
Sher Mohammad Khan Paindakhel ( Division of Nuclear Medicine, IRNUM, Peshawar University Campus, Peshawar. )
Mir Badshah ( Division of Nuclear Medicine, IRNUM, Peshawar University Campus, Peshawar. )
April 1980, Volume 30, Issue 4
Original Article
Abstract
The frequency of pyramidal lobe varies from 43% to 80% in operated or cadaver specimens, but on radioisotopic scanning, it was not found to be high. Four hundred and forty six patients who had scanning (imaging) of the thyroid were analysed. The percentage of pyramidal lobe was 4.2. (JPMA 30:87, 1980).
Introduction
Normally the thyroglossal duct undergoes dissolution and fragmentation about the second month after conception. It is represented at its origin by the foramen caecum and at its distal end, the remnant differentiates to thyroid tissue forming the pyramidal lobe. The incidence of the pyramidal lobe varies from 43 percent to 80 percent in operated or cadaver specimens (Hollinshead, 1954; Means et al., 1963) but in the experience of workers performing thyroid scans it has not been very high (Atkins and Richards, 1968). The object of the present study was to find the frequency of pyramidal lobe in routine scanning (imaging) of the thyroid gland in Peshawar.
Patients and Methods
The thyroid scans of 464 patients (141 males and 305 females) were studied. The ages ranged from 6 to 80 years. All patients were clinically examined before the thyroid imaging and the images were corelated with the clinical findings. Eighteen Scans were excluded because of technical reasons.
Iodine-131 was given orally and images were obtained after 24 hours using Toshiba Gamma Camera.
Results
Nineteen pyramidal lobes were seen on imaging. A pyramidal lobe was considered if finger like radioactivity extended proximally in or near the midline from the isthmus or either of the lobes as shown in the accompanying figures.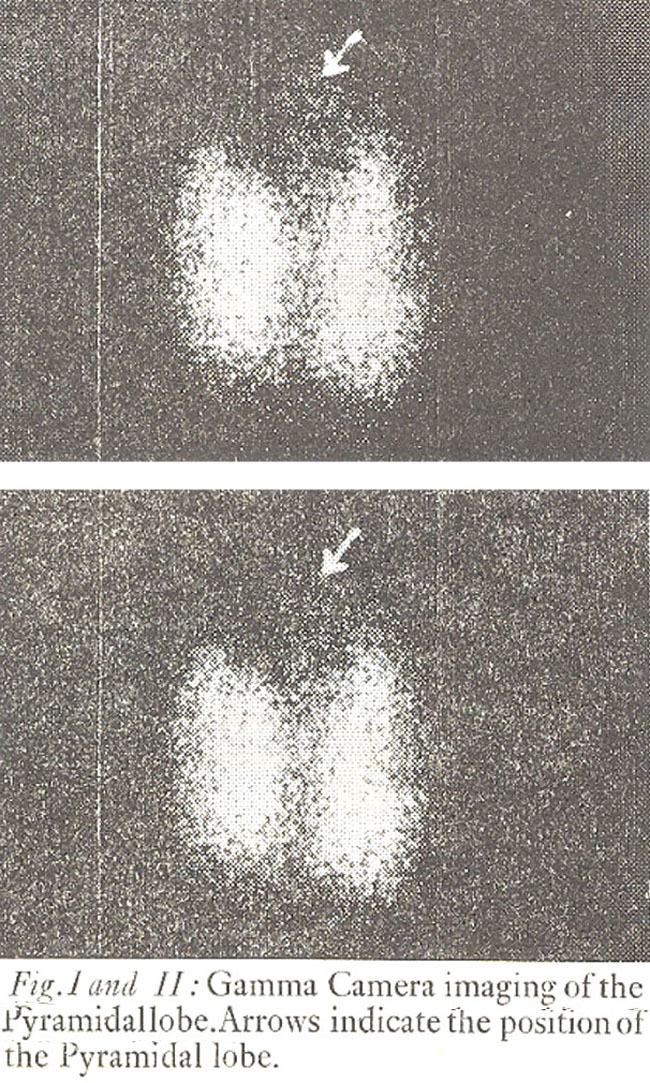
Discussion
The pyramidal lobe may present as a midline neck swelling. It may enlarge after thyroid surgery because of hypertrophy and or hyperplasia to supply the body needs. This is apparently the reason for its frequent appearance in postoperative patients. The lobe enlarges because of the action of thyroid stimulating hormone. On imaging, the radioactivity is anterior to the main radioactivity of the thyroid gland in the lateral and oblique views. Knowledge of pyramidal lobe is also important if total thyroidectomy is contemplated by a surgeon in patients with cancer of the thyroid.
In the present series the frequency (4.2%) is less than that reported by Atkins and Richards (1968) and Izenstark et al (1969), but slightly more than Beierwaltes et al (1957). The low frequency is probably not due to racial characteristics but may be due to the physical characteristics of the imaging agent, iodine-131, which is not ideal for gamma camera (Khan Paindakhel and Ahmad, 1979).
Acknowledgements
We are grateful to the clinicians for referring patients and to Miss Tabassum Latif for secretarial help.
References
1. Atkins, H.L. and Richards, P. (1968) Assessment of thyroid function and anatomy with technetium-99m as pertech netate. J. Nuc. Med., 9:7.
2. Beierwaltes, W.H., Johnson, P.C. and Solari, A.J. (1957) Clinical use of Radioisotopes. Philadelphia, Saunders, 1957, p. 59.
3. Hollinshead, W.H. Anatomy for surgeons Vol. 1. New York, Hoeber-Harper, 1954, p. 519.
4. Izenstark, J.L., Forsaith, A.L. and Horwitz, N.H. (1969) The Pyramidal lobe in thyroid imaging. J. Nucl. Med., 10:519.
5. Khan Paindakhel, S.M., Ahmad, I. (1979) Rapid Evaluation of Thyroid Function and Structure in and Around Khyber Pass. JPMA., 29:168.
6. Means, J.H., Degroot, L.J. and Stanbury, J.B. The Thyroid and its diseases. 3rd ed. New York, McGraw-Hill, 1963, p. 7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: