
I. Ahsan ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
M.U. Jehangir ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
T. Mahmood ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
N. Ahmed ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
M. Saleem ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
M. Shahid ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
A. Shaheer ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
A. Anwer ( Department of Medicine, Jinnah Postgraduate Medical Centre, Karachi. )
November 2002, Volume 52, Issue 11
Original Article
Abstract
Objectives: To study the differences between the clinical presentation and complications of amoebic and pyogenic liver abscess. To correlate the diagnostic significance of Entamoeba Indirect Haemagglutination test (E.IHA) in establishing the diagnosis of amoebic liver abscess.
Design: Open cohort observational study.
Setting: Department of Medicine (Medical Unit II) Jinnah Postgraduate Medical Centre, Karachi.
Participants: Fifty two patients aged 13-70 years admitted in Medical Unit II and diagnosed to have liver abscess.
Interventions: Group A comprised of patients clinically diagnosed to have amoebic liver abscess and received Metronidazole 500mg iv x 8 hourly for atleast 10 days or more if patient developed complications. Group B comprised of patients diagnosed to have pyogenic abscess and received Cefotaxime Ig iv x 8 hourly for the same duration or more if complicated (antibiotic reviewed in accordance with culture and sensitivity report).
Main Outcome Measures: Differences in the clinical presentation, complications and diagnostic parameters between the two groups of patients.
Results: It was not possible to differentiate between amoebic and pyogenic liver abscess on clinical grounds, routine investigations and imaging techniques. Aspiration of pus, especially if the abscess was multiple, was most helpful in differentiating the two types of abscesses. Serological test of E.IHA was highly specific and sensitive for amoebic liver abscess.
Conclusion: Majority of liver abscesses in Karachi are due to Entamoeba Histolytica. Pyogenic abscess though less frequent, must be excluded by pus aspiration and culture and sensitivity. E.IHA is a good rapid method of discriminating between the two types of abscesses (JPMA 52:497;2002).
Introduction
Liver is an organ prone to developing abscesses. It is a serious ailment fraught with a multitude of serious complications. Whereas amoebic liver abscess is the commonest abscess in the under developed tropical world, pyogenic abscess is more commonly encountered in the developed countries1,2. The high incidence of amoebic liver abscess can be attributed to malnutrition, poor personal hygiene, inadequate sanitary conditions and over crowding3. In the case of pyogenic abscess, micro-organisms may invade the liver via the portal circulation, systemic circulation, contiguous organs and biliary stasis due to bile duct obstruction. In 50% cases of pyogenic abscess no obvious predisposing focus of infection can be identified.
The overlap of symptoms between amoebic and pyogenic liver abscess makes early clinical differentiation difficult and hence jeopardizes correct management2. This small study was undertaken to try and delineate the clinical and laboratory differences between these two conditions.
Methodology
Study Design
This was an open cohort observational study conducted in Medical Unit II of Jinnah Postgraduate Medical Centre (JPMC), Karachi over a period of one year. This unit has 50 beds and admits medical cases on every third day. All patients of both sexes admitted with a clinical suspicion of liver abscess (subsequently confirmed by ultrasonogrpahy) were included in the study. A total of 52 liver abscess patients were admitted during the study period.
Study Protocol
Diagnosis of liver abscess was confirmed by ultrasonography. All patients also had a complete blood count (CBC) and ESR, liver function tests (LFTs), microscopic stool examination, E.HIA Test and a chest xray. CBC, ESR and LFTs were repeated every 3 days. Abdominal ultrasonography and chest x-ray were repeated on the 10th day or earlier if a complication was suspected. Blood culture weas done only in patients suspected of having a pyogenic liver abscess on pus aspiration.
Liver abscess was aspirated only if there was a suggestive history of pyogenic abscess, multiple abscesses on ultrasonography, imminent rupture, left lobe abscess or failure to respond to 3-5 days of medical therapy.
Treatment Protocol Group A
All patients suspected of amoebic liver abscess were treated with metronidazole 500 mg intravenously x 8 hourly initially, followed by 400 mg x 8 hourly, as soon as the patient was well enough to tolerate oral medication. Metronidazole was given for 10 days. In the event of a complication, such as rupture treatment was more prolonged.
Group B
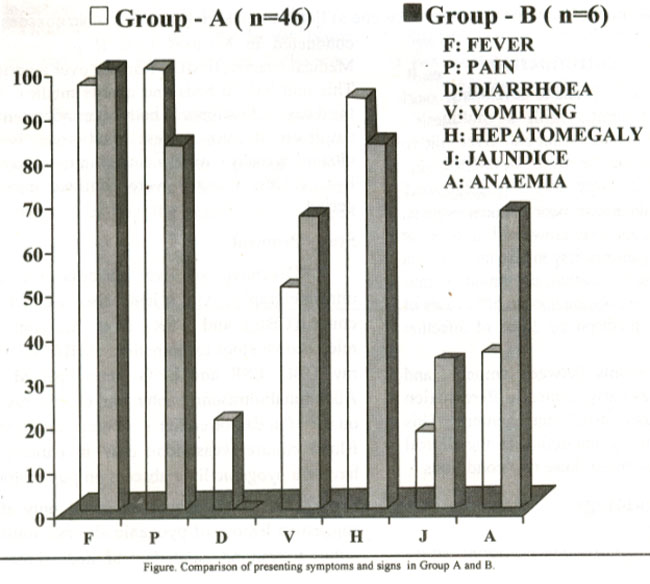
If the aspirate was purulent Cefotaxime ig iv x 8 hourly was administered until the results of culture and sensitivity were available. Antibiotic was appropriately revised in accordance with the sensitivity report. Patients were followed up for changes in symptoms and signs including fever pain, vomiting, diarrhoea, hepatomegaly, jaundice and anaemia.
Results
A total of 52 patients were registered during the one year study period. Amoebic liver abscess was diagnosed in 46 (88%) patients and 6 patients (12%) had pyogenic liver abscess. Age ranged from 13-70 years in group A with a mean age of 38.9 years, while it was 27-50 years in group B with a mean age of 42.6 years . Overall male to female ratio was 8:1; in group A it was 7:1 while in group B all patients were male. In group A only 9 patients (20%) had a history of dysentery or diarrhoea at the time of admission, while none of the patients in group B had diarrhoea (Figure). One patient in group B had diabetes, whereas no patient gave any history of taking steroids or any other immunosuppresive drug or interventional procedure. Pyrexia was recorded in almost all patients in both groups. Pain in the right hypochondrium was a dominant symptom in all patients in group A and 83% of the patients in group B (Figure). Approximately half the patients in each group complained of vomiting. Mean duration of symptoms in group A was 20 days while in group B it was 12 days.
Jaundice was infrequent in group A with only 8 patients exhibiting clinical jaundice whereas 3 out of 6 patients had jaundice in group B. Hepatomegaly was present in majority of patients in both groups (Figure).
Investigations showed a statistically significant difference between the mean haemoglobin level in groups A and B (Table 1). Leucocytosis was present in almost all patients of both groups, the difference being not significant. Mean ESR and alkaline phosphatase were elevated in both groups without a statistically significant difference.
There was a significant difference in the mean bilirubin level with a higher mean bilirubin level in group B (Table 1).
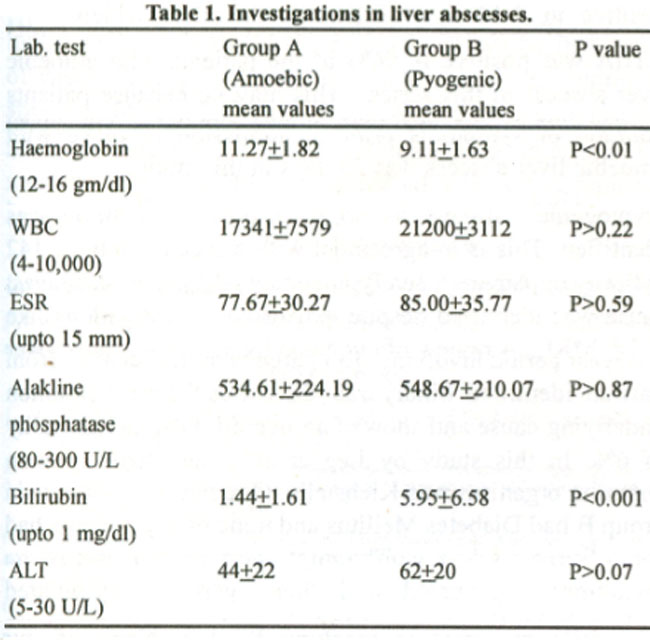
Minimal elevation of ALT was noted in both groups. Examination of faeces showed cysts and trophozoites of Entamoeba Histolytica in 10 (22%) patients in group A.
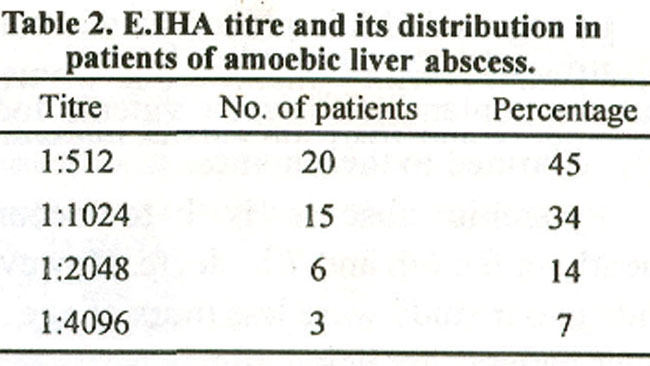
E.IHA was positive in 44 patients (96%) in group A and it was negative in all 6 patients of group B (Table 2).
Chest x-ray showed a raised right hemidiaphragm in 13 patients of group A (28%) and 1 in group B. A right sided pleural effusion was present in 10 patients in group A and 1 patient in group B. Ultrasonography confirmed liver abscess in all patients with majority of abscess in both groups being located in the right lobe (Table 3).
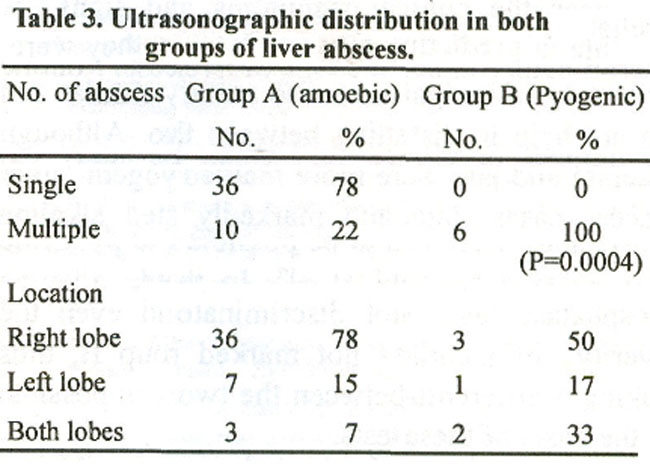
A total of 25 patients had their liver abscess aspirated, including all patients in group B. All patients in group B had multiple abscesses, whereas only 10 patients in group A had multiple abscesses, including 2 patients who also had secondary bacterial infection. The difference in percentage of multiple abscess between the two groups showed a statistically significant result (P = 0.0004), when tested by Yates corrected chisquare (12.21). Culture results in group B revealed E.Coli in 4 patients, Klebsiella Pneumoniae in one and Pseudomonas Aeroginosa in one patient. Blood culture was done in all patients of group B and 2 patients in group A, and was negative in all, Pleural rupture occurred in one patient in group A and peritoneal rupture in one patient in each group. There was no fatality in either group.
Discussion
The ratio of amoebic liver abscess to pyogenic liver abscess depends upon the geographical location of the reporting institution. Amoebic liver abscess is much more common in Pakistan as compared to pyogenic abscess1,4. It is also the most common form of extra-intestinal amoebiasis, occurring in 3-9% of infected patients5. E. Histolytica largely affects inhabitants of tropical and subtropical countries. Recent reports suggest some resurgence of amoebic liver abscess in the Western Countries also, believed to be caused by increased immigration, over crowding and poor living conditions5,6. Wide spread use of imaging techniques have also resulted in increased detection of pyogenic abscess in the liver which may have remained undiagnosed otherwise7.
The ratio of amoebic to pyogenic liver abscess in this study is consonant with other studies from this region1,3,4. The age and sex distribution in this series is also similar to other studies from this region7,8. Male predominance may be attributed to the different lifestyles of men and women of this country with menfolk going out to work and consuming contaminated water and unhygienic food from street vendors and roadside eateries, while the women are largely confined to their homes.
Pyogenic abscess is believed to occur more frequently in the 6th and 7th decade of life. However, all 6 patients in our study were less than 50 years of age. Recent studies suggest that there may be a shift of age so that younger patients are being affected7,9.
Whereas the clinical symptoms and signs were fairly reliable in predicting a liver abscess, they were not discriminatory in defining the type of liver abscess. Routine laboratory investigations were also remarkably similar and did not help in distinguishing between the two. Although the number of cases were very small in this study but anaemia and jaundice were more marked in pyogenic liver abscess cases. Jaundice and markedly elevated alkaline phosphatase were reported to be possible clues to pyogenic liver abscess by Reginald et al7. In this study alkaline phosphatase level was not discriminatory and even the severity of jaundice was not marked in group B, thus making a differentiation between the two types impossible on the basis of these two tests.
Neutrophilic pleocytosis is present in both types of liver abscesses. All patients with pyogenic abscess in this study had multiple liver abscesses, with a statistically significant difference between the two groups. It appears that the strongest indicator of a liver abscess being pyogenic is its multiplicity. Therefore all liver abscesses that are multiple on ultrasonography should be aspirated to establish the diagnosis of a pyogenic abscess by culturing the organism. A suspected amoebic liver abscess can be treated without aspiration unless it is large, threatens to rupture or is in the left lobe6.
The yield of trophozoites in the amoebic pus is poor. Neverthless confirmation of diagnosis would require isolation of organism from the aspirated pus. Indirect evidence of infection can be provided by serological tests for E. histolytica. A positive serological test for E.histolytica antibodies is highly predictive of current invasive disease in non-endemic areas . Conversely a negative serology in an endemic area is very useful in excluding the possibility of invasive amoebiasis, A positive serology requires more thorough clinical and diagnostic correlation in endemic areas10. Antibodies to E.histolytica are detected in more than 85-95% of patients with invasive amoebic colitis or amoebic liver abscess”. However, the initial serology may be negative in acute invasive amoebiasis and like all serological tests may become positive in 7-14 days. E.IHA is the most widely used serological test for invasive amoebiasis6,12. The initial E.HIA was positive in 96% of the patients with amoebic liver abscess in this series. This may be because patients present late to the hospitals in this country. The mean duration of symptoms prior to admission in those with amoebic liver abscess was 20 days in this study.
All 6 patients of pyogenic abscess in this series had cryptogenic abscess as no predisposing condition was identified. This is in agreement with a recent study of 142 patients in America by Reginald et al.7, where the vast majority of patients had cryptogenic pyogenic abscess as no cause was identified despite exhaustive investigations like CT & MRI . A review of pyogenic liver abscess cases over a 10 year period involving 133 patients by Lee et al.12 from Taiwan identified biliary tract disease as the most common underlying cause and showed an overall hospital mortality of 6%. In this study by Lee et al.12 the most common associated disease was diabetes mellitus and the most common organism was Kiebsiella. One out of 6 patients in group B had Diabetes Mellitus and none of our patients had any biliary tract disease. The most common organism in our small series was E.Coli. Only one case of Kiebsiella pneumoniae occurred and there was no associated endophthalmitis as reported by other authors with Kiebsiella pneumoniae serotype K114-16. None of our patients had underlying cirrhosis or carcinoma of liver17,18 in keeping with the lower incidence of liver abscess in cirrhotic livers. None of our patients were treated with continuous percutaneous drainage or surgical drainage or irrigation as reported by other authors13,19,20. Pyogenic liver abscess should be confirmed by culturing the organism from aspirated pus as a positive liver pus culture with a negative blood culture is common7. In this study blood culture was negative in all 6 cases where pus culture had a positive yield. An audit of pyogenic liver abscess in 133 patients by Alvarez et al.21 identified poor prognostic variables, as the presence of clinical shock, low haemoglobin, elevated prothrombin time and polymicrobial infection and a positive blood culture.
The absence of fatality in this study could be attributed to prompt diagnosis and specific effective treatment and the small number of patients who did not have the adverse prognostic factors identified by Alvarez et al.12.
Majority of liver abscess in this series were amoebic in nature, This infection largely afflicts males because of their particular lifestyles as opposed to women who are largely house bound. It was not possible to clearly differentiate between amoebic and pyogenic abscesses on clinical grounds or routine tests. Although aspiration of the pus is diagnostic, it is not always feasible. Serology for E.
Histolytica may be very valuable in establishing the diagnosis of amoebic liver abscess as shown by this series of cases. A high index of suspicion , early institution of specific medical therapy and aspiration of abcesses especially when multiple, have all contributed to an accurate diagnosis, a low complication rate and nil mortality in this study as compared with other reported studies.
References
1.Shaikh Z, Khan MH, Qamar R. Clinical profile of 100 cases of liver abscess. J.Pak.Med.Assoc., 1 989;39:256-59.
2.Rustgi AK, Richter JM. Pyogenic and Amoebic liver abscess. Med. Clinics of North America. 1989;73:847-58.
3.Goh KL, Wong NW, Paramsothy M, et al. Liver abscess in Tropics. Postgrad. Med. J., 1987, 63:551-54.
4.Hayat Z. Mahmood S, Ali M, et al: Liver abscess not a uncommon disease. J. Postgrad. Med. Inst., 1995; 9:56-61.
5.Moazam F, Nazir Z. Amoebic liver abscess: spare the knife but save the child. J. Paediatr. Surg., 1998;33: 119-22.
6.Weinke T, Grobusch MP, Guthoff W. Amoebic liver abscess: rare need for percutaneious treatment modalities. Eur. J. Med. Res., 2002;7:25-29.
7.Seeto RK, Rockey DC. Pyogenic liver abscess, changes in etiology, management and outcome. Medicine, 1996;75: 99-113.
8.Yeoh KG, Yap I, Wong ST, et al. Tropical liver abscess. Postgrad. Med. J., 1997; 73:89-92.
9.Land MA, Moinuddin M, Bisno AL. Pyogenic liver abscess: changing epidemiology and prognosis. South Med. J., 1985;78 1426-30.
10.Ravdin JI. Diagnosis of invasive amoebiasis, Gut., 1994;35:1018-21.
11.Ravdin JI. Amoebiasis. Rev. Clin. Infect. Dis., 1995; 20:1453-66.
12.Ellen L, Samuel L, Stanley Jr. Amoebiasis. Gastroenterol. Clin. N.America., 1996; 25:471-92.
13.Lee KT, Wong SR, Sheen PC. Pyogenic liver abscess: an audit of 10 years experience and analysis of risk factors. Dig. Surg., 2001;186:459-65.
14.Tan YM, Chong CK, Chow PK. Pyogenic liver abscess complicated by endogenous endophthalmitis : ANZ. J. Surg., 2001;71:744-46.
15.Fung CP, Chang FY, Lee SC, et al. A global emerging disease of Kiebsiella pneumoniae liver abscess: is serotype KI an important factor for complicated endophthalmitis? Gut, 2002; 50:420-24.
16.Wong TY, Chiu SI, So MK, et al . Septic metastatic endophthalmitis complicating Klebsiella pneumoniae liver abscess in a non-diabetic Chinese man. Hong Kong Med. .,J 2001;7:303-6.
17.Kuo CM, Kuo CH, Changchien CS. Liver abscess in patients with cirrhosis of the liver: a 12 year experience. J. Gastroenterol., 2001;36:552-56
18.Molle I, Thulstrup AM, Vilstrup H, et al. Increased risk and case fatality rate of pyogenic liver abscess in patients with liver cirrhosis: a nationwide study in Denmark. Gut, 200l;48:260-63.
19.Zenda T, Kaizaki C, Sato H, et al. Irrigation of liver abscess: proposal of a novel method and possible indications. Hepatogastroenterology, 2001 ;48:847-50.
20.Sharma MP, Ahuja V. Management of amebic and pyogenic liver abscess. Indian J. Gastroenterol., 2001 ;20:33-36.
21.Alvarez Perez JA, Gonzalez JJ, Baldonedo RF, et al. Clinical course treatment and multivariate analysis of risk factors for pyogenic liver abscess. Am. J. Surg., 2001; 181:177-86.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: