
B.S. Ali ( Departments of Community Health Sciences, The Aga Khan University, Karachi. )
M.H. Rahbar ( Departments of Community Health Sciences, The Aga Khan University, Karachi. )
S. Naeem ( Departments of Psychiatry, The Aga Khan University, Karachi. )
A.L. Tareen ( Departments of Community Health Sciences, The Aga Khan University, Karachi. )
A. Gui ( Departments of Community Health Sciences, The Aga Khan University, Karachi. )
L. Samad ( Departments of Community Health Sciences, The Aga Khan University, Karachi. )
November 2002, Volume 52, Issue 11
Original Article
Abstract
Objective: To study the prevalence of, and factors associated with anxiety and depression among women.
Design: A cross sectional survey.
Setting: A lower middle class semi -urban community of Karachi, Pakistan.
Participants: A total of 1218 women between the ages of 18-50 years.
Methodology: Systematically every third household was identified from which a woman was randomly selected. The Aga Khan University Anxiety and Depression Scale and a socio-demographic questionnaire were administered verbally by trained interviewers for assessing the prevalence of, and associated factors for anxiety and depression.
Results: A prevalence of 30% was found. Increasing age, lack of education and verbal abuse were the associated factors found to have an independent relationship.
Conclusion: Providing education and reducing domestic abuse could lead to decrease in the prevalence of anxiety and depression in women (JPMA 52:513;2002).
Introduction
World-wide 480 million people are estimated to be suffering from depression and a quarter of these have anxiety as well1. Over ninety percent of mental health problems in the community are anxiety and depression and co-morbidity is common2. Their combined prevalence is taken as a measure of the magnitude of mental illness in a community3 and the enormous universal burden . of depression has been reported in several studies. Two thirds of the affected are living in the developing countries, and this ratio is expected to rise due to the rapid population growth, urbanization and strong links between adverse socio-environmental factors and prevalence of mental illness4-12.
Studies conducted in Pakistan have revealed a high prevalence of anxiety and depression on the whole with more than double the prevalence in women, and a higher prevalence in rural compared to urban areas13-16. Some of the psycho-social risk factors for depression identified among women living in Karachi are very early marriage, hostile in-laws and lack of an intimate and confiding relationship with the husband17.
Pakistan is a developing country with an estimated population of 140 million. About 70% of the population is rural based and dependent on agriculture for its livelihood. Persisting drought over the last few years has forced people to urban areas in search of employment18. Karachi is a mega-city with a population of more than 14 million of which 40% live in squatter settlements where over crowding; unemployment, poor civic amenities and rapidly changing social structure are common. Women are in double jeopardy because of their illiteracy, domestic violence and loss of extended family19.
This survey was carried out to identify women who were anxious and depressed for a community based interventional study being conducted in Qayoomabad one of the lower middle class semi-urban community of Karachi. This paper reports the baseline data collected before initiation of the main study.
Methodology
A cross-sectional survey was carried out in Qayoomabad which has a population of about 80,000, from January 8 - February 14, 2001, to identify women suffering from anxiety and depression. Systematically every third household was identified from which a woman meeting the inclusion criteria was randomly selected. The inclusion criteria were: informed consent, age 18-50 years, able to understand the local language Urdu, planning to live in Qayoomabad for at least one year, and not having suffered a bereavement in the last six weeks.
The Aga K1ian University Anxiety and Depression Scale (AKUADS) was used as the assessment tool. It is an indigenously developed and validated screening instrument that has been used in several studies20-23.
AKUADS was administered verbally by trained interviewers. A questionnaire covering the sociodemographic characteristics and potential factors associated with anxiety and depression was also administered. Pretesting was carried out at a field site with socio-economic and cultural environment similar to the study area.
Data was entered using Epi-Info package following standard double entry procedure; 10% of the records were compared and the error rate detected was 0.03%. Data was analyzed using the statistical software package SPSS,
version 10. The descriptive analysis provides important information about the study population. Univariate and multivariate logistic regression models were used to estimate the crude and adjusted odds ratios and their confidence intervals.
Results
Overall 1226 women were interviewed. Out of these women, 8 were excluded from the sample, as their age was less than 18 years. Finally a sample of 1218 women was analyzed of which 366 were identified to be anxious and depressed. This provides an estimate of 30% for the overall prevalence of anxiety and depression in this population. Mother tongue (language spoken at home) was used as a surrogate marker for ethnicity and immigration. Five ethnic groups were identified; Hazarawalas, Pathans, Punjabis, Urdu speaking and others (Gujrati/Sarieki). In the entire study population (1218 women), 430 were Hindko speaking, out of the later 140 (32.6%) were found to be cases. Similarly of the 155 Pushto spreaking 58 (37.4%), of 421 Punjabi spreaking 113 (26.8%), of 196 Urdu spreaking 52 (26.5%), of 16 Gujrat/Sarieki speaking 3 (18.8%) were found to be cases.
Among the 366 anxious and depressed women identfied, 140 (38.3%) were Hindko speaking, 113 (30.9%) spoke Punjabi, 58 (15.8%) were Pushto speaking, 52 (14.2%) were Urdu speaking and 3 (0.8%) spoke Gujrati/Sarieki) (They have been grouped together as their number are too small to influence the results.
Majority of the residents (86.5%) had houses of concrete construction, 47% had three or more than three living rooms, almost all the households (98.4%) had Sui gas and electricity (99.4%). Households with a television were 75.3%, with a motorcycle or a car were 20.2% and with a telephone were 26%. These possessions were used as proxy indicators for socioeconomic status as used in the National Health Survey of Pakistan24. According to these criteria 4.5% belonged to the high socioeconomic class, 78.2% to the middle and 17.2% to the low socioeconomic class.
The baseline characteristics of the population are provided in Table 1.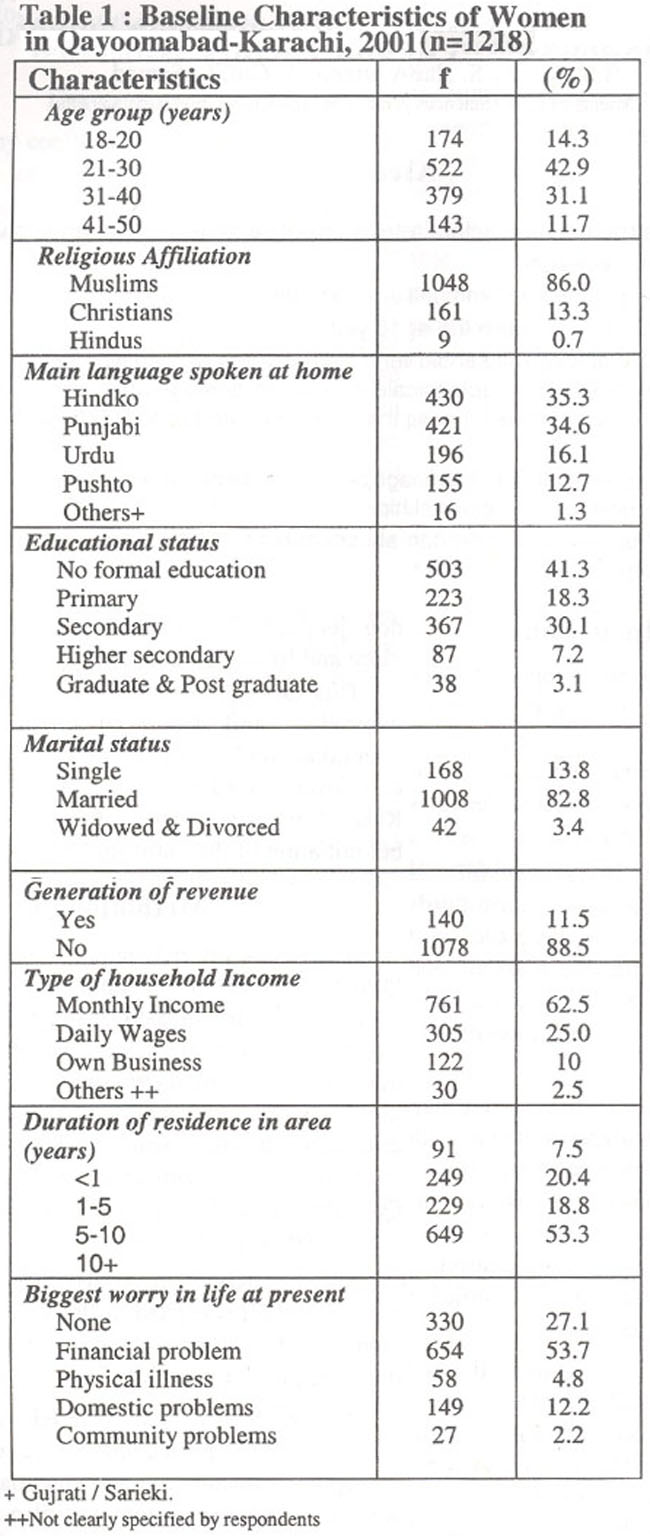
The mean age was 30.7 years with the standard deviation of 8.3. The majority of the women were migrants from other areas of Pakistan as only 16.6% considered Urdu as their first language. The mean number of children in the family was 4.7 with a standard deviation of 2.8. Contraception was practiced by 44.5% of women.
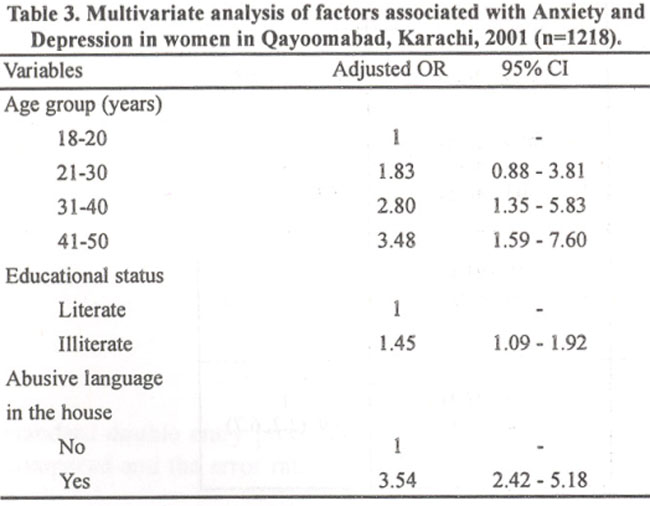
Factors associated with anxiety and depression in the univariate analysis are summarized in Tables 2 and 3 list the factors that remained significant in multivariate analysis.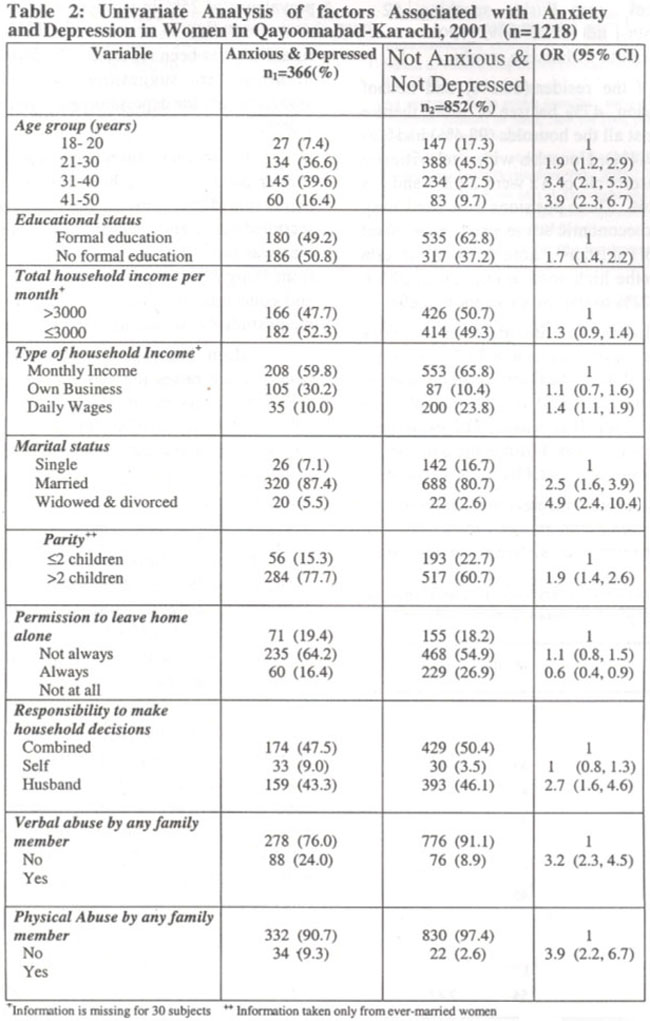
Discussion
The prevalence of anxiety and depression is universal, but varies in different countries, environments, between sexes and different ages. A community based study of prevalence in women done in urban Zimbabwe25 reported a figure of 30.8% and another in urban Mumbai 25-28%26. A prevalence of 25% in women of urban Rawalpindi16 has been shown, these figures are close to our finding of 30%. Prevalence of 46% among women in Chitral13 and 66% in rural Punjab14 has been reported, which is much higher than in urban women, suggesting the possibility that the associated factors for depression are more prevalent in rural women.
A crossectional study conducted in 199615 in a similar community in Karachi had reported a prevalence of depression in 42% women, but the subjects were not recruited randomly and according to authors a self-selection bias was possible. A prevalence of only 17.6% is reported from Banglore26, which is known for its high literacy rate and education and has been found to confer protection in many studies13,16,27 including ours (p <0.001).
Education improves coping mechanisms in more than one-way; it raises the self-efficacy and therefore the self-esteem of women. It also makes women feel less helpless in difficult situations and gives a greater sense of control over their environment28.
The lowest prevalence was found in the local population (Urdu as mother tongue) lending credence to immigration being an associated factor for depression10.
Prevalence of depression rises with age15,16,29 which is similar to our finding, of a 5% increase in the odds of becoming anxious and depressed for every one year increase in age. Marital status and parity have been identified as associated factors consistently in studies carried out in Pakistan13,27 and this is supported by our study as well.
The retention of verbal abuse and the elimination of physical abuse in the multivariate model is noteworthy as it indicates that emotional trauma is worse than physical30. Financial difficulty was found significant in the univariate analysis but it did not come out as an independent factor in our multivariate model indicating that depression is not just an inventory of poverty.
Compared to women who could go out unescorted, the women who always had to be escorted were less likely to be anxious and depressed. This finding probably indicates that culturally women who are escorted feel more secure and cared for.As Qayoomabad is predominantly a lower middle class semi-urban community in Karachi, the results can be generalized to similar settings. To avoid interpreter bias only women who could understand Urdu were included which could be responsible for a bias in interpreting prevalence in different ethnic groups.
Educating women, enabling them to generate revenue and reducing verbal abuse could lead to decrease in the prevalence of anxiety and depression.
Currently a study is underway to assess the effect of counselling by briefly trained community counsellors on levels of anxiety and depression in women identified in this survey. The results will be reported in a subsequent paper.
Acknowledgements
We wish to thank the University Research Council of The Aga Khan University and the women of Qayoomabad without whose help this study would not have been possible.
References
1.Broadhead WE, Blazer DO, George LK, et al. Depression disability days and days lost from work, a perspective epidemiological survey. JAMA; 1991 ;5:281-85.
2.Goldberg D, Bridges K, Cook D, et al. The Influence of Social Factors on Common Mental Disorders: Destabilization and Restitution. Br. J. Psychiatr., 1990;156:704-13.
3.Goldberg D. Identifying psychiatric illness in general medical patients. BMJ.,1985;291:161-62.
4.Holden C. Global survey examines impact of depression. Science, 2000;288:39.40.
5.Desjalais R, Eisenberg L, Good B, et al. World mental health - problems and priorities in low -income countries. New York: Oxford University Press, 1995.
6.World Bank. World Development Report 1993 - Investing in Health. Oxford, England: Oxford University Press, 1993.
7.Murray CJL, Lopez AD, Eds. The global burden of disease. Comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and projected to 2020. Cambridge MA, Harvard School of Public Health on behalf of the World Health Organisation and the World Bank, 1996.
8.Saraceno B. 2001 - a landmark year for world mental health. J. Coil. Physicians Surg., 2001;11:190-91.
9.World Health Organization. Health trends and emerging issues in 1990s and 21st century, Geneva, monitoring, evaluation and project methodology unit, WHO, 1991.
10.Blue I, Harpham T. Urbanization and mental health in developing countries: current issues in public health, 1996;2:181-85.
11.World Health Organization. The World Health Report 1999 - making a difference. Geneva, Switzerland: World Health Organization; 1999.
12.World Health Organization. Director General’s Report: a corporate strategy for WHO. Geneva: WHO, 1999.
13.Mumford DB. Stress and psychiatric disorders in the HinduKush. A community survey of mountain village in Chitral, Pakistan: Br, J. Psychiat., 1996; 168:229.307.
14.Mumford DB, Saeed K, Ahmad I, et al. Stress and psychiatric disorders in the rural Punjab: Br. J. Psychiatr., 1997;170:473-78.
15.Ali BS, Amanullah S. Prevalence of anxiety and depression in an urban squatter settlement of Karachi: J.Coll.Physicians Surg.Pak., 2000; 10:4-6.
16.Mumford DB, Minhas FA, Akhtar I, et al. Stress and psychiatric disorder in urban Rawalpindi: community survey Br. J. Psychatsy, 2000;177:557-62.
17.Naeem S. Vulnerability factors for Pakistani women: J.Pak.Med.Assoc.,l992; 42:137-38.
18.An overview of the economy: economic survey of Pakistan. A pre-budget document released on Saturday, June the 16th, published in the Daily Dawn on Sunday June 17th 2001.
19.Hassan KZ. Practice of psychiatry in the developing countries in the new millennium. J.Coll.Physicians Surg. Pak., 2001;11:206-7.
20.Ali BS, Reza H, Khan MM, et a!. Development of an indigenous screening instrument in Pakistan: The Aga Khan University Anxiety and Depression Scale: J.Pak.Med.Assoc., 1998;48:261-65.
21.Mumford DB, Tareen IAK, et al. The translation and evaluation of an Urdu version of The Hospital Anxiety and Depression Scale. Acta. Psychiatr. Scand., 1991; 83: 81-85.
22.Ali BS. Validation of an indigenous screening questionnaire for anxiety and depression in an urban squatter settlement of Karachi: J.Coll.Physicians Surg.Pak., 1998;8:207-1 1.
23.Rabbani F. Views about women’s mental health: study in a squatter settlement of Karachi: J.Pak.Med.Assoc., 1999;49:139-42.
24.National Health Survey of Pakistan 1990-94, p. 163.
25.Broadhead JC, Abas AM. Depression and anxiety among women in an urban setting in Zimbabwe. Psychol. Med.,1997; 27:59-71.
26.World Health Organization. The World Health Report 2001: Mental health: new understanding, new hope. Geneva, Switzerland: World Health Organization; 2001.
27.Dodani S, Zuberi WR: Centre-based prevalence of anxiety and depression in women of the Northern areas of Pakistan: J.Pak.Med.Assoc., 2000;50:l38-40.
28.Harpham T. Urbanization and mental health in developing countries: a research role for social scientists, public health professionals and social psychiatrists. Soc. Sci. Med.,1994;39:223-45.
29.Pillay AL, Sargent CA. Relationship of age and education with anxiety depression and hopelessness in a South African community sample: percept mot skills. 1999;89:881-84.
30.Evans, P. The verbally abusive relationship: how to recognize it and how to respond: Adams Media Corporation, 1992.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: