
Ayesha Ashraf ( Shifa College of Medicine, Islamabad, Pakistan. )
Mobeen Iqbal ( Shifa College of Medicine, Islamabad, Pakistan. )
November 2009, Volume 59, Issue 11
Case Reports
Abstract
Intra pulmonary sequestration is a rare congenital disorder that is characterized by malformation of pulmonary tissue having no connection to normal tracheobronchial tree and pulmonary arteries. This is a case history of 20 years old man initially misdiagnosed as Tuberculosis and later diagnosis of intra-lobar pulmonary sequestration was confirmed. There are few reports of this rare disorder globally and we are reporting the first case of Intrapulmonary Sequestration in Pakistan.
Introduction
Pulmonary sequestration is a rare malformation in which pulmonary tissue is formed with no connection to the normal bronchial system and the aberrant arteries arise from the systemic supply, either within the lung (intralobar) or as a separate adjunct (extra lobar).1 Pryce et al2 classified intralobar sequestration by the extent of blood supply from an aberrant systemic artery in 1947. Intralobar sequestration is diagnosed at age 20 years or younger in approximately 50% to 60% of cases, and is rarely found in patients older than 70 years.3 Diagnosis of sequestration requires a high index of suspicion. Intralobar sequestration diagnosed typically in juvenile patients is often misdiagnosed both because of a lack of recognition of chest radiographic findings and a low expectation of the disease.
Case Report
A 20 years old male presented with cough, haemoptysis and on and off fever for the last 3 years. Initially cough was white to yellow in colour but later patient developed frequent episodes of haemoptysis. There was no associated weight and appetite loss. Systemic examination was unremarkable. Patient was seen by a local doctor and was put on anti-tuberculous therapy (ATT) in 2006 based on X-ray chest finding of opaque shadow in left lower zone. He took ATT for 8 months during which his symptoms improved only slightly. Two weeks after discontinuing treatment he again developed fever and haemoptysis, that gradually aggravated and he received symptomatic treatment from various local doctors. Patient was then referred to our setup where a detailed work up was done to find the cause for patients' symptoms. Based on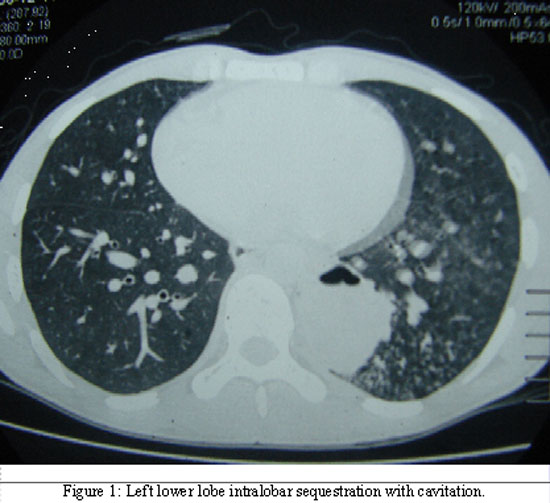
chest X-ray and computed tomographic scan (CT) of chest, pulmonary sequestration was suspected. A CT angiography was done in addition to sputum gram staining, culture and sensitivity which were all negative. CT scan showed left costovertebral area of consolidation with cavitations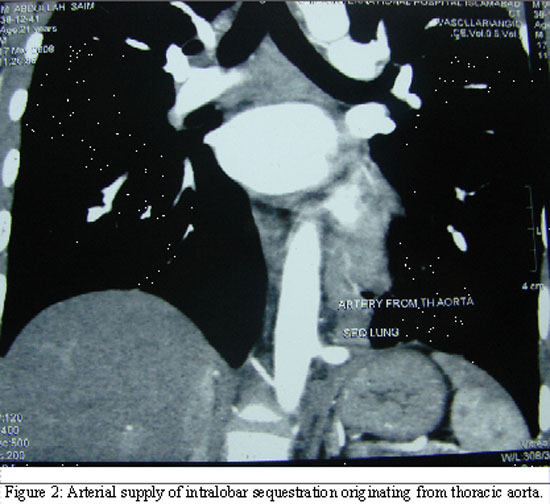
(Figure-1). No evidence of mediastinal lymphadenopathy and pleural effusion was seen. CT Pulmonary Angiography confirmed the diagnosis of Left lower lobe intralobar sequestration with adjacent pulmonary inflammation and demonstrated arterial branch arising from lower thoracic aorta (Figure-2). The diameter of this branch was approximately 6 mm with branches inside the sequestrated segment. There was demonstration of draining pulmonary veins from the sequestrated segment. However no bronchial communication was noted. Patient then underwent Left sided thoracotomy and left lower lobectomy. During surgery arterial supply to the lobe from descending aorta just above the diaphragm was observed with poor fissure between upper and lower lobe. Sequestrated lower lobe artery was ligated from descending aorta along with ligation of Inferior pulmonary vein. Branches of pulmonary artery to lower lobe were also ligated and oversewn. Recovery was uneventful.
Discussion
Pulmonary sequestration is an infrequent congenital pulmonary disorder defined by non-functional and dysplastic pulmonary tissue lacking a normal connection with the tracheobronchial tree and the pulmonary arteries.4 Savic et al reported that more than 50% of patients become symptomatic after the second decade of life, and in 15% of patients' anomaly caused no symptoms.4 The diagnosis of sequestration relies on imaging techniques, mainly helical CT angiography,5 that can identify each of the components of the sequestration pattern: sequestered or dysplastic lung mass, aberrant arterial supply, and anomalous venous drainage. Intralobar sequestration (75% of cases) occurs in the normal lung parenchyma and does not have a separate pleural lining.6 The arterial supply usually originates from the aorta or its branches, and the venous return is usually (95% of cases) into the pulmonary veins.4 Intralobar sequestrations are usually found within the lower lobes.6 It was reported that 97.75% of 400 intralobar sequestrations were in such locations.4 Only eight cases (2%) in this series were found in the upper lobes, mainly in the right side.4 In juvenile patients, the arterial supply originates from the descending thoracic aorta predominantly, and it occurs in the left lung, most commonly in the basal segment of the lower lobe.6 The main treatment for pulmonary sequestration should be surgical resection with ligation of aberrant artery which may cause recurrent pulmonary infection and unfavourable cardiac influence due to the existing aortopulmonary shunt.7
The clinical manifestations of intralobar sequestration are chronic cough, sputum and recurrent attacks of pneumonia. Our patient was treated for pneumonias, and eventually with anti-tuberculous therapy due to persistent infiltrate and haemoptysis, which is not surprising for such a rare disorder in a tuberculosis prevalent region, like ours.
Therefore, we recommend that an unresolving medially situated lung infiltrate in lower lobes should be suspected for possible sequestration and timely referral for definitive treatment should be sorted. To our knowledge this is a first case reported in Pakistan and neighbouring countries and advocates clinical importance of this rare disorder which with timely diagnosis can be prevented from complications and can be treated effectively.
References
1.Masuko H, Satoh H, Miyazaki K, Kikuchi N, Kondo Y, Ohtsuka M, et al. Pulmonary sequestration with elevated serum level of progastrin-releasing peptide. Intern Med 2008; 47: 157-60.
2.Pryce DM, Sellors JH, Blair LG. Intralobular sequestration of the lung associated with an abnormal pulmonary artery. Br J Surg 1947; 35: 18-29.
3.Tsunezuka Y, Sato H. Intralobar pulmonary sequestration with three aberrant arteries in a 75-year-old patient. Chest 1998; 114: 936-8.
4.Savic B, Birtel FJ, Tholen W, Funke HD, Knoche R. Lung sequestration: report of seven cases and review of 540 published cases. Thorax 1979; 34: 96-101.
5.Lee EY, Siegel MJ, Sierra LM, Foglia RP. Evaluation of angioarchitecture of pulmonary sequestration in pediatric patients using 3D MDCT angiography. AJR Am J Roentgenol 2004; 183: 183-8.
6.Ferretti GR, Jouvan FB, Coulomb M.MDCT demonstration of intralobar pulmonary sequestration of the right upper lobe in an adult. AJR Am J Roentgenol 2005; 185: 1663-4.
7.Sato H, Watanabe A, Yamaguchi T, Harada N, Yamauchi A, Inoue S, et al. Pulmonary sequestration associated with asymptomatic aspergillosis. Ann Thorac Cardiovasc Surg 2005; 11: 41-3.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: