizure disorders patients had significantly higher copper levels, as in the literature2, three having raised levels. However, levels of zinc and magnesium were not significantly different from normals as previously reported2,4. No individual had the expected raisedzinc level and, in fact, one had a low level. Two had raised magnesium levels and not one had the expected low level. Blood lead levels were significantly higher than for controls, with 2 males and 3 females (71.4% of patients) being abnormal. The intermetallic correlation coefficient (r, Table VIII) was significant for magnesium versus copper for male depressives and for zinc V. copper for seizure disorders. Also of note was the fact that for zinc V. copper it was positive for depressives (both sexes) and in seizure disorders, whereas for male normals10 and in previous reports12 the coefficient was negative. Consideration of the results on a more individual patient basis (Table IX) reveals that among the patients suffering from depression two of three females in the depressive phase of manic depressive illness had the expected metal abnormalities but one had a raised copper level in disagreement with the literature concerning depression2. One of two males with schizophrenia with depression had a low zinc level as in previous reports3,4, but one malewith psychomotor retardation bad a raised copper level. Two females had no metal abnormality. The remainder of the depressives had either not been admitted to the wards or had discharged themselves before a diagnosis had been completed and were therefore categorised according to their presenting conditions or manifestations. Six males and two females exhibited according to their presenting conditions or manifestations. Six males and two females exhibited lethargy, lack of interest and/or headaches. All except two of the males had metal abnormalities, the two females and three of the males havingmetal abnormalities which included raised copper levels. One of the males had raised magnesium (expectcd4)and raised zinc levels (unexpected2) in addition. One female, in addition to a raised blood copper level, had a lead level of 74.7 ug/dl. Two of three male and one of two female agitated depressives had no metal abnormality. However, the remaining male had raised copper and zinc levels and the female a lead level of 290.3 ug/dl. Three males and seven females were quiet, withdrawn or suffered from weeping spells. Two of the females had no metal abnormalities, but the other patients had abnormalities including two males and three females with raised copper levels and one male with a low magnesium level (unexpected4). A total of 21 of the 31 patients in the depressives group (67.7%) had at least one metal abnormality but only seven of these (33.3% of abnormal cases or 22.6% of the total number of patients) had abnormalities totally in agreement with reports in the literature2-4. Of those with mental retardation one out of six males and the only female had no abnormality and, of note, one male had raised blood copper, zinc and lead levels, that of zinc being unexpecteth, for mental retardation. In all, five (71.4%) of the seven patients had at least one metal abnormality. Three males and four females were having seizure disorders. One female had no metal abnormality and out of the remainder one male had a raised magnesium level and another, had raised copper, magnesium and lead levels and a low zinc level. The magnesium and zinc results were contraryto previous reports concerning seizure disorders2,4. Two females had lead levels of 53.7 and 74.7 ug/dl. In all, six of the seven patients (83.7%) had at least one metal abnormality of which four (66.7% of abnormal cases or 57.1% of the total) had results agreeing with the literature. In summary, psychiatric disease is accompanied by blood metal abnormalities and many of our results, especially for blood coppr levels in depressives are contrary to those previously reported24. As yet we do not knowwhich is the cause and which the effect. One metal abnormality can cause another13, which may be happening here in some cases, and it is known that lead is often taken up more readily and has more serious results in those in low socioeconomic groups14 such as we have here.
ACKNOWLEDGEMENTS
Thanks are due to the Aga Khan University Medical College for a grant in support of this research and to Ms. Seema Mohamedi for typing this report. Thanks also go to Dr. M. Hussain and to the many postgraduate students at the outpatients neuropsychiatric clinic, J.P.M.C., Karachi, who enabled us to collect blood specimens and who supplied us with the diagnostic information and personal details of the patients.
REFERENCES
1. Manser, W.W.T., Altaf Khan, M. and Zaki Hasan, K. Trace element studies in Karachi populations, Part III" Blood copper, zinc, magnesium and lead levels in psychiatric patients with disturbed behaviour. JPMA., 1989; 39: 235.
2. Bryce-Smith, D. John Jaye’s Lecture: Environmental chemical influence on behaviour and mentation. Chem. Soc. Rcvs., 1986; 15: 93.
3. Srinivasan, D.P. Trace elements in psychiatric illness. Br. J. Hosp. Med., 1984; 32: 77.
4. Linter, G.M. Neuropsychiatric aspects of trace elements. Br. J. Hosp. Med., 1985; 34: 361.
5. Cade, J.F.J. A significant elevation of plasma magnesium level in schizophrenia and depressive states. Med. J. Australia, 1964; 1: 195.
6. Chugh, J.D., Dhingra, R.K., Gulali, R.G. and Bathia,J.C. Magnesium in schizophrenia. Indian J. Med. Res., 1973; 61: 998-1001.
7. Chhatre, S.M., Ganeriwal, S.K. and Reddy, B.V. Serum magnesium levels in schizophrenia. Ind. J. Med. Sci., 1985; 39: 259-261.
8. Pandey, S.K., Devpura, J.C., Badi, H.K. and Babel, C.S. An estimation of magnesium and calcium in serum and C.S.F. in schizophrenia. J. Assn. Phys. Ind., 1973; 21:201-205.
9. Paul, E.A., Daniel, P., Vankamen, W.E. and Bunney,J.R. Serum calcium and magnesium in schizophrenia: Relationship to clinical phenomena and neuroleptic treatment. Br. J. Psych., 1978; 133: 143-149.
10. Manser, W.W.T. and Altaf Khan, M. Trace element studies in Karachi populations, Part I: Normal ranges for blood copper, zinc, and magnesium for adults. JPMA., 1989; 39: 4349.
11. Centre for Disease Control, Preventing lead poisoning in young children. Atlanta: U.S. Department of Health and Human Services, 1985.
12. Festa, M.D., Anderson, It.L., Dowdy, R.P. and Ellerstecky, M.R. Effect of zinc intake on copper excretion and retention in men. Am. J. Clin. Nutr., 1985; 41: 285-292.
13. Watson, W.S. et at. Food iron and lead absorption in humans. Am. J. Clin. Nutr., 1986; 44: 248-257.
14. Winneke, G. and Kraemer, U. Neuropsychological effects of lead in children: interaction with social background variables. Neuropsychobiology, 1984; 11: 195.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: