
Q. Fasihuddin ( Department of Urological Surgery and Transplantation, Jinnah Postgraduate Medical Center, Karachi. )
A.T. Hasan ( Department of Urological Surgery and Transplantation, Jinnah Postgraduate Medical Center, Karachi. )
November 2002, Volume 52, Issue 11
Original Article
Abstract
Objective: To study the effectiveness and complications of the use of ureteroscope in the management of ureteral calculi and as diagnostic modality for ureteric strictures and hydroureter.
Patients and Method: URS was carried out in 125 consecutive patients .Technical failure to negotiate the ureteric orifice was observed in 10 (8%) patients. Three of them had passive dilatation with ureteric catheter for 48 hours, while in 7, the failures were due to inability to traverse the ureter.This study will thus review 118 patients, 87males (73.7%) and 31 females (26.3%) with a mean age 38 years ± 12 years during 24 months. All the ureteroscopies were performed with a 8 FG rigid ureteroscope under G.A. Swiss (pneumatic) lithoclast was used for lithoripsy. Of the 118 patients, 98 calculi were treated, Five of these patients had associated ureteric strictures. Twenty patients underwent ureterorenoscopy for diagnostic purposes. Ten of them had ureteric strictures and in 10 patients dilated ureters with no luminal obstruction was found.
Results: Four (4%) of the stones were located in the upper, 13(13.2%) in middle and 81(82.6%) in the lower ureter. The size of the stones treated ranged between 6-22 mm. Clearance of stones within 48 hours and 15 days was observed in 66.3% and 93.8% respectively. Only 6.1% of the patients had failure to clear calculus after 30 days and repeat procedures were required. Four of the patients with ureteric strictures had ureteroneocystostomy while in 6 endoscopic dilatation was done. Thirty one and 10 patients had fever upto 38.5°C and more than 38.5°C respectively. Percutaneous Nephrostomy (PCN) placement was required in 2 patients and stripping of mucosa occurred in 1 patient. Mild hematuira was observed in 46 (38.9%) patients. Only 2.5% had moderate degree of hematuria after the procedure.
Conclusion: Considering the result from this study we suggest that URS is an effective interventional and diagnostic modality for ureteric diseases with a low complication rate (JPMA 52:51 0;2002).
Introduction
Ureteroscopy was first described by Young and Mc Kay in 19291 but not until the late 1970s was its clinical use demonstrated2,3 Currently, advances in ureteroscope design including fiberoptic visualization, flexibility and downsizing and improvements in calculus fragmentation ability, balloon dilatation and various baskets stents and wires have broadened ureteroscopic diagnostic and therapeutic capabilities4. This study reports two years local experience of this procedure.
Patients and Methods
From November 1999 through October 2001, one hundred twenty five patients underwent ureteroscopic procedures, at our institution. All the patients had preoperative assessment with detailed history and thorough physical examination. Laboratory investigations included blood complete examination, blood sugar, urea, serum creatinine and electrolytes. Urine complete analysis was performed in all patients and urine culture was performed when indicated. Pre-operative film of the kidneys, ureters and bladder and excretory urogram was done in all patients to document size and site of stone.
Pre-operatively gentamycin was given to all patients 30 minutes before and 4 more doses after the procedure. Oral Quinolone were prescribed subsequently from evening of 3rd post-operative day to 7th post-operative day. A plain x-ray KUB was taken in patients with stone disease to see any migration of stone. Preliminary urethrocystoscopy was performed in all cases to inspect urethra and bladder to exclude any pathology and identify ureteric orifices.
All the ureteroscopies were performed with a 8 FG rigid ureterorenoscope under G.A. Technical failure to negotiate the ureteric orifice in 1st place was observed in 10 (6.1%) patients. Three of them had passive dilatation with ureteric catheter for 48 hours, While in 7, the failures were due to inability to traverse the ureter. So this study will review 118 cases.
Swiss (pneumatic) lithoclast was used for lithotripsy. After fragmentation of stone, a ureteric catheter 5 F size was left in place for 48 hours as stent in 75 patients. DJ stent 4.7F was left in place for 4 weeks in 5 patients who had lithotripsy for stone and balloon dilatation for stricture of ureter. Among 18 non-stented patients, in 4 patients ureteric catheter was not placed as complete extraction of stone was possible and in 14 patients ureteric catheter and guide wire could not be manipulated through ureter.
All patients were followed up routinely after 48 hours for clearance of stone; repeat x-ray after 15 days was done if clearance was not observed after 48 hours, Patients with failure of clearance after 30 days were subjected to subsequent treatment session after 30 days of the initial procedure.
Of the 10 patients with ureteric strictures, 6 had endoscopic balloon dilatation while in 4 ureteroneocystosmy was performed. Patients were followed with excretory urography to assess the outcome of the procedure. In the remaining 10 patients only diagnostic ureteroscopy.was done and no intervention was carried out, Patients were observed for complications and managed accordingly.
Results
One hundred and twenty five consecutive patients were included in the study . Seven patients were excluded for the reasons stated above. Of 118 patients, there were 87 males (73.7%) and 31 females (26.2%) with a mean age 38± 12 years. Ninety eight patients had lithotripsy for stone disease and 20 patients ureteroscopy was done for diagnostic purposes.
Of the 20 patients (10 strictures, 10 dilated ureters with no obstruction) 4 with ureteric stricture disease had ureteroneocystostomy, as the strictures were complete and endoscopic manipulation was not possible.While in six balloon dilatation was performed and DJ stent was left in place for 4 weeks. Of the 10 patients who underwent inspection for obstructions of unclear etiology, all had normal examination except dilated ureter.
The size and site of the stone are outlined in Table 1.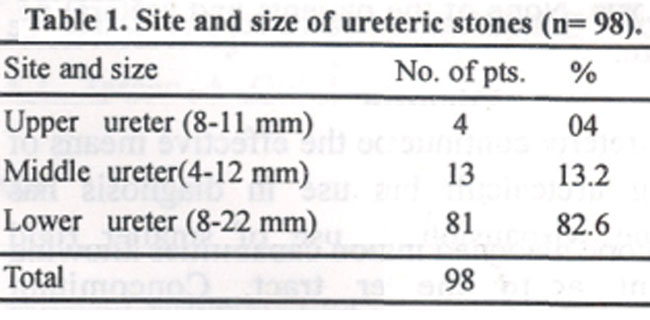
After single session of stone fragmentation, 93.8% of the patients had clearance of stone. Only 6.1% required two sessions. Overall 66.3% and 93.8% of the patients had complete stone clearance after 48 hours and 15 days respectively (Table 2).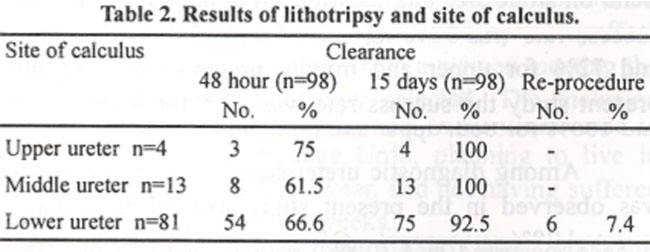
Fever was the commonest complication encountered in 56 (47.4%) patients, Out of these 56 febrile patients, majority 31(26.2%) had low-grade fever while 10 (8.4%) had fever more than 38.5°C. Hematuria was the other complication. Mild in 46 (38.9%), which settled within 12 hours and moderate in 2.5%, which settled within 48 hours. Distinction between mild and moderate hematuria was simply visual. None of the patient required transfusion.
PCN placement was required in 2 patients. One of the patients had stripping of mucosa of ureter, and the other was secondary to failure in stone clearance and pyonephrosis. None of the patients had ureteral perforation or septicemia. No death resulted from ureteroscopic procedure.
Discussion
Ureteroscopy continues to be the effective means of removing ureteral calculi but its use in diagnosis has undergone wide expansion. The use of smaller rigid ureteroscope has broadened inspection capabilities allowing consistent access to the upper tract. Concomitant downsizing of biopsy forceps, stone baskets, lithotripsy and laser probes for the decreased working port size enables effective treatment and diagnostic evaluation. These advancement and improvement in technique have caused an increase in overall diagnostic and therapeutic success from 86 to 96%5. In this study of 125 patients we found, overall success rate of the procedure in 118 (94.4%) patients. There were 7 failures in 125 ureteroscopic procedures. The failures were due to inability to negotiate the ureter.
Pneumatic lithotripsy, which is the most recent modality in the armamentarium for the treatment of ureteric stones6 is used for stone fragmentation. Four (4%) of the stones were located in the upper, 13 (13.2%) in middle and 81(82.6%) in the lower ureter. While Naqvi et.al7 in their series of 220 stones found 3% of the stones in upper, 11% in the middle and 86% in the lower ureter. Naqvi et.a17 and Hofbauer8 reported stone free rate at 4 weeks to be 95% and 89.5% respectively. In this study stone free rate at 4 weeks was 93.8%.
The success rates for ureteroscopic stone removal depend on stone size and location. In a large series of 346 ureteroscopic procedures performed at the Mayo Clinic, the success rate was 95% for removing lower ureteral stones and 72% for upper and middle ureteral stones9. In the present study the success rate was 92.5% for lower stone and 100% for both upper and middle ureteral stones.
Among diagnostic ureteroscopy, 100% success rate was observed in the present study while William et.al5 reported 98% success rate. Of the 118 patients, stripping of mucosa, occurred in 1 (0.8%) patient compared to 1.5% reported by Williams et al.5
Although fever was the commonest complication reported in 47.4%, but termperature >38.5°C was encountered in 8.4% patients only in the present series. This is comparatively higher than 1.9% reported by Williams et al5 and 2.9% reported by Peter et al10. One hypothesis may be that the higher percentage of fever compared to other studies may be due to external stenting but we have not been able to identify any specific factors that may be an evidence of the fact and more controlled trials are required for the establishment of the reality.
Hematuria was the second common complication observed in 41.5% patients while Naqvi et.al.7 found hematuria in 3.2% patients but the degree of hematuria was not mentioned.
Reported frequency of ureteral perforation was 1 (2.6%) patient in Hofbauer’s series8 and of 164 patients in Peter’s study, 1 (0.6%) acquired this complication. We did not come across this complication. It could be concluded from the study that URS is an effective and safe interventional and diagnostic modality for ureteric diseases.
References
1.Young HH, McKay RW. Congenital valvular obstruction of the prostatic urethra. Surg. Gynecol. Obstet., 1929; 48:509.
2.Lyon ES, Kyker JS, Schoenberg HW. Transurethral ureteroscopy in women: a ready addition to the urological armamentarium. J. Urol., 1978;119:35.
3.Perez Castro Ellendt, Martinez Pineiro JA.Transurethral ureteroscopy: a current urological procedure. Arch. Esp.Urol., 1980;33:445.
4.Watson GM, Landers B, Nauth Misir R, et al. Development in ureteroscopes, techniques and accessories associated with laser lithotripsy. World J. Urol.,1993; 11:19.
5.William JH, Peter DS, Michael LB, et al. Ureteroscopy: current practice and long term complications. .J Urol., 1997;157:28.
6.Management of ureteral calculi. ed. The debate continues. J. Urol., 1992; 48:1102.
7.Naqvi AA, Khaliq M, Zafar MN, et al. Pneumatic lithotripsy: a new modality for treatment of uretenc stones. J.Pak.Med.Assoc., 1995; 45:9.
8.Hofbauer J, Hobarth K, Marberger M. Electrohydraulic versus pneumatic disintegration in the treatment of ureteral stones: a randomized, prospective trial. J. Urol., 1995;153:623.
9.Blute ML, Segura JW, Patterson DE. Ureteroscopy. J. Urol., 1998;139:510.
10.Peter D, Sershon W, Joseph W. Rochester MN. Ureteroscopy: current indications and management. AUA eightyninth annual meeting, San Franscisco, California, USA. 14-19 May, 1994 abstract.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: