
Zaman Shaikh ( Department of Medicine, Medical Unit-3, Civil Hospital, Karachi. )
Masood Hameed Khan ( Department of Medicine, Medical Unit-3, Civil Hospital, Karachi. )
Rana Qamar ( Department of Medicine, Medical Unit-3, Civil Hospital, Karachi. )
October 1989, Volume 39, Issue 10
Original Article
Abstract
One hundred patients with liver abscess were studied for clinical features and complications. They were diagnosed by radiography, ultrasonography, serology and by needle aspiration. A variety of interesting clinical, haematological and ultrasonographic findings were observed. Literature on liver abscess was reviewed and results compared (JPMA 39: 256, 1989).
INTRODUCTION
Amoebiasis is very common in Pakistan. Due to recurrent amoebic intestinal infection, the prevalence of amoebic liver abscess is also very high. Clinical features and laboratory parameters of such cases varywidely and poses a great diagnostic problem. One hundred cases of liver abscess were studied in the department of Medicine, Dow Medical College and Civil Hospital, Karachi. Cases from four other hospitals of the city were also included in the study.
PATIENTS AND METHODS
One hundred patientswith liver abscess were studied for aetiology, clinical features, complications, laboratory parameters, radiological and ultrasound findings. Abscess was diagnosed on ultrasonographic examination, aspiration and serological tests for amoebiasis. Patients were interrogated in detail and examined thoroughly. They were subjected to sigmoidoscopy, stool was tested for Entamoeba Histolytica, X-ray chest was done for any pleuropulmonarycomplication. Aspiration ofthehepatic pus was done for routine examination, bacteriology and to see active trophozoites. These patients received antiamoebic treatment in the form of metronidazole (infusion/tablets) and chloroquine orally close aspiration of the hepatic abscess was performed in some cases. In cases of pyogenic liver abscess, anti-bacterial therapy was instituted. These patients were subjected to re-examination after 3 weeks for clinical and laboratory parameters.
RESULTS
Of 100 patients, % had amoebic and 4 pyogenic abscesse& In the later group Actino-mycosis and proteus was cultured from one case each and E.coli from two cases. Mean age inthe amoebic group was 40 years, while in the pyogenic group it was 46 years. Males out numbered females both in the amoebic (85%) and pyogenic groups (75%). Patient’s history and physical examination revealedthat fever (95.8%),right upper abdominal pain (91.6%) and anorexia (693%) were the commonest symptoms, while hepatic tenderness (100%) and hepatomegaly (100%) were the cardinal signs of amoebic liver abscess. Temperature ranged from 38.5c to 40oc It was remittent in 72% and intermittent in 28% of the cases. It was accompanied by chills in 46% cases and rigors in 14%. Mean temperature at the time of admission was 38.09°C ± 036°C. Hepatic tenderness was rated as mild, moderate and severe. Mean downward hepatic enlargement was 8 ±23 cms in the midclavicular line below the right costal margin. Upward enlargement, also confirmed on X-ray chest, PA view was present in 45.8% of cases with amoebic liver abscess. Splenomegalywas present in only 3.0% of cases, enlargemënt below the costal margin was 4 ± 13 cms (Table 1).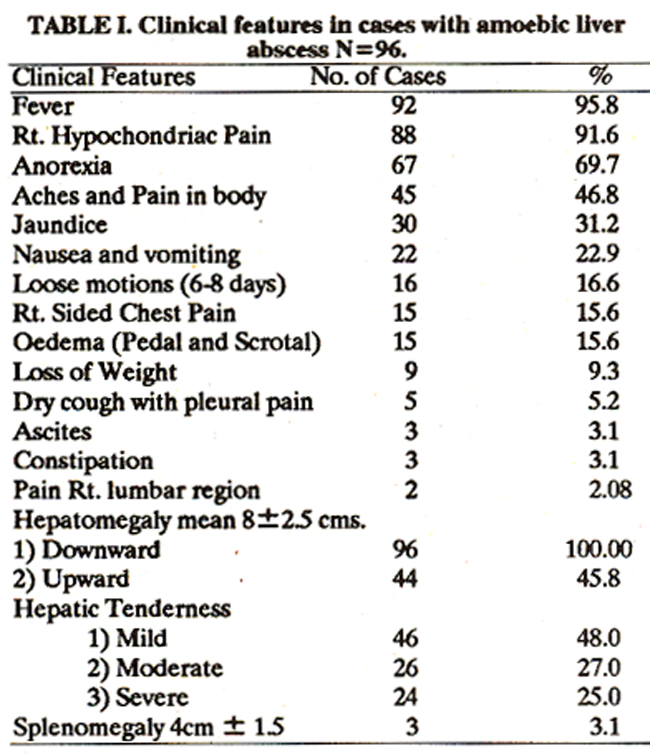
Stool when tested for cysts and trophozoites of Entamoeba Histolytica showed cysts in 80% of the cases and vegetative forms in 20%. Sigmoidoscopy could be done only in 26 cases (27%), as the rest were not willing for the procedure. Only four cases had amoebic ulcers. Thirty one patients with amoebic liver abscess had complications, like pleural effusion16 rupture into peritoneal4 and pleural cavities3, compresion of the inferior vena cava3 secondary infection, hepatic encephalopathy and monoparesis.1 Laboratory investigations in the amoebic group showed a raised serum bilirubin in 38% and a raised ALT in 60% of cases. More significant was the level of serum alkaline phosphatase which was elevated in 94% of the cases with a mean rise of two fold above the normal level. Leucocytosis was present in all the patients (mean TLC=19,807/ cumm). Mean ESR was 81mm in the 1st hour by Western method. Investigations were repeated at the end of 3 weeks (Table II).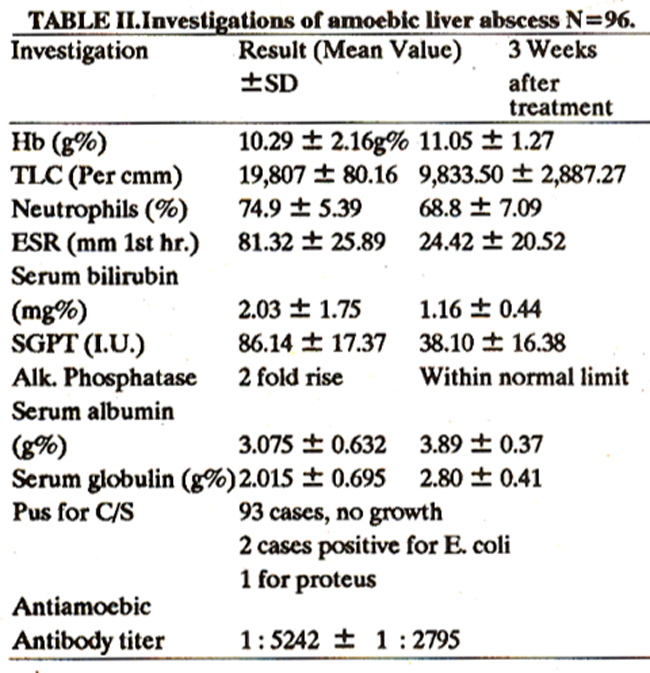
Radiology of the chest was normal in 33.3% cases with amoebic liver abscess. Two major radiological abnormalities noted were raised right hemidiaphragm (40%) and right sided pleural effusion (16%) while 11% had both abnormalities. Ultrasonographic findings showed that smallest abscess was 3 x 3.5cms and the largest 16.8 x 14.4 cms. Seventy Five percent abscesses were in the right lobe, 17% in the left and 8% in both lobes. Eighty five percent cases had a single abscess, 6% double and 8% had multiple abscess.
DISCUSSION
Present study comprises of 96 patients with amoebic liver abscess and 4 with pyogenic. This contrasts much with the studydone bykubinson et al1, who found 5 cases of amoebic and 12 cases of pyogenic liver abscess in a series of 17 cases.All patients with pyogenic liver abscess had multiple abscesses. There was no significant difference clinically and on routine laboratory investigations between this and the amoebic liver abscess group. In one case with pyogenic liver abscess, actinomycosis was diagnosed on culture. This patient was operated for appendisectomyabout 20 years back. However, such a long latent period is not acceptable. This patient was a heroin addict with impaired immunity, hence infection might have come from some unrecognized focus like dental abscess. Moreover, in the absence of a definite proof, this case remains in the category of cryptogenic liver abscess. This was the only mor talityin the present series. Comparison of the present studywith a study done on 137 patients with liver abscess3 showed that majority of the patients in the present study presentedwith classical syndrome i.e. fever, pain in the right hypochondrium, and tender hepatomegaly. Other striking differences were high percentage of anorexia, jaundice and loose motions in the present study being 69%, 31% and 16% respectivelyin comparison to 2.2%, 8% and 6.6% respectivelyin the other study (Table III).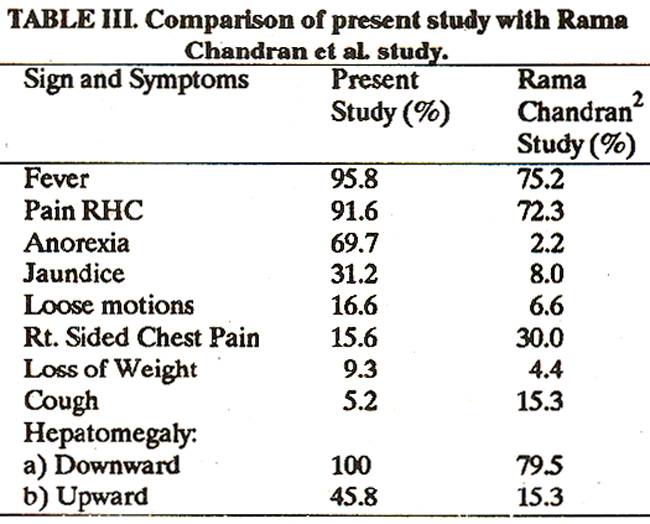
Two points in the present study are worth mentioning. One is the occurrence of Jaundice and other is concomitant presence of intestinal amoebiasis with liver abscess. According to Wilmot and Hennessy3, jaundice occurs in less than one percent of the cases and is usually obstructive in nature. Adams and Maergraith4 are of the opinion that jaundice never occurs jn amoebic liver abscess. Moreover Chalgidakis5 reported jaundice in 18% of his 87 fatal cases of amoebic liver abscess. The combination of amoebic colitis and liver abscess is said to have a grave prognosis, but all our patients with this presentation (16.6%) recovered without any complication. The above association has also been reported by others6-9. The scrotal and pedal oedema was present in 15.6% of the patients. Three patients had obstruction of the inferior vena cava, diagnosed clinically and on ultrasonographic examination. In these patients oedema subsided within 24 hours of drainage of the abscess. Serum albumin level was within normal limits in these three patients. Rest of the patients with oedema had hypoalbuminaemia (Serum Albumin less than 2.5 gm%). Monoparesis occurred in one patient with amoebic liver abscess. He was normotensive and non-diabetic. During stay in the hospital, he developed paresis of the left upper limb. C.T. scan of the brain could not be performeçl as the patient left against medical advice. Emboli to brain and lungs alongwith D.I.C. has been described10 in pyogenic but not in amoebic liver abscess. One patient presented with hepatic encephalopathy, this is in contrast to most reported series where none of the patients had encephalopathy, 2,11,12. One case each of encephalopathy was reported in 196616 and 196714. Intra-peritoneal rupture is a very serious complication of amoebic liver abscess. Singha15. reported sudden pain at the site of rupture and Vakil et al,16 acute symptoms without actual rupture. In the present series, four patients had intraperitoneal rupture of the abscess but none had any history of sudden abdominal pain. Reported frequency of this complication varies from 2.5%17 to 17%18. In an Indian study12 of 779 patients with liver abscess 2.4% ruptured into peritoneal cavity. This complication has also been reported by others. 14,19 Thoracic complications of liver abscess20,21 include rupture and drainage through bronchi, rupture into right or left pleura with empyema, rupture into the pericardium and right sided pleural effusion. In the present study, reactionary pleural effusion was seen in 16%, perforation into the right pleural space in 3% and raised right dome of the diaphragm in 39.7% of cases. In 15%, there was combined abnormality. Some other interesting complications which have not been encountered in the present study are rupture through the skin, 22 hepatocolic fistula14 and haematobilia23 and various other studies described the clinical features and complications of amoebic liver abscess,9,10,20,29-30 All of them have emphasized that amoebic liver abscess can be confused not only with pyogenic liver abscess, but it may mimic abdominal malignancy and hepatic granuloma. It may also be confused with viral or alcoholic hepatitis, cholecystitis, pyogenic cholangitis, hepatic hydatid cyst, perforated peptic ulcer, acute appendicitis, subdiapbragmatic abscess and lesions of the right lung base and right pleura. Thus recognition of well-defined but diverse clinical syndromes are important not only for diagnosis but for planning surgical treatment.
REFERENCES
1. Rubinson, HA, Isikoff, M.B. and Hill, M.C. Diagnostic imaging of hepatic abscess; a retrospective analysis. A.TR., 1980; 135:735.
2. Ramachandran, S., Goonatillake, H.D. and Induruwa, PAC. Syndromes in amoebic liver abscess. Br. J. Surg., 1976; 63:220.
3. Wilmot, AJ. Clinical nmoebiasis. Philadelphia, Davis, 1962, p.102.
4. Adams, A.R.D. and Maergraith, B.G. Amoebiasis, in clinical tropical diseases. 3rd ed. Oxford, Blackwell, 1964,p.3.
5. Chalgidakis, C.B. The pathology of hepatic amoebiasis as seen on the Wit Waler brand. South Afr. J. Clin. Sc., 1953; 4:230.
6. Cain, G.D., Moore, P. and Patterson, M. A ten years review of amoebic abscess of the liver 1956-66. Am. 1. Dig. Dis., 1968; 13:709.
7. Turner, J.A., Lewis, W.P., Hayes, M. and Ziment, I. Amoebiasis, a symposium. Calif. Med., 1971; 114:44.
8. Shabot, J.M. and Patterson, M. Amoebic liver abscess 1966-76. Am. J. Dig. Dis., 1978; 23:110.
9. Verlenden, W.L. and Prey, C.F. Management of liver abscess. Am. J. Surg., 1980; 140:53.
10. Sanford, N.L, Bradbear, RA. and Powel, LW. Pyogenic liver abscess a qeglected diagnosis. Aust. N.Z. J. Med., 1984; 14:597.
11. Farid, Z., Trabolsi, B., Kilpatrick, M.E., Yassin, W.M. and Watten, RH. Amoebic liver abscess presenting as fever of unknown origin (FUO). Serology, isotope scan fling and metronidazole therapy in diagnosis and treatment. J. Trop. Med. ilyg., 1982; 85:255.
12. Eggieston, P.C., Handa,A.K.andVerghese,M.Amoebic peritonitis secondary to amoebic liver abscess. Surgery,1982; 91:46.
13. Wright, It Amoebiasis, a diagnostic problem in Great Britain. Br. Med. J., 1966; 1:957.
14. Rab, S.M., Alam, N., Hoda; A.N. and Yes, A. Amoebic liver abscess; some unique presentation. Am. J. Med., 1967; 43:811.
15. Singha, H.S.K. Spontaneous intra-peritoneal rupture of solitaiy(amoebic)liverabscess. Br. J.Surg., 1959; 47:198.
16. Vakil, B.J., Metha, AJ. and Desai, H.N. A typical manifestation of amoebicabscess of livers. J. Trop. Med. Hyg., 1970; 73:63.
17. Adi, P.C. Complications, treatment and prognosis of hepatic amoebiasis. West Mr. Med. J., 1966; 15:43.
18. Nadkarni, S.V., Parashar, S.K., Malik, T.K. and Varmi, LA. Amoebic abscess of the liver. Tnt. Surg., 1973; 58:112.
19. Lamont, N. M. and Pooler, N.R. Hepatic arnoebiasis. A study of 250 cases. QJ. Med., 1958; 27:389.
20. Young, A.E. The clinical presentation of pyogenic liver abscess. Br. J. Surg., 1976; 65:216.
21. Rhode, P.C., Prieto, 0. and Riveros, 0. Thoracic corn plications of amoebic liver abscess. Br. J. Dis. Chest, 1979; 75:302.
22. Heimburger, LP. Amoebiasis cutis with a survey of medical literature to date. Arch. Dermatol. Syph., 1925;11:49.
23. Larsen, L.R. and Raffensperger, J. Liver abscess. J. Pediatr. Surg., 1979; 14:329.
24. McFadzean, AJ.S., Chang, ICP.S. and Wong, C.C. So litaiy pyogenic abscess of the liver treated by closed aspiration and antibiotics. A report of 14 consecutive cases with recovery. Br. J. Surg., 1953; 41:141.
25. Perera, M.R., Kirk, A. and Noone, P. Presentation, diagnosis and management of liver abscess. Lancet, 1980;2:629.
26. Price, M.E. Amoebic liver abscess in a Norfolk factory worker. Br. Med. J. (Clin Rca.), 1981; 283:1175.
27. Abuabara, S.F., Barrett, J.A., Hau, T. and Jonasson, 0. Amoebic liver abscess. Arch. Surg., 1982; 117:239.
28. Northover,J.M.A., Jones, BJ.M., Dawson, J.L and Williams, It Difficulties in diagnosis and management of pyogenic liver abscess. Br. J. Surg., 1982; 69:48.
29. Fischer, M.G. and Beaton, H.L Unsuspected hepatic abscess associated with biliaiy tract diseases. Am. J.Surg., 1983; 146:658.
30. Dietrick, R.B. Experience with liver abscess. Am. J. Surg., 1984; 147:288.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: