
H.R. Chaudhry ( Department of Psychiatry, Fatima Jinnah Medical College and Sir Ganga Ram Hospital, Lahore. )
Z. Qureshi ( Liaquat National Hospital, Karachi. )
I.A.K. Tareen ( Department of Psychiatry, Mayo Hospital, Lahore. )
I. Yazdani ( Department of Psychiatry, GlaxoSmithKline Pakistan, Karachi. )
November 2002, Volume 52, Issue 11
Original Article
Abstract
Objective: To assess the efficacy and tolerability of paroxetine 20mg daily, for the treatment of depression and depression associated with anxiety.
Method: An open, non-comparative study undertaken at three centers in three cities of Pakistan. A total of 112 in-or out- patients, presenting with a major depressive episode were included in the study. Depression was diagnosed according to DSM IV criteria and a Hamilton Rating Scale for Depression (HAMD -D) score of >18 on the first 17 items of the HAM-D-21. After a placebo washout period of 7 days, patients were given a 20-mg fixed dose of paroxetine daily in the morning for a period of 6 weeks. After baseline, regular assessments were made at 1, 2, 4 and 6 weeks. Efficacy measures included the HAMD-D, the Clinical Anxiety Scale, The Clinical Global Impression Severity of Illness Scale (CGI-S), and the Clinical Global Impression Improvement Scale (CGI-I). Tolerability was assessed by any adverse event. The primary therapeutic outcome measures were patients who achieved a 50% or greater reduction in HAMD-D score at the end of the treatment or achieved a reduction in final HAMD-D score of <1 0 points. The final scores of 1 or 2 for CGI-S and CGI-I were considered as full clinical response.
Results: Of 112 cases evaluated, 57 were males and 55 females whose ages ranged from 18 to 65 years. There was a clear and statistically significant efficacy of paroxetine on all the major outcome variables. A total of 88% patients achieved a reduction in the final HAMD-D score at the end of treatment. The total HAM-D score reduced to 10 or less in 73% patients at 6 weeks and by this week 76% and 92% patients achieved a score of I or 2 for CGI-S and CGI-l, respectively. The mean Clinical Anxiety Scale score reduced from 12.6 at the baseline to 4.4 at the end of treatment. Safety data was evaluated in all 112 patients and paroxetine was well tolerated. Adverse events were experienced by 10% of patients of whom 4% were dropped from the study. Nausea was the commonest adverse event reported.
Conclusion: The study shows that paroxetine is an effective, well-tolerated, and safe drug for the treatment of depression (JPMA 52:518;2002).
Introduction
Major depression is a prevalent psychiatric condition1,2 which according to current clinical guidelines strongly needs drug treatment3-5. Unfortunately, the pharmacologic management of depression is not always that easy, because the traditional antidepressant drugs are far from ideal. Most of these drugs, for example, tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs) are associated with a variety of unpleasant side effects that can reduce compliance6 and increase the risk of extremely dangerous toxicity in case of overdosage6,7.
Recent studies indicate that over the last decade, selective serotonin re uptake inhibitors (SSRIs) have entered wide-spread clinical use and are increasingly becoming the agents of choice in the treatment of major depression, replacing TCAs8-11.
Paroxetine is a novel phenylpiperidine antidepressant agent. It acts as a potent and selective inhibitor of serotonin re-uptake in the brain, thus enhancing serotonergic neurotransmission. It is structurally different from the cyclic antidepressant drugs and the other SSRIs. It has been shown in vitro to be more potent and selective than fluoxetine, sertraline and fluvaxamine12,13 suggesting a potentially improved safety and tolerability profile. Paroxetine has a mean terminal elimination half-life of about 24 hours, permitting once daily administration and has no active metabolites, unlike fluoxetine and sertraline. Dosage adjustment is accomplished more quickly with paroxetine as compared to other SSRIs. In double blind, controlled studies the efficacy of paroxetine was found to be comparable to that of imipramine, clomipramine, amitriptyline, and mianserine14-18.
This open, non-comparative, multicenter trial was conducted at three centers to assess the efficacy and tolerability of Paroxetine 20mg daily in the treatment of patients suffering from major depression and depression with associated anxiety.
Patients and Methods
Patients
Patients suffering from depression with or without anxiety who fulfilled DSM IV criteria for a current episode of major depression and who had a score of 18 or more on the first 17 items of the 21- item Hamilton Rating Scale for Depression (HAM - D) were selected for the study. All patients gave written consent for participation in the study.
Patients were excluded from the study if they had any clinically significant co-existing disease like renal, hepatic, cardiovascular, neurological or gastrointestinal disorders. Other exclusion criteria included patients at a significant suicidal risk; those with a recent history or concomitant diagnosis of substance addiction; and patients with marked hallucinations, delusion, schizophrenia, organic brain syndrome, or a history of hypersensitivity or intolerance to SSRIs. In addition patients were excluded if they had received treatment with any other investigational new drug within the previous 4 weeks, had received electroconvulsive therapy or other antidepressant drugs in the last 4 weeks, or were presently receiving psycho-stimulants. Female patients were excluded if they were pregnant, lactating or planning a pregnancy during the study, or not using a medically acceptable form of contraception.
This was an open, non-comparative, 6 week study performed in three hospitals in three different cities of Pakistan, using the same protocol. The trial was conducted in accordance with good clinical practices and the Helsinki Declaration.
Visits were scheduled as visit 1 for screening, visit 2 as baseline (Day 0), and then at 1, 2, 4 and 6 week. Physical screening of eligible patients at visit 1 included body weight, physical examination and evaluation of vital signs. The patients’ baseline demographic data, medical history, psychiatric history and record of concomitant medication were collected and inclusion and exclusion criteria were checked. Psychiatric screening included use of the 21 - item HAM - D, the 6 - item Clinical Anxiety Scale and a seven point rating scale of Clinical Global Impression - Severity of Illness (CGI - S).
All patients selected for the study completed a one-week placebo washout period and were scheduled for baseline visit. After compilation of baseline safety and efficacy ass essment data, patients received a medication pack of par )xetine 20mg tablets, to be taken once daily as a fixed dose in the morning with food.
The protocol prohibited the use of any other antidepressant medication during the study. Short acting benzodiazepines were permitted for sleep disturbance, if required. Patients taking non-psychotropic medication were allowed to continue their use if the patient had been stabilized on the medication for 4 weeks.
Following baseline visit, the patients were evaluated at the end of weeks 1, 2, 4 and 6.
During each visit the HAM-D, Clinical Anxiety scale, CGI-S and CGI-I were completed. Tolerability was assessed by asking a non-leading question with the spontaneous responses being recorded, as were all clinical adverse events. For each adverse event, physicians recorded the nature of the event, time of onset, duration, severity and relationship to treatment, Compliance of the patient with treatment was assessed by means of capsule count returned at each clinic visit. At the end of 6 weeks, or upon termination of the study, patients underwent physical examinations and evaluation of vital signs. A conclusion record assessed patients’ reasons for completion/termination of the study.
The primary therapeutic outcome variable was HAM-D total score. Responders were defined as those who achieved reduction in fmal HAM-D total score of less than or equal to 10 or those who achieved a greater than or equal to 50% reduction in HAM-D score at the end of the treatment compared to base line. The other efficacy variable that were also considered included change from base line in the Clinical Anxiety Scale total score, CGI-S scores of 1 (normal, not at all ill) or 2 (border line mentally ill) and CGI-I score of 1 (very much improved) or 2 (much improved).
Safety analysis, demographic and clinical characteristic summaries comprised the data from all patients who were enrolled in the study and received at least one dose of medication. Efficacy analysis excluded the patients who received less than 2 weeks treatment or failed to return for an end of study evaluation. Patients who deviated from protocol (including non-compliance) or consumed prohibited medication were also excluded.
The statistical analysis included students’ t-test or a one- way analysis of variance (ANOVA): Power analysis was performed using a = 0.05 and a = 0.01. Statistical analyses were made with SPSS version 10.0 for Windows.
Results
A total of 112 patients were enrolled for the study.
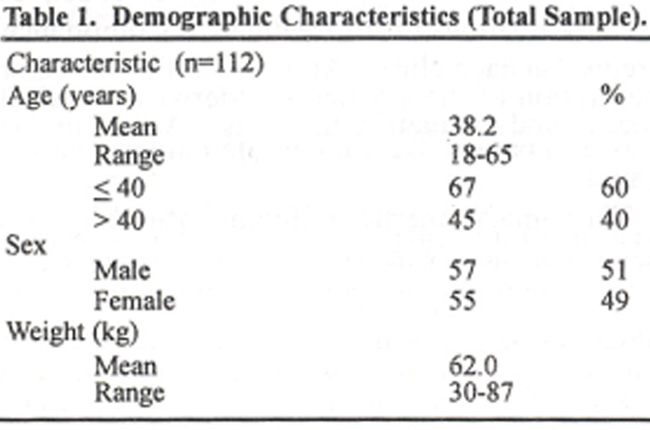
Table 1 shows demographic characteristics of the patients. The mean age of the patients was 38 years (range 18-65 years). Forty nine percent of the patients were women. Clinical characteristics are given in Table 2.
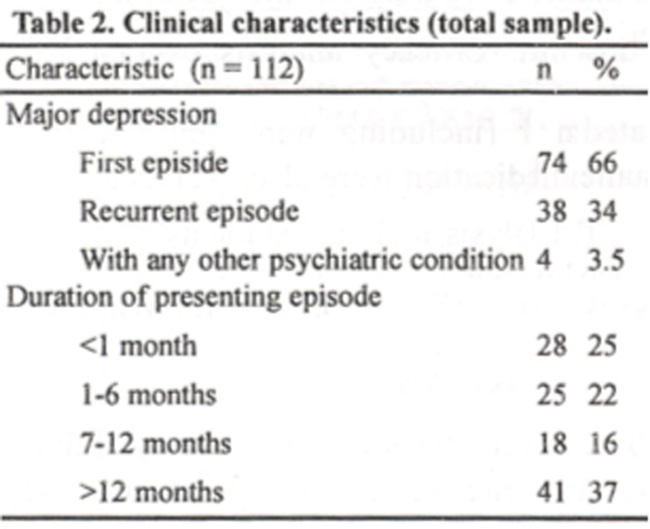
Depression was diagnosed as first episode in 66% of the patients. The depressive episode had been present for less than one month in 25% patients, between 1 and 6 months in 22% and for more than 6 months in 53% patients. Of the patients who had been previously diagnosed with depression, 25% had used antidepressants. Forty-one percent of the patients had at least one concomitant illness and 45% were taking concomitant medication during the study, whereas 55% did not use any concomitant medication. The most commonly used medications were gastrointestinal drugs, antihypertensives, non-steroidal anti-inflammatory drugs, antiemetics and anti-diabetics. Benzodiazepines were also taken in few cases.
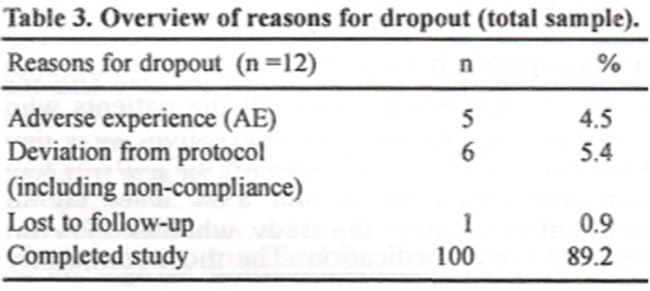
A total of 100 out of 112 patients (89.2%) completed the 6-week study. The reasons for dropout are given in Table 3.
The efficacy of paroxetine on the primary outcome variable HAM-D is shown in Figure 1.
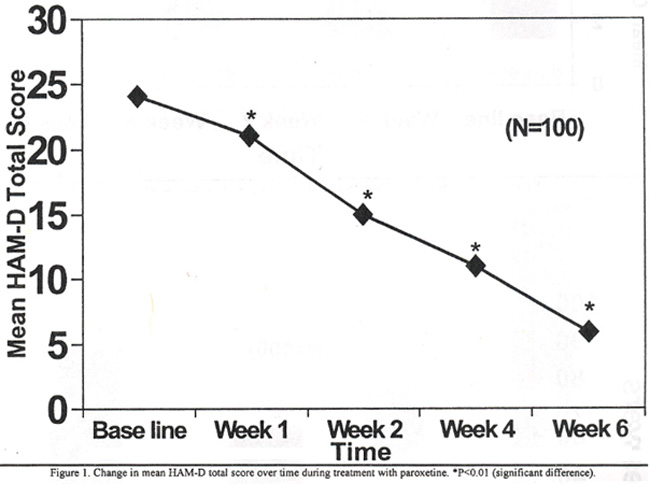
The mean HAM-D score at baseline was 24, which showed a highly significant difference at weeks 1, 2, 4 and 6 (P<0.01). By week 6, the mean HAM-D score decreased to 6.2, from a baseline of -18.2 (highly significant). As symptoms of depression improved, so did symptoms of anxiety. When the Clinical Anxiety Scale was considered, there was a significant reduction in the mean baseline, score of 12.6, over the 6 weeks (Figure 2),
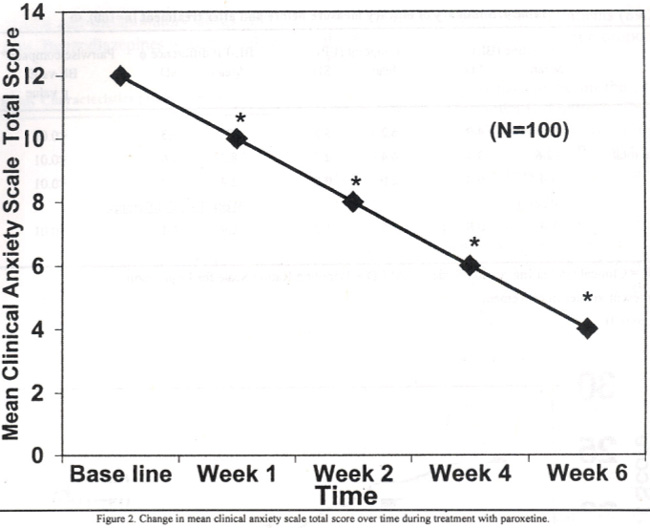
the mean end of treatment score being 4.4 with a difference of 8.2 (p<0.01). At week 4 the percentage of responders defined by a reduction >50% from baseline HAM-D, total score was 62% compared to 20% responders at week 2 (p<0.01) (Figure 3).
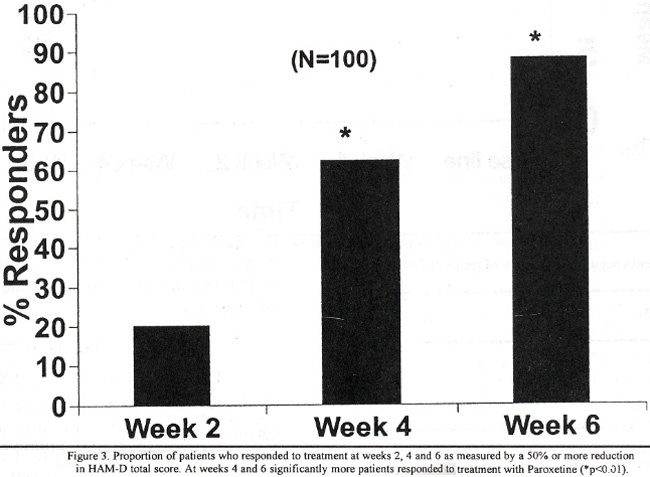
This early significant response continued till week 6, when percentage of responders increased to 88%. Considering the number of patients whose total HAM-D score was reduced to 10 or less at each assessment, a high proportion of patients achieved a response using this criterion at week 6 (Figure 4).
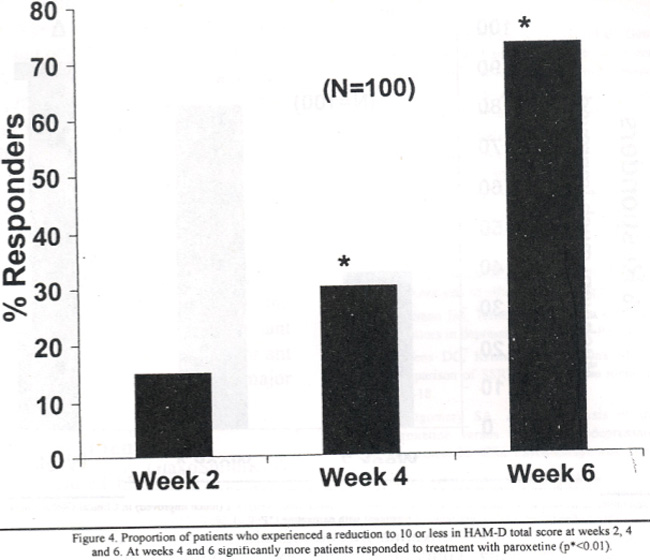
The response at week 6 was 73% compared to 30% at week 4 (p<0.01). A positive response on CGI - severity of illness was defined as a score of 2 or less, for those who had been assessed with a score of 4 or more at baseline. All patients in this study had a mean CGI-S score of 4.4 at baseline. After 6 weeks of treatment with paroxetine 76% patients had scores of 1 or 2 compared to 37% at week 4 (p<0.01) (Figure 5).
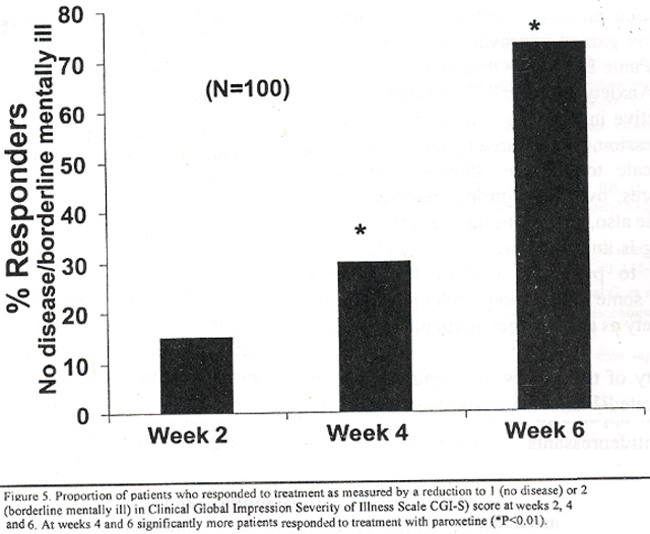
Of the responders on CGI-S, 28% of patients had a score of 1 (no disease) and the remaining 72% had a score of 2 (borderline mentally ill). By week 6 the mean CGI-S score reduced to 2.0 (p<0.01). Results obtained for Clinical Global Improvement, showing the percentage of patients who responded to treatment as measured by a reduction to I (very much improved) or 2 (much improved) are shown in Figure 6.
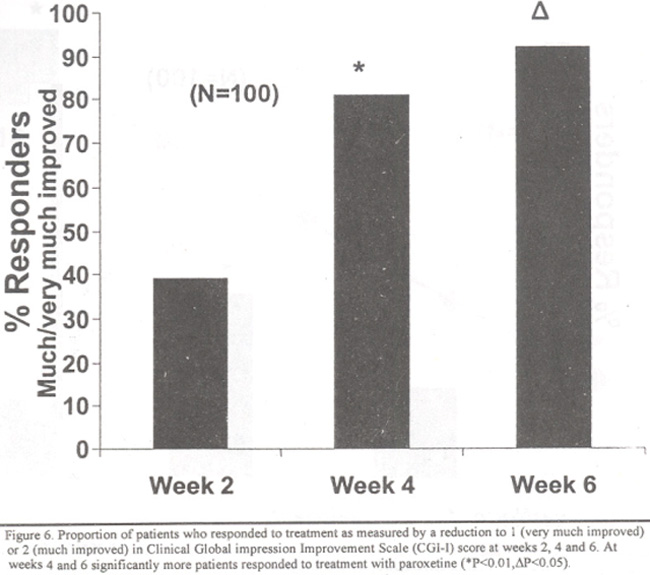
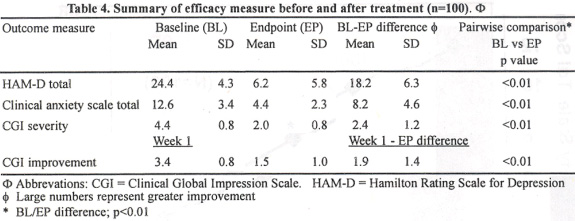
Paroxetine produced significant improvements at weeks 2, 4 and 6. The clinical improvement was most marked at week 4 (p<0.0l) showing 81% of patient responding to treatment compared to 39% response at week 2. At the end of the week 6, the response rate reached to 92% (p<0.05). Among these 92% responders, 66% patients had a CGI-l score of 1 (very much improved). The mean CGI-I score at week I was 3.4, which reduced to 1.5 at week 6 (p<0.0l). The results of all efficacy measures before and after treatment with paroxetine are summarized in Table 4.
Paroxetine was well tolerated. Adverse events were experienced by 10% patients but were mild and transient and occured early during treatment. The most common adverse event was nausea reported by 6% patients followed by anxiety and headache in 2% of patients (Table 5).
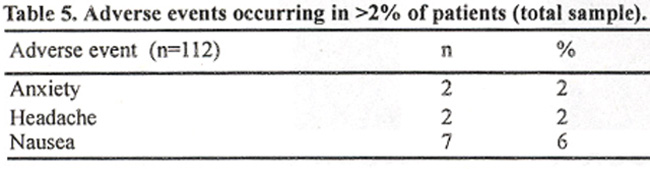
A total of five patients (4%) withdrew from the study because of adverse events.
Discussion
The results of this study show a significant antidepressive effect for paroxetine in patients from major depressive episodes. It exhibited significant efficacy on all outcome variables like HAM-D, Clinical Anxiety Scale, CGI severity of illness and CGI improvement. After 6 weeks of treatment, majority of patients responded to treatment. Considering the primary outcomc variable HAM. D. the baseline score of 24 decreased Paroxetine to 6, which is well below the threshold of 1 Paroxetine showed similar efficacy with regard to the achicvemcnt of HAM-D total scores of less than or eaual to 10, GI-S scores of 1 (no disease) or 4 (borderline mentally ill), and CGI-I scores ot 1(very much improved) or 2 (much improved). An ear’y onset of efficacy with paroxetine was evident from week 2 onwords on almost all efficacy variables and the consistent improvement was maintained till the end of the study Period Similar early response with paroxetine has also been observed in two large Placebo controlled studies19,20.
An important goal of antidepressant therapy is efficacy against concomitant anxiety symptoms. The findings has paroxetine has significantly greater efficacy in reducing concomitant anxiety symptoms than TCAs (excluding clomipramine) is sup ported by a comparison of pooled data analysis from paroxetine database21. In addition to improving associated anxiety symptoms, paroxetine is also effective and has gained approval for other anxiety disorders, including Panic Disorder, Obsessive-Compulsive Disorder and Social Anxiety Disorder22-24. In this study also paroxetine was effective in relieving symptoms of anxiety associated with depression, as measured by change in mean Clinical Anxiety Scale total score, showing consistent decline in mean scores, over time during treatment. For Clinical Anxiety Scale also, paroxetine had an early onset of efficacy. This finding is important because some clinicians might be reluctant to prescribe a SSRI for anxious depression, because some medications belonging to this class may cause anxiety as a side effect, particularly in early phase of treatment.
In the majority of the studies, paroxetine has been extremely well tolerated25 and the favorable tolerability profile of this agent appears to be its primary advantage over traditional antidepressants. Paroxetine lacks the anticholinergic, antihistamin i c, and cardiovascular side effects of the TCAs. Nausea has been the most frequently reported adverse event during short-term use of paroxetine, but it is generally mild and transient. Furthermore, the frequency of withdrawal due to adverse effects is less with paroxetine than with TCAs26.
In the present study also, paroxetine was very well tolerated and was not associated with typical anticholinergic side effects, such as dry mouth and constipation. Headache, commonly associated with other SSRIs, was reported by 2 improved) or 2 (much improved) in Clinical Global impression Improvement Scale (CGI-l) score at responded to treatment with paroxetine (*P<0.014 P<0.05). patients. Paroxetine was commonly associated with nausea (6%), which is similar to that with other SSRIs,. However, the nausea was generally mild. Only two patients dropped from the study due to nausea, Overall, adverse events were reported by 10% of study population, but the intensity of all were mild to moderate. No patient experienced any serious adverse event.
Considering safety data, paroxetine had no effect on blood pressure or on other vital signs. Body weight of the patients also remained unchanged. Unlike other SSRIs, paroxetine caused no weight loss, nor did it cause weight gain, as is often seen with TCAs. In addition, paroxetine had no sedating effects.
Results of this study further define the dosing regimen for paroxetine in the treatment of depression. The recommended starting dose of paroxetine is 20 mg/day for most patients, which is also shown to be the minimum effective dose27. The highly potent antidepressant activity and good tolerability observed in this study with fixed doses of 20 mg of paroxetine per day suggest that upward dose titration may be unnecessary for many patients. Such simplicity of dosing regimen should benefit patients as well as clinicians, especially as compared with TCAs and even other SSRIs, which may require frequent dose titration. The high degree of compliance observed with the present study may be attributed to the simple 20 mg dosing schedule. Only 4 patients dropped out from the study due to noncompliance, and of the patients, who completed the trial, only 7% patients missed any of the doses during the treatment phase.
Although the newer compounds may appear more expensive than older antidepressants, however, it is more important to take into account other benefits as well, such as acceptability, tolerability, improved compliance, reduced toxicity in overdosage, efficacy in the prevention of relapse and recurrence of illness and improved quality of life all must be considered when comparing the relative costs of medication.
Conclusion
The results of the present study in conjunction with those already published strongly suggests that paroxetine is an effective, well-tolerated, and safe medication for the treatment of depression, accompanied with concomitant anxiety symptoms. Paroxetine represents an important addition to the clinical tools available to treat major depression with associated anxiety.
Acknowledgement
This research was sponsored by GlaxoSmithKline Pakistan.
References
1.Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12 months prevalence of DSM-llI-R psychiatric disorders in United 5tates. Results from the National comorbidity Survey. Arch. Gen. Psychiatr., 1994; 5: 8-19.
2.Ormel J, VonKorff M, UstUn TB, et al. Common mental disorders and disability across cultures. Results from the WHO collaborative study onp psychological problems in general health care. JAMA., 1994; 272 1741.48.
3.Paykel ES, Priest RG. Recognition and management of depression in general practice: consensus statement. BMJ., 1992; 305: 1198-1202.
4.Agency for Health Care Policy and Research, Depression in Primary Care. Clinical Practice Guideline, Number 5, publication no. 93-0550. Rockville, MD: US Department of Health 5ervice, Agency for Health Care Policy and Research. AHCPR, 1993.
5.Ustun TB, Goldberg D, CooperJ, Simon GE, et al. New classification for mental disorders with management guidelines for use in primary care: LCD-I 0 PHC. Br. J. Gen. Pract., 45: 211-15.
6.Cookson J. Side effects of antidepressants. Br. J. Psychiatry, 1993; 163: 20-24.
7.Henry JA, Alexander CA, Sener EK. Relative mortality from overdose of antidepressants. BMJ., 1995; 310: 221-24.
8.Donoghue J, Tylee A. The treatment of depression: prescribing patterns of antidepressants in primary care in the UK. Br. J. Psychiatry, 1996;168:164-68.
9.Donoghue J, Tylee A, Wildgust H. Cross-sectional database analysis of antidepressant prescribing in general practice in the United Kingdom, 1993-5. BMJ., 1996; 3 13:861-62.
10.Martin RM. Hilton SR, Kerry SM, et at. General practitioners perceptions of the tolerability of antidepressant drugs: a comparison of selective serotonin reuptake inhibitors and tricyclic antidepressants. BMJ., 1997; 314:646-51.
11.Chaudhry HR, Kanwal Q, Altaf Q, et al. Effect of Paroxetine in postpartum depression. P. J. Neurol. ,2001;7: 54-56.
12.Thomas DR, Nelson DR, Johnson AM. Biochemical effects of the antidepressant paroxetine, a specific 5-hydroxytryptamine uptake inhibitor. Psychopharmacology, 1986; 93:193-200.
13.Johnson A. The comparative pharmacological properties of selective serotonin reuptake inhibitors in animals. In: Feighner if, Boyer WF, eds. Selective serotonin reuptake inhibitors. New York: John Wiley and 5ons Inc; 1991, pp. 37-70.
14.Song F, Freemantle N, Sheldon TA. Selective serotonin reuptake inhibitors: meta-analysis of efficacy and acceptability. BMJ., 1993; 306 683-87.
15.Anderson IM, Tomenson BM. The efficacy of selective serotonin reuptake inhibitors in depression: a sants. J. Psychopharmacol., 1994; 8:238-49.
16.Steffens DC, Krishnan KR, Helms MJ. Are SSRIs better than TCAs? Comparison of SSRIs and TCAs: a meta-analysis. Depress. Anxiety, 1997; 6:10-18.
17.Montgomery SA. A meta-analysis of the efficacy and tolerability of paroxetine versus tricyclic antidepressants in the treatment of major depression. Int. Clin, Psychopharmacol, 2001;16 169-78.
18.Chaudhry HR, Hofman PA., Awan MR. SelectivesSerotonin uptakeimnhibitors- an update: Pak. J. Neurol., 1996;2:93-98.
19.Claghom JL, Kiev A, Rickets K, et at. Paroxetine versus placebo: a double- blind comparison in depressed patients. J. Clin. Psychiatr., 1992;53: 434-38.
20.Dunbar GC, Cohn JB, Fabre LF, et al. A comparison of paroxetine, imipramine and placebo in depressed outpatients, Br. J. Psychiatry,. 1991; 53:394-98.
21.Dunbar GC, Fuell DL. The anti-anxiety and intiagitation effects of paroxetine in depressed patients. Int. Clin. Psychopharmacol, 1992; 6: 53-58.
22.Lecrubier Y, Judge R. Long-term evaluation of paroxetine, clomipramine and placebo in panic disorder. Collaborative Paroxetine Panic Study Investigators. Acta. Psychiatr. Scand., 1997; 95: 153-60.
23.Zohar J, Judge R. Paroxetine versus clomipramine in the treatment of obsessive-compulsive disorder. Paroxetine Study Investigators. Br. J. Psychiatry, 169:468-74.
24.Stein MB, Liebowitz MR, Lydiard RB, et at. Paroxetine tereatment of generalized social phobia (social anxiety disorder): a randomized controlled trial., JAMA. 1998; 28: 708-13.
25.Dunbar GC. An interim overview of the safety and tolerability of paroxetine. Acta, Psychiatr. Scand. Suppl., 1989; 80: 135-37.
26.Montgomery SA, Henry JA, McDonal G, et al. Selective serotonin reuptake inhibitors: meta-analysis of discontinuation rates. In.t Clin. Psychopharmacol., 1994; 9: 47-53.
27.Dunner DL, Dunbar GC. Optimal dose regimen for paroxetine. J. Clin. Psychiatry, 1992; 53: 21-26.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: