
Amit Agrawal ( Department of Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal. )
Akshay Pratap ( Department of Surgery, B.P. Koirala Institute of Health Sciences, Dharan, Nepal. )
Awadhesh Tiwari ( Department of Radiology, B.P. Koirala Institute of Health Sciences, Dharan, Nepal. )
November 2009, Volume 59, Issue 11
Case Reports
Abstract
Intracranial complications of otitis media are associated with high mortality. Persistent otalgia or otorrhea while on oral antibiotics with associated neurological symptoms are ominous signs suggestive of a complication. A high index of suspicion and early diagnosis with radio-imaging are essential for better outcome in these patients. We report a neglected case of chronic otitis media and discuss the magnetic resonance imaging findings.
Introduction
In spite of significant decrease after antibiotic advent, intracranial complications of otitis media still represent a jeopardizing situation associated with high mortality.1,2 A high index of suspicion and early diagnosis are essential for better outcome in these patients.2,3 Extension of the infectious process beyond the mastoid system can lead to a variety of intracranial and extracranial complications, including meningitis; epidural, subdural and intraparenchymal abscesses; vascular thrombosis; osteomyelitis and abscesses deep within the neck. A neglected case of chronic otitis media is presented and the magnetic resonance imaging (MRI) findings are discussed.
Discussion
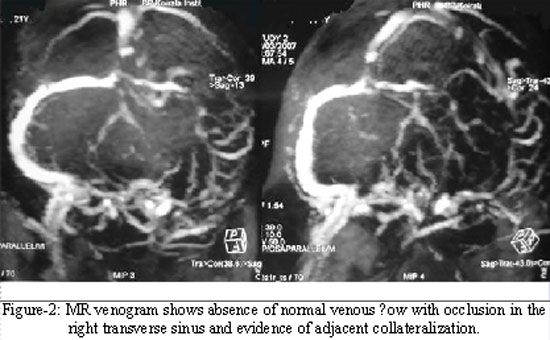
A variety of intra and extracranial complications can occur due to extension of the infectious process beyond the mastoid system.1,3 The most common early symptoms are increased otorrhea, fever, and headache, with later altered mental status, cranial nerve palsies, and nuchal rigidity.4,5 MRI is superior in depicting intracranial complications like subdural and epidural empyema and vasculitic complications notably on (FLAIR fluid-attenuated inversion recovery)-weighted images.6 MRI helps to visualize meningeal enhancement more clearly (Figure-1).6 Epidural abscess is the most common intracranial complication arising from middle ear infection. It results from spread by contiguity following bone destruction in coalescent mastoiditis.7 Although it can occur in the middle cranial fossa, the posterior fossa location is far more common due to osseous destruction in the Trautmann triangle over the sigmoid sinus plate or in the posterior cortex of the petrous pyramid.8,9 Subdural empyema secondary to otitis media usually develops in the interhemispheric fissure and along the tentorium cerebelli and appears at imaging as widening of the extracerebral space with compression of the adjacent sulci.3 It is mildly hyperintense relative to cerebrospinal fluid (CSF) and hypointense to white matter on T1WI. It appears hyperintense relative to CSF and white matter on T2WI allowing distinction from sterile effusions and most chronic haematomas.6,8 Loculation within the collection is not uncommon (Figure-1). As surrounding vasogenic oedema does not occur in association with empyema, the presence of abnormal attenuation or signal intensity in the adjacent parenchyma is usually the result of associated cerebritis.3 In contrast to epidural abscess, subdural empyema never manifests as a clinically silent complication. Affected patients usually have meningismus, focal neurologic findings, or focal seizures and always a very serious complication that requires prompt neurosurgical drainage.9 The epidural abscess may lead to sigmoid sinus thrombosis as a protective mechanism in an attempt to localize the infection.2,3 Indirect imaging signs of dural venous thrombosis include low attenuation of the sinus on un-enhanced and contrast-enhanced CT scans, absence of normal flow void on spin-echo MR images and absence of flow-related enhancement on gradient-echo MR images.3 Direct evidence of dural sinus thrombosis consists of identification of a thrombus within the sinus, particularly in the deoxyhaemoglobin stage. MR venography with reversal of the saturation pulse of MR angiography is very useful for definitive diagnosis (Figure-2).9 The severity of these complications underlines the importance of clinical awareness and early imaging diagnosis to establish suitable treatment.1 For early management, it is necessary to maintain a high index of suspicion and identification of non-typical cases which are likely to be masqueraded by antibiotic use.1 Persistent otalgia or otorrhea while on oral antibiotics with associated neurological symptoms are ominous signs suggestive of a complication.10 Therefore, CT should be performed as early as possible in all patients with suspected mastoiditis, followed by cranial MR imaging if an intracranial complication is suspected.3
Case Report
A 21-years old female patient presented with intermittent right ear pain and discharge of 8 years duration. Presently, the ear discharge was persistent for last two months, with no response to medication. She developed headache with multiple episodes of vomiting during last 24 hours and gradually lapsed into altered sensorium. On examination, she had neck rigidity. She was responding to deep pain and was moving all four limbs. Rest of the examination was unremarkable. Blood investigations were normal. A previous pus culture from ear discharge showed Pseudomonas aeroginosa resistant to all antibiotics except Ceftriaxone and Amikacin. She underwent MRI of brain and it showed mastoiditis, extradural abscess, subdural empyema, cerebritis and transverse sinus thrombosis (Figures 1-2). She was started on Inj. Cefriaxone, Gentamicin and Metronidazole, anti-epileptics and anti-oedema measures. While she was awaiting for emergency surgery, she deteriorated in her neurological status and succumbed to it.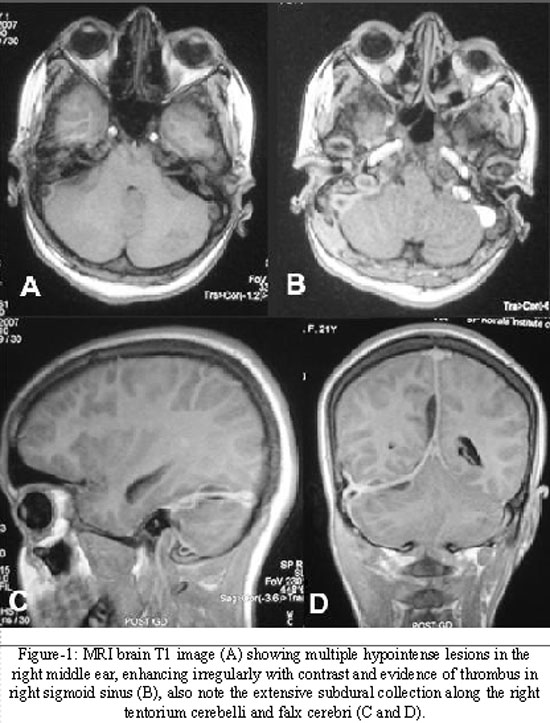
References
1.Miura MS, Krumennauer RC, Lubianca Neto JF. Intracranial complications of chronic suppurative otitis media in children. Rev Bras Otorrinolaringol 2005; 71: 639-43.
2.Gower DJ, McGuirt WF, Kelly DL Jr. Intracranial complications of ear disease in a pediatric population with special emphasis on subdural effusion and empyema. South Med J 1985; 78: 429-34.
3.Vazquez E, Castellote A, Piqueras J, Mauleon S, Creixell S, Pumarola F, et al. Imaging of Complications of Acute Mastoiditis in Children. RadioGraphics 2003; 23: 359-72.
4.Kolenda J, Carr MM, Lemckert RJ, Ummat SK. Intracranial sinus thrombosis secondary to ear disease in an adolescent. J Otolaryngol 1997; 26:203-6.
5.Kuczkowski J, Mikaszewski B. Intracranial complications of acute and chronic mastoiditis: report of two cases in children. Int J Pediatr Otorhinolaryngol 2001; 60: 227-37.
6.Kastrup O, Wanke I, Maschke M. Neuroimaging of Infections. NeuroRx 2005; 2: 324-32.
7.Harley EH, Sdralis T, Berkowitz RG. Acute mastoiditis in children: a 12-year retrospective study. Otolaryngol Head Neck Surg 1997; 116: 26-30.
8.Mafee MF, Singleton EL, Valvassori GE, Espinosa GA, Kumar A, Aimi K. Acute otomastoiditis and its complications: role of CT. Radiology 1985; 155:391-7.
9.Dobben GD, Rao? B, Mafee MF, Kamel A, Mercurio S. Otogenic intracranial in?ammations: role of magnetic resonance imaging. Top Magn Reson Imaging 2000; 11: 76-86.
10.Veillon F, Riehm S, Roedlich MN, Meriot P, Blonde E, Tongio J. Imaging of middle ear pathology. Semin Roentgenol 2000; 35:2-11.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: