
N. K. Mahdi ( Departments of Microbiology, College of Medicine, University of Basrah, Iraq. )
F. Al-Obaidi ( Departments of Surgery, College of Medicine, University of Basrah, Iraq. )
A.Z. Benyan ( Departments of Surgery, College of Medicine, University of Basrah, Iraq. )
October 1989, Volume 39, Issue 10
Original Article
Abstract
Hepatic abscess was studied in 21 established cases in Basrah hospitals (Southern Iraq) during 1985 to 1988. Age of patients varied from 19 to 60 years. There were 7 females and 14 males and most of them from urban areas. All patients had a single abscess and the common site affected was the right lobe. Microorganisms isolated from 19 patients included a variety of aerobic and anaerobic bacteria and a protozoan Entamoeba histo/ytica. Escherichia co/i was the most common etiologic agent for the pyogenic abscesses. Therapy was a combination of an open surgical drainage and antimicrobial agents. Usually the drug regimen included metronidazole in combination with either tetracycline, ampicillin or gentamicin. No mortality was recorded on a long-term sequelae (JPMA 39: 259, 1989).
INTRODUCTION
Hepatic abscesses have an invariably fatal outcome in untreated cases1-3. They figure prominently in the diagnosis of upper abdominal illness. Therefore, surgeons have maintained an active interest in differential diagnosis, principles of treatment and indications for surgical intervention. Open surgical drainage and antimicrobial agents4 have improved the prognosis, but are still associated with high mortality. After the introduction of ultrasound along with modern surgical and antimicrobial treatments, the operative mortality dropped to 5-9% for solitary hepatic abscess5,6due to its significant impact on both diagnosis and treatment. There has also been an increased recognition that anaerobes play an important role in this condition1,4,7,8. Metronidazole, an agent that is amoebicidal and bactericidal is now being recommended for the treatment5,9. Accordingly, we present an analysis of a recent series of Iraqi patients with hepatic abscess for the first time. It is an attempt to delineate the clinical setting, the most useful diagnostic clues and the current 4pproach to therapy.
PATIENTS AND METHODS
From 1985 to 1988, 21 cases of hepatic abscess were diagnosed, operated and treated by chemotherapy in Basrah hospitals (Southern Iraq). Informed consent was obtained in all patients. The clinical details were recorded. The admitting diagnosis was based on the clinical presentation, mostly fever, abdominal pain and enlarged tender liver. The diagnosis was confirmed by x-ray, ultrasonography and laparotomy. In order to facilitate the isolation of the microorganisms, gram-stain, aerobic and anaerobic cultures of the aspirate were carried out. Open surgical drainage was performed for all patients and adjuvant antimicrobial agents were given.
RESULTS
Twenty one patients were diagnosed, operated and treated for hepatic abscess. There were 7 females and 14 males; 8 from rural and 13 from urban localities (Table 1).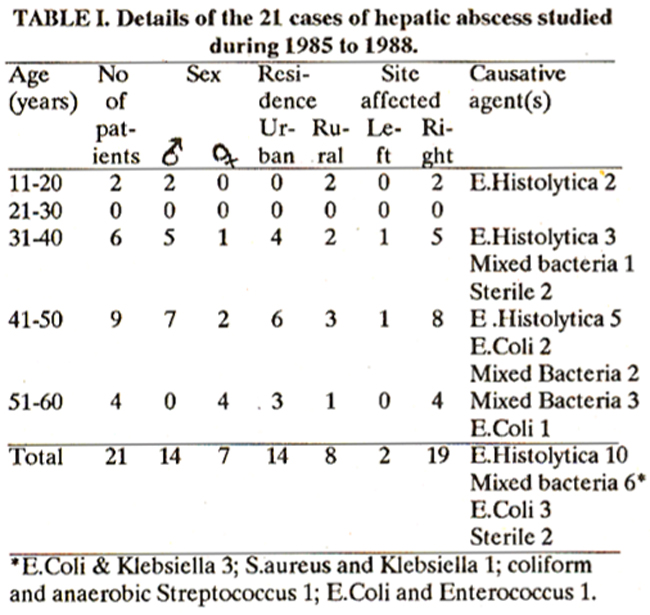
The mean ± SD age was 41.6 ± 10.1 years, with a range of 19 to 60 years. All patients had a single focus of infection. Symptoms and signs included fever and right upper abdominal pain (Table II).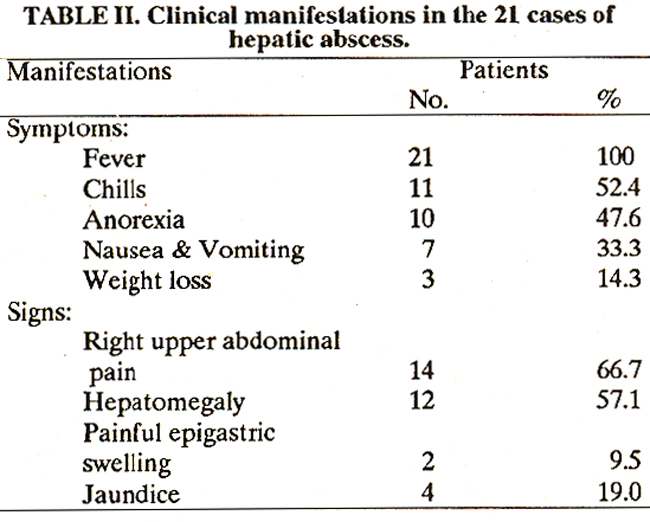
Fever was noticed in 100% of patients. Left lobe abscess presents as a painful epigastric swelling. Tender hepatomegaly was an almost constant feature. Microbiological data are presented in Table I. All patients underwent an open surgical drainage in combination with antimicrobial administration. A variety of antimicrobial agents were given, the choice depending on the sensitivity of the isolated microorganism. Metronidazole was administered in combination with either tetracycline, ampicillin or gentamicin (Table III).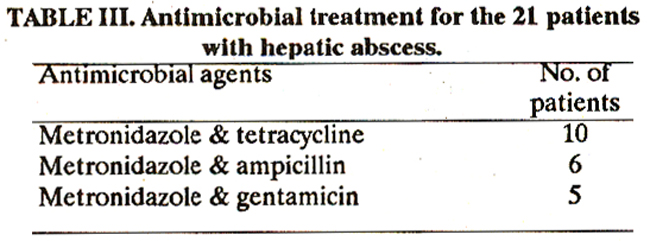
There were no deaths or long-term sequelae.
DISCUSSION
Twenty one patients, seen in this study, underscore the key features of epidemiology, clinical presentation, causative agents and treatment. Hepatic abscess presented as an acute abdominal illness. Most of the patients were Iraqi males in the age group of 41-50 years, confirming the findings of others5,6,10-12. Interestingly, there was no case in the age group of 21-30 years which is difficult to explain. However, other workers have pointed out that there is no predilection of either sex and the highest percentage of progenic abscesses occurs in the age over 55 years. 8,11 The admitting diagnosis, based on clinical presentation, most often was intra-abdominal inflammatory disease. The chief complaints in our series were fever (100%) and right upper abdominal pain (66.7%). Hepatomegaly and jaundice were noticed in 57.1% and 19% respectively. Schwartz et al11 however have reported that fever accompanied by chills and sweating is present in over 75% of the patients. Hepatomegaly is observed in 30-60% of cases and jaundice is an uncommon finding. While the predominant symptoms and signs recorded by Rubin et al8 are fever (87%), hepatomegaly(51%) and right upper quadrant pain (47%). Clinically, apparent jaundice was noticed only in patients with abscess secondary to biliary tract infection or with adjacent sites of localized. suppuration. 4,8 The diagnosis was then confirmed by ultrasound test, laparotomy and aspiration of abscess content. However, pyogenic hepatic abscess has, in many instances, produced sterile cultures which probably reflects inadequate culture techniques for anaerobic microorganisms9. Pyogenic cultures were obtained from pyogenic abscesses in 82%8 and 50A%11 of cases. Further more, amoebic trophozoites are occasionally found in the pus of amoebic hepatic abscess9,11. Since Iraq is endemic for hydatidosis13 differential diagnosis must be done. Hydatid cyst should always be excluded due to the potential risk of spreading if material from the cyst leaks out into the peritoneal cavity12,14. In our series, Entarnoeba histolytica Escherichia coil and mixed bacteria were detected in 47.6%, 28.6% and 14.3% of the cases respectively. Sterile abscess was found in only 9.5% of the cases. The high amoebic abscesses observed in this study are related to the high prevalence of intestinal amoebiasis in the area15 . In contrast, amoebic abscesses are relatively uncommon in the unendemic countries5,8,1. The present study and others4,8,10,11 have found that E.coli is the prime bacterial invader of the liver. Staphylococcus aureus and streptococcal species being reported either of lesser importance4,10,1,5 or equally important8. Nevertheless, Proteus, Klebsiella-Enterobacter and Pseudomonas also play a major role4,8,1. Due to the high reported percentage (38-60%) of sterile hepatic abscesses in the past, the concern of anaerobic bacteria have been realized1,4,8. Thereafter, the percentage of sterile hegatic abscesses have dropped to a less than 15%4,7. Nineteen hepatic abscesses were located in the right lobe probably due to its relative bulk confirming the findings of others5,6,11,12. The observed 2 left lobe abscesses in this work were amoebic in nature. A solitary amoebic abscess of the left lobe is rare but has a particular propensity to cause perforation8. Due to a wide diversity of microorganisms that have been associated with hepatic abscess, definitive chemotherapy depends on the results of properly obtained cultures and antimicrobial sensitivity. In other words, the choice of chemotherapy be determined according to the source of the abscess. But, today, it is not clear that these microorganisms will remain sensitive to the chosen antibiotics. Metronidazole is effective against intestinal and hepatic amoebiasis, anaerobic and a number of gram-negative microorganisms likely to be encountered in hepatie abscess5,9 . Thus, metronidazole was given to all patients in our series in combination with either tetracycline, ampicillin or gentamicin because it has a potential advantage in its rapid and consistent bactericidal and amoebicidal activities. However, open surgical drainage still has a significant role in the treatment of hepatic abscess. Survival rate recorded in this study was 100%. Others reported a rate of 95%5, 93%11, 91%6, 81% and 70%4 in uncomplicated cases. But Rubin et al8 had documented that only 21% patients over 50 years of age and 47% patients under 50 years of age were survived. The present results reflect a better understanding of the epidemiology, diagnosis and treatment of hepatic abscess in Iraq. With availability of the ultrasound test and modern surgery, mortality was not recorded. Metronidazole shows great promise as an effective bactericidal and amoebicidal agent. Until assessing the efficiency of antibiotics treatment alone, open surgical drainage in combination with chemotherapy remains the treatment of choice.
REFERENCES
1. Altemieer, W.A., Schowengerdt, C.G. and Whiteley, D. H. Abscess of the liver, surgical considerations. Arch. Surg., 1970; 101:258.
2. Berger, L.A., Osborn, D.R. Treatment of pyogenic liver abscesses by percutaneous needle aspiration. Lancet, 1982; 1:132.
3. Braun, B., Pernice, H., Herzog, F., Bonier, N. and Dormeyer, H.H. Diagnosis and therapy of liver abscess by ultrasonographic imaging, puncture and drainage. Hepatogastroenterology, 1982; 30:9.
4. L.azarchick, J., DeSouza e Silva, N.A., Nichols, D.R and Washington, J.A. Pyogenic liver abscess. Mayo Gin. Proc., 1973; 48:349.
5. Hardy, J.D. Rhoads textbook of surgery, principles and practice. 5th ed. Philadelphia, Lippincott, 1977.
6. Gerzof, 5.0., Johnson, W.C., Robbins, A.H. and Nab-seth, D.C. Intrahepatic pyogenic abscesses; treatment by percutaneous drainage. Am. J. Surg., 1985; 149:487.
7. Sabbaj, J., Sutter, V.L and Finegold, S.M. Anaerobic pyogenic liver abscess. Ann. Intern. Med., 1972; 77:629.
8. Rubin, RH., Swartz, M.N. and Malt, It Hepatic abscess; changes in clinical, bacteriologic and therapeutic aspects. Am. 3. Med., 1974; 57:601.
9. Greaney, 0.C., Reynolds, T.B. and Donovan, AJ. Ruptured amoebic liver abscess. Arch. Surg., 1985; 120:555.
10. Ochsner, A., DeBakey, M. and Murray, S. Pyogenic abscessof the liver. II.An analysis of 47 cases with reviewof the literature. Am. 3. Surg., 1938; 40:292.
11. Schwartz, Si., Shires, G.T., Spencer, F.C. and Storer, E.H. Principles of surgery. 3rd ed. New York, McGraw Hill, 1979.
12. Beaver, P.C., Jung, B.C. and Cupp, E.W. Qinical parasitology. 9th ed. Philadelphia, Lea & Febiger, 1984.
13. Mahdi, N.K., Benyan, A.Z.and Al-Nowfal, A. Hepatic hydatidosis of man and his livestock in southern Iraq. Jpn. J. Trop. Med. Hyg., 1987; in press.
14. Schiller, C.F. Complications of echinococcus cyst rupture; a study of 30 cases. JAMA., 1966; 195:220.
15. Mahdi, N.K. and Jassim, A.H. Intestinal parasitic infec tions of primaiy school children in three regions of Southern Iraq. Med. J. Basrah Uni., 1987; 6:55.
16. Sherman, J.D. and Robbins, S.L. Changing trends in the casuistics of hepatic abscess. Am. J. Med., 1960; 28:943
17. Butler, TJ. and McCarthy, C.F. Pyogenic liver abscess. Gut, 1969; 10:389.
18. de la Maza, L.M., Naeim, F. and Berman, L.D. The changing etiology of liver abscess. JAMA., 1974; 227:161.
19. Hirschowitz, 8.1. Pyogenic liver abscess; a review with a case report of a solitary abscess caused by Salmonella enteriditis. Gastroenterology, 1952; 21:291.
20. Pyrtek, U., and j3artus, S.A. Hepatic pyemia. N. Engl. J. Med., 1965; 272:551.
21. Basile, J.A., Klein, S.R., Worthen, NJ., Wilson, S.E. and Iliatt, J.R. Amoebic liver abscess; the surgeon’s role in management. Am. J. Surg., 1983; 146:67.
22. Wafai, I., Mahajan, K.K. and Leven, H. Percutaneous drainage of pyogenic liver abscesses; an alternative to open drainage. J. Kuwait Med. Assoc., 1987; 21:97.
23. de Louvois, J. The bacteriology and chemotherapy of brain abscess. J. Antimicrob. Chemother., 1978; 4:395.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: