
N.A. Rao ( Ojha Institute of Chest Diseases, Karachi. )
M. A. Sadiq ( Ojha Institute of Chest Diseases, Karachi. )
November 2002, Volume 52, Issue 11
Original Article
Abstract
Objective: To determine the radiological presentation of pulmonary tuberculosis in adults and to compare it with that of other national and international studies.
Method: This prospective study was done on 150 newly diagnosed smear positive pulmonary tuberculosis patients. Two chest physicians reviewed the chest radiographs. Those x-rays were selected in which there were no difference of opinion.
Results: There were 77 male and 73 females. The average age was 3452 years with range of 17 to 80 years. Out of 150 films, eighty-seven (58%) showed the typical pattern (infiltration and / or nodules with or without cavitations, involving upper zone). While sixty three (42%) showed the atypical pattern (pattern other than typical one).
Conclusion: Typical pattern of pulmonary tuberculosis is still the common mode of presentation in adults but there is a trend toward increase in atypical pattern (JPMA 52:501:2002).
Introduction
Pulmonary tuberculosis is generally classified into primary and post primary tuberculosis, both have distinct characteristic on radiology. Post primary tuberculosis is the commonest form in adults, in which the patients usually present with infiltration with or without cavitations involving the apical and posterior segment of upper lobe1-3. In some cases the apical basal segment of the lower lobe is the first to be involved. The other lobes may be involved but classically follow involvement of the upper lobe. Based on these characteristics, pulmonary tuberculosis is divided into typical or usual pattern and atypical or unusual pattern.
In the typical pattern, there is upper zone involvement in the form of infiltration or nodules with or without cavitations. In the atypical pattern all other forms are included e.g. lower lung field tuberculosis, hilar lymphadenopathy, miliary tuberculosis, diffuse pulmonary tuberculosis, tuberculoma, atelectasis, pleural effusion, pnemothorax etc.
The object of the study was to determine the current radiological presentation of pulmonary tuberculosis and to compare it with that of other national and international studies.
Material and Method
This prospective study was done between August 2000 and November 2000, in patients attending Nazimabad and Malir Chest clinics of Ojha Institute of Chest Diseases, Karachi. We included those cases that were diagnosed as smear positive pulmonary tuberculosis and the fresh chest X-rays were available These Chest radiographs were reviewed by two chest physicians. Only those X-rays were selected in which there were no difference of opinion.
Results
A total of 150 patients were included in the study, seventy-five from each clinic. There were 77 male and 73 females. The average age was 34.52 years with range of 17 to 80 years.
Out of 150 films, eighty-seven (58%) showed the typical pattern and sixty three (42%) showed the atypical pattern. Among the typical, 65 films (74.71%) had unilateral and 22 films (25 .28%) had bilateral disease.
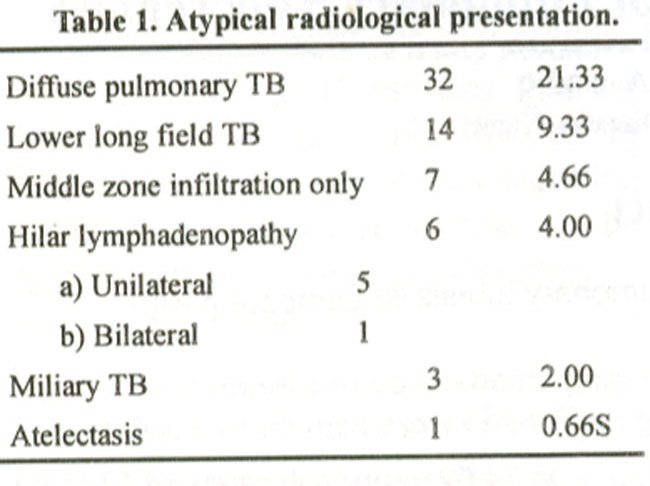
Table 1 shows the distribution of atypical radiological pattern.
Discussion
Although the gold standard for the diagnosis of pulmonary tuberculosis is isolation of mycobacterium tuberculosis from respiratory secretions but chest X-ray is equally important in the diagnosis. There are a number of cases in which there is no expectoration or in which the disease is minimal or who cannot just bring their sputum up. In such cases we rely on clinical and radiological features.
It is well known that tuberculosis can be included in the differential diagnosis of almost any pulmonary case, so knowledge of radiological presentation of pulmonary tuberculosis is beneficial for the practicing physicians.
In this study 58% of the patients presented with typical radiological pattern, which mean still the majority of the patients present with typical pattern.
In 1993, Javaid K. et al4 reported the typical pattern in 76% of culture positive pulmonary tuberculosis cases. In 1997, Saulatullah et al5 reported the typical pattern in 60% of Diabetic and 70.7% of non-diabetic patients. In our series only 10 patients were diabetic, out of which 3 (30%) presented with typical pattern and 7 (70%) with atypical pattern.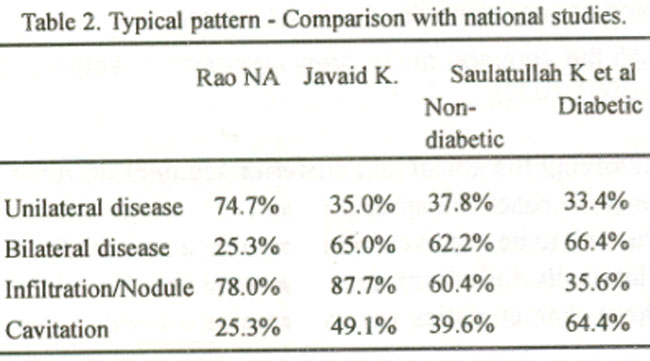
Table 2 compare the pattern of lung involvement in patients presenting with typical chest X-ray. In this study unilateral disease was more common than other two locally reported studies.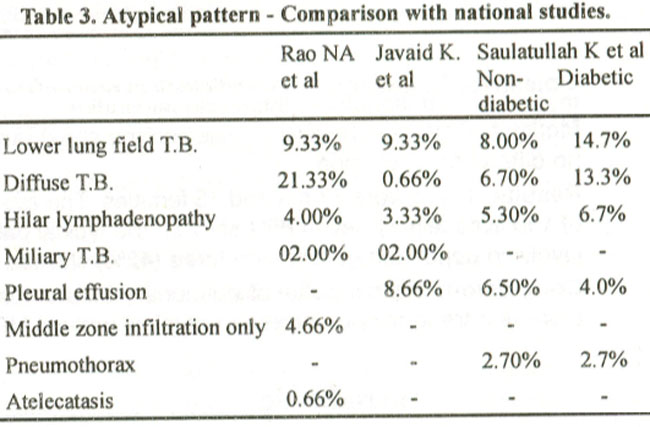
Table 3 compares the atypical pattern. The higher presentation of diffuse pulmonary tuberculosis in this study i.e., 21.33% is noteworthy, while Javaid K reported just
0.66%4. The inclusion criteria of the patients reported by Javaid K was culture positive pulmonary tuberculosis, and thefr patients usually belong to higher socioeconomic group and they consult medical services earlier. Our patients belong to the poor community and for them daily earning is top priority than their health. So they seek medical advice late.
Pleural effusion has not been reported in any case in this study because our cases were smear positive for pulmonary tuberculosis. Middle zone infiltration only was noted in 4.66% cases, which most probably represents apical basal segment, which is also the common site of post primary pulmonary tuberculosis.
One of the patients presented with atelectasis and was smear positive, which indicate endobronchial tuberculosis with or without lymph node enlargement. While comparing this study with internation ones the atypical pattern, lower lung field pulmonary tuberculosis was from 5.31% to 7%6-8, hilar tymphadenopathy from 7.44% to 9.7%7,9 and military tuberculosis 4.5%6.
In 1998 Vanden BP et al reported an increase in unusual presrntation of tuberculosis from 24% in 1981-85 to 35% in 1986-9010, but this study was from Belgium where tuberculosis is well under control. We are observing the same phenomenon of incease in unusual presentation in this part of the world where tuberculosis is highly prevalent. In this regard it is suggested that radiological presentation of pulmonary tuberculosis must be stressed during undergraduate training. This is important because in post sanatorium era, emphasis on tuberculosis teaching has been declining. A study was carried out to determine the fact. In that study11 44% of the patients was undiafnosed on admission despit of the fact that majority of them had characteristic chest X-ray findings. This likelihood is greater when the patient present with atypical radiological pattern.
Conclusion
Typical pattern of pulmonary tuberculosis is still the common presentation in adults but there is a trend toward increase in atypical pattern. It is suggested that medical students and practicing physicians must also be aware of atypical presentation.
References
1.Fraser RG, Pare JAP, Diagnosis of diseases et Chest. Vol. II, pinladelpinta. WJ3. Saunders Co., 1979w pp 731-49.
2.Hinshaw HC, Murray IF. Tubercurasis. In: Diseases of the cheE, 4th Ed. Phladelpataa. WB Saunder Co., 1980, pp 298-355.
3.Simon Pg, padley, Michaci BR Pulmonary infections in David S. Ed Textbook et radiology and Lri 2007 6th ed. Edinburg Churchil Livindstrate. 1998, pp. 421-49.
4.Javed K, Najmal I, Khurram F, et al. Chest radiographic findings of tuberenlosis ir. Pakistani adults. Pak. Med. Sei,, 1 993.10.5-9
5.Saulatullab K. Tahira MC. Tariq M. et aL A Comparative gucty of radiological pattern of pulrnonai tuberculosis in ciabeues Versus non.diabetics. PakJMcd Res., 1997,36:55-57.
6.Khan MA, Kuvnat DM, Hrucc B. et al. Clinical and roentogenographic spectrum of pulmonary tuberculosis in the adult. Am J. Med., 1977: 6231-38.
7.Krysl J, Korzeniewska -Kosela M. Muller NL, ct al Radiological features of pulmonary tuberculosis an assessment of 1S8 cases. Can Assoc Radiol. J., 1994; 45:101-7.
8.Farman DP. Spcir WA Initial roentgenographic manifestation of bacteriologically proven mycobacterium tuberculosis. tuberculosis. : Typical or Chest, 1986;89:75-77.
9.Choyke PL. Sostman HD, Curtis AM, et al Adult-onest pulmonary tuberculosis. Radiloogy. 1983;148:357-62.
10.Vanden Brande P, Dock S, Valck Bet al. pulmonary tuberculosis in the adult in the low prevalence area Is the radiological prcscntation changing? Int. 3 Tuberel. Dis.,1998;2 904-8.
11.Mac Gregor RR: year\'s experience with tuberculosis in a private urban eaching hospital in the postsanatorium era. Am J. Med,, 1975,58 221.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: