
Masood Hameed Khan ( Department of Medicine, Medical Unit-3, Civil Hospital, Karachi. )
Rana Qamar ( Department of Medicine, Medical Unit-3, Civil Hospital, Karachi. )
Zaman Shaikh ( Department of Medicine, Medical Unit-3, Civil Hospital, Karachi. )
October 1989, Volume 39, Issue 10
Original Article
Abstract
Serological test based on HA (Indirect Haemagglutination Method) was performed in 100 cases of hepatic abscess. The test was 100% sensitive and 94% specific. The cut off point of antibody titer between normal population and patients with invasive amoebiasis was 1:128. Antibodytiter in amoebic liver abscess was 1:5242 ±2795. A significant (P <0.001) correlation was found between total leucocyte count and antibody titer (JPMA 39: 262, 1989).
INTRODUCTION
Entamoeba histolytica infection is a common problem especially in third World Countries. It is very common in ill-sanitised areas, particularly in warm climate of the tropical and sub-tropical countries, due to poor socio-economic conditions, poor nutrition and hygiene. After intestinal amoebiasis liver abscess is the commonest form of invasive amoebiasis, occurring in about 83% of patients with intestinal amoebiasis1. Often it is difficult to distinguish pyogenic from amoebic liver abscess clinically and by laboratory and imaging techniques. Serological tests are of great help in the diagnosis of invasive amoebiasis.In the prescnt study an attempt has been made to assess the efficacy and sensitivity of serological test and antiamoebic antibody titers in patients with invasive amoebiasis.
PATIENTS AND METHODS
Hundred patients with liver abscess were studied. Liver abscess was diagnosed clinically, on ultrasonography, aspiration and serological test for amoebiasis. Patients with liver abscess were interrogated in detail and examined thoroughly. Their Sera were stored at -4°C for indirect haemagglutination test (IHA). These patients were reexamined after three weeks for clinical, laboratory, ultrasonographic and serological parameters. Hundred aged matched healthy individuals from various socio economic classes were included in the study as controls. The controls were also subjected to similar examination and investigation and their sera were stored for estimation of antibody by using cellognost amoebiasis - kit. The reagent is available in lyophilized form, and is stable at 2-8°C, for upto 4weeks after preparation. Keepinginview the short stability of the reagent, sera of these cases and controls were stored and test was performed on two consecutive days. Statistical analysis was done by Chi square and students ‘C test.
RESULTS
Out of 100 cases of liver abscess, 96 had amoebic and 4 had pyogenie liver abscess. There were 80 males and 20 females in control group with mean age of 40.44 ± 12.9 years. In amoebic liver abscess out of 96 I 82(85.4%) were males and 14 (14.6%) were females. Serological test was performed in all the 96 eases of amoebic liver abscess, in which anti-amoebic antibody titers were very high. In the control group these titers were below 1:128 except in six cases in whom the titers were above threshold i.e. 1:128. In these six cases there was history of. loose motions during the previous six months. Hence the increased titers might be due to invasive intestinal amoebiasis. The mean value of antiamoebie antibody titer in the control group, pyogenic group and amoebic group was 1 :71 ± 17.8, 1 : 64, 1 : 5242:88 ± 2795 respectively. A significant correlation (P <0.001) was found between total leucocyte count and antibody titer (Table).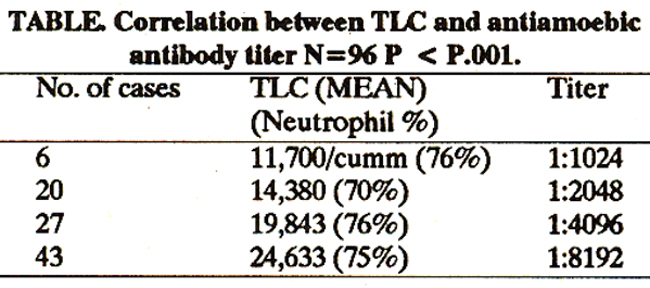
The sensitivity and specificity of the IHA test in the present study was 100% and 94% respectively.
DISCUSSION
It is difficult to differentiate amoebic from pyogenic liver abscess on clinical fmdings, laboratoryinvestigations and imaging techniques. Though aspiration and examination of the pus is very helpful in differentiating between the two disease processes, it is not always feasible especially when the abscess involves the left lobe of the liver. In the present study, 100% of the cases with amoebic liver abscess had neutrophilleucocytosis, while 18% had two or more abscess. These two fmdings were once considered to be the most reliable for diagnosis of pyogenic liver abscess. Moreover, trophozoites are not easy to fmd the liver “pus”. Therefore, the diagnosis of Amoebic Liver Abscess cannot be made with certainty by such conventional methods. Confirmation of diagnosis requires either isolation of trophozoites from pus or by serological tests for amoebiasis. Various serological tests for invasive amoebiasis have been introducedwith variable sensitivity, specificity and reproducibility. Of these IHA is the most widely used test in many centers of the world and has also been employed in the present study. It is highly sensitive non-invasive and cost effective. Attempts have been made to isolate amoebic antigen in the purified form from monoxenic culture of Entamoeba histolytica. 2-5 These workers introduced the antigenic system ofexenicEnt. histolytica (NIH20 strain) to characterize the immunological specificities of various isolated factions. They reported their reproducible results of gel filtration of crude axenic extract. In all, three fractions (Fi, P11 and Fill) were obtained. Antisera against each fractions and whole antigen were raised in rabbits. Serological tests employing pun-fled antigens are positive in nearly all patients with proven amoebic liver abscess and in great majority of those with acute amoebic dysentery. They are generally negative in asymptomatic cyst passers, suggesting that tissue invasion is necessary for antibod; production, which has been confirmed earlier. 6 Failure to detect antibodies probably indicates that invasion has not taken place and this maybe the best means of separating the commensals from the invasive infection in individuals passing cysts. Thus it is also evident that serology, particularly in the endemic area is of more value in excluding the diagnosis than in confirming it, since the persistence of significant antibody titer for months after complete cure. Many workers throughout the world have done research in this particular field and confirmed the efficacy of serodiagnosis in invasive amoebiasis.7-14 Hence, considering the sensitivity, specificity and cost effectiveness of serodiagnbsis of amoebiasiis by IHA, we recommend its routine use and further recommend that the cut off point should be taken as 1: 128 for the test.
REFERENCES
1. Ralls, P.W>, Colletti, P.M., Quinn, M.F. and Halls, J. Sonographic findings in hepatic amoebic abscess. Radiology, 1982; 145:123.
2. Alam, M. and Ahmed, S. Studies on the antigenicity of Ent.histo lytica antigen fractions,proceedingsofthesymposium on central mechanism in cellular processes. Bombay, Bhabha Atomic Research Centre, 1973, P.74.
3. Khan, Z.A> and Meerovitch, E A comparative study of the antigens of some of the "histolytica-type" strains of Entamoeba. A qualitative quantitative evaluation of antigens by indirect hemagglutination, gel-precipitation, and immunoelectrophoresis. Am. J. Trop. Med. Hyg., 1968; 17: 528.
4. Krup, LM. Comparison of CIEP with other serologic tests in the diagnosis of amoebiasis. Am. J. Trop. Med. Hyg., 1974; 23:27.
5. Sawhney, S., Chakravarti, RN., Jam, P. and Vinayak, V.K. Immunogenicity of exenic Entamoeba histolytica antigen and its fractions. Trans. It Soc. Trop. Med. Hyg., 1980 74:26.
6. Nanda, It, Baveja, U. and Anand, B.S. Entamoeba histolytica cyst passers; clinical features and outcome in untreated subjects. Lancet, 1984; 2:301.
7. Harrison,H.R,Crowc, CP. and Pulginiti, V.A. Amoebic liver abscess in children; clinical and epidemiological features. Pediatrics, 1979; 64:932.
8. Hartmann, D.P., Ghadirian, E. and Meerovitch, a Enzyme-linked immunosorbent assay (ELISA) and indirect hemagglutination (IHA) test in the serodiagnosis of aperimental hepatic amoebiasis. 1. Parasitot., 198% 66:344.
9. Bos, HJ., Schouten, WJ., Noordpool, H.; Makbin, M. and Oostburg, B.F.Aseroepidemiologicalstudyofamoebiasis in Surinam bythe enzyme-linked immunosorbent assay (BLISA). Am. J. Trop. Med. Hyg., 198% 2% 358.
10. Tandon, A. Use of enzyme linked immunosorbent assay in intestinal and extraintestinal amoebiasis (amoebic liver abscess). Trans. It. Soc. Trop. Med. Hyg., 1981; 75:574.
11. Agarwal, S.S.., Sharma, P., Das, P., Ahmad, J. and Dutta, 62. Micro-enzyme linked immunosoibent assay for serodiagnosis of amoebiasis. Indian J. Med. Rca., 1981; 74:219.
12. Price, M.E. Amoebic liver abscess in a Norfolk factoiy worker. Br. Med. J. (Clin Res.), 1981; 283:1175.
13. Katzenstein, D., Rickerson, V. and Braude, A. New con. cepts of amoebic liver abscess derived from hepatic imaging, serodiagnosis, and hepatic enzymes in 67 consecutive cases in San Diego. Medicine (Bait.), 1982; 61: 237.
14. Oyeyinka, 0.0. and Onyemeiukwe, G.C. Amoebic liver abscess; serum immunogiobulins and complement in Northern Nigerian patients. Ann. Trop. Med. Parasitol., 1983; 77:293.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: