
Aziza Fayyaz ( PMRC Research Centre, Lahore. )
Zulfiqar Haider ( PMRC Research Centre, Lahore. )
Fayyaz-ud-Din ( PMRC Research Centre, Lahore. )
Kishwar Z. Moeen ( Dept. of Pathology, Fatima Jinnah Medical College and Radioisotope Centre, Lahore. )
Maqbool Shahid ( Mayo Hospital, Lahore. )
April 1980, Volume 30, Issue 4
Original Article
Abstract
One hundred and one patients (51 females and 50 males), presenting with unexplained hepatomegaly were investigated. The histological findings on liver biopsy included normal architecture (36), changes of viral hepatitis (5), round cell infiltration in portal tract (10), fatty changes (14), hepatic malignancy (8), biliary disease (3), infections of the liver (12), cirrhosis of liver (6) and a miscellaneous group comprising of 8 cases.
A past history of jaundice was a frequent feature in those showing changes of viral hepatitis, cirrhosis and chronic inflammatory changes. Similarly significant elevation of transaminases was most frequently encountered in patients with histological features of viral hepatitis. Gross elevation of alkaline phosphatase was present in those with hepatic malignancy and biliary disease. Liver scan was helpful in 15 cases showing focal involvement such as malignancy and early abscess formation. Obscure liver enlargements form a heterogenous group and further work is needed in patients showing normal architecture and minimal histological changes (JPMA 30:84, 1980).
Introduction
There are number of patients who present with unexplained mild to moderate enlargement of liver, sometimes associated with vague and recurrent abdominal symptoms. Most of these cases are treated empirically with anti-amoebic drugs with variable results.
Earlier, we reported the results of serological test for amoebiasis in 50 such patients which showed that nearly two third were negative on serological testing (Haider and Fayyaz, 1978). In the present study we report the results of investigation in 101 patients who presented with unexplained hepatic enlargement.
Material and Methods
The study comprises of 101 cases (51 females and 50 males) admitted in the Medical Wards of various hospitals in Lahore. All patients had hepatomegaly without a clinically obvious cause. In addition a large number of patients had associated chronic abdominal symptoms such as intermittent diarrhoea, dyspepsia, vaguely localised abdominal pain, flatulence and discomfort in the right hypochondrium. Low grade temperature was also complained of by a few patients. Hepatomegaly was diagnosed on clinical examination and was defined as enlargement of liver above the 6th intercostal space in midclavicular line on percussion and below the right costal margin while patient is examined in supine position when there was no evidence of emphysema or visceroptosis.
Liver enlargement was always confirmed by a liver scan. Routine investigations included Haemoglobin total and differential leucolyte count, stool examination and urine analysis. The liver function profile which included serum bilirubin, transaminases, alkaline phosphatase, serum protein, albumin, globulin and thymol turbidity was, done in all.
Results of SGOT and SGPT were expressed as Karman units (normal values SGOT 8-40, SGPT 5-35 units) and alkaline phosphatase as K.A. units (normal 3-13 units). Serum protein and bilirubin were done by the methods described by King and Wooten (1964). An albumin: globulin ratio of less than 1 was considered abnormal. Liver biopsy was done in all cases using Menghini\'s aspiration needle. The histological findings in liver biopsy were interpreted by one of the authors (K.Z.M.) according to the general criteria described by Scheuer (1973). The typing of cirrhosis was done according to the criteria adopted by the Panel of Pathologists (PMRC, 1973).
Results
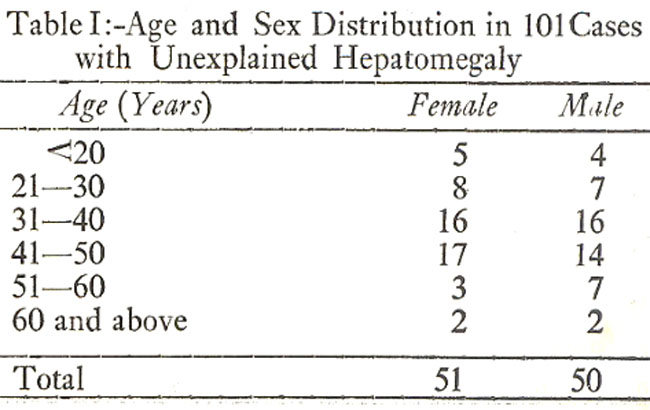
Table I shows age and sex distribution. The majority of the patients were between the ages of 31-60 years.
The histological findings in 101 cases are shown in Table II.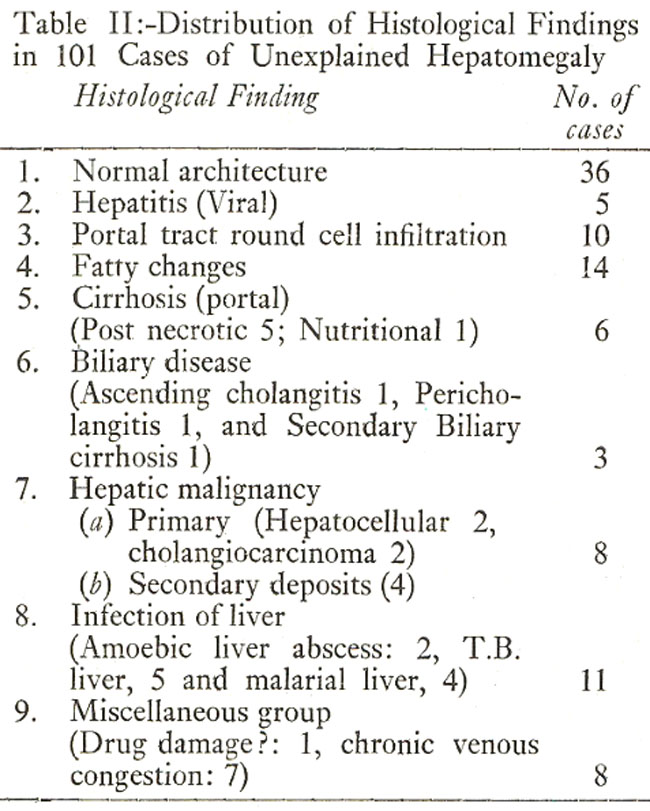
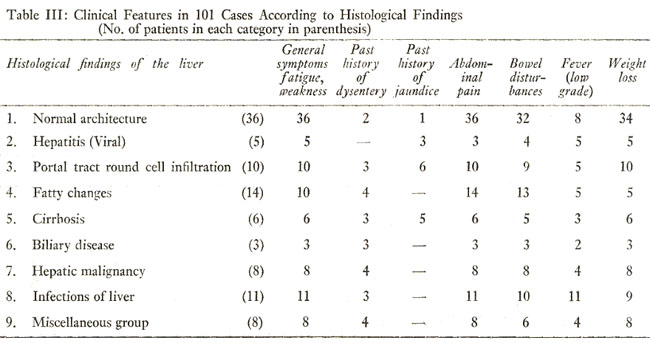
Table III shows signs and symptoms in relation to histological findings. General symptoms like malaise, lethargy, indigestion, anorexia as well as weight loss were present in a large number of cases in various histological groups. Also, periodic fever was one of the common complaints. Past history of jaundice was present in only one out of 36 with normal histology but in 3 of the 5 patients with changes of viral hepatitis, 6 of the 10 cases with non-specific portal tract round cell infiltration and 5 of the 6 cases with cirrhosis of liver. A past history of dysentery was present in a few patients in each group except in those with changes suggestive of viral hepatitis.
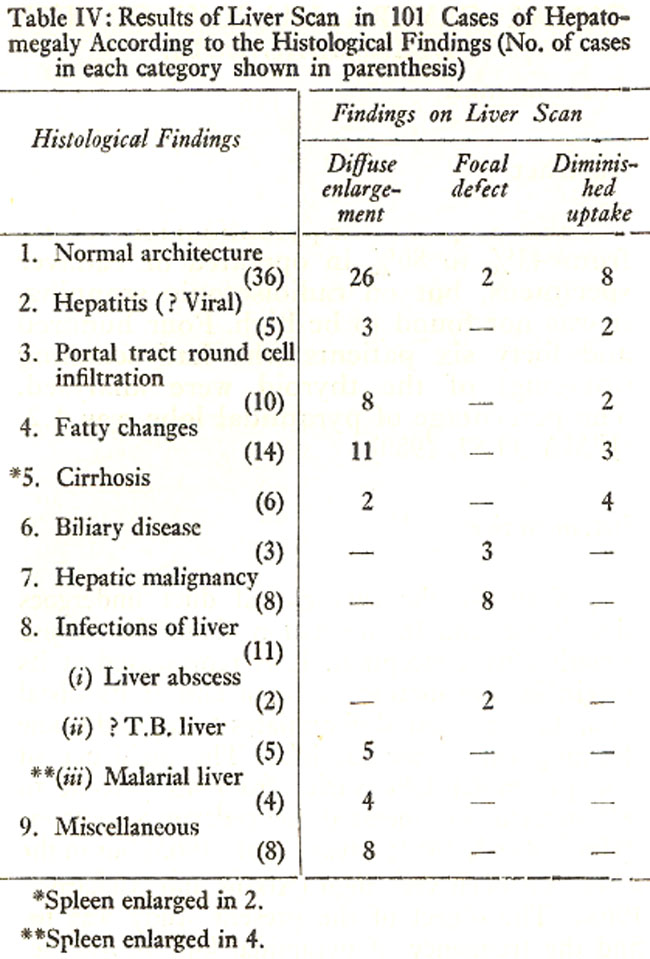
Table IV shows results of liver scan in patients with liver enlargement. The liver enlargement was associated with a cold area in 15 and poor uptake of isotope in 19 patients.
Histological findings in the 15 patients with cold areas on liver scan included normal histology (2), biliary disease (3), malignant liver (8) and early amoebic liver abscess (2). The 2 patients with normal histology and a cold are later developed hepatic malignancy. There were 19 patients who showed diminished uptake associated with liver enlargement. Histological findings were normal architecture (8), viral hepatitis (2), portal tract round cell infiltration (2), fatty changes (3) and cirrhosis of liver (4).
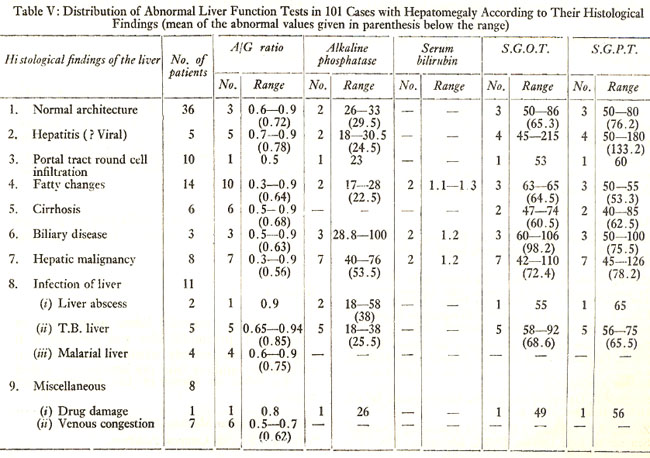
Table V shows liver function profile as related to histological findings. Only 3 out of 36 with normal histological findings showed abnormal liver function tests of whom two developed malignancy on follow up. Four out of 5 patients with changes of viral hepatitis showed elevation of SGOT and SGPT with a value of 146.5 and 133.2 units respectively. Of the 10 patients with non-specific round cell infiltration in portal tract, only one showed mild changes in liver function tests.
Patients with biliary disease and malignant involvement of the liver were characterised by high level of alkaline phosphatase and mild to moderate elevation in transaminases. The two cases of amoebic liver abscess also showed elevated levels of alkaline phosphatase with mild elevation of transaminases in one.
Discussion
This study has shown that patients presenting with chronic unexplained liver enlargements associated with chronic symptoms are a heterogenous group. It is evident that approximately 50% of the patients showed minimal changes which included either normal histology or fatty changes. Most of the patients had vague general symptoms and abdominal disturbances. However, two patients with initial normal histology subsequently died of malignancy involving the liver. Two patients whose initial histology showed marked fatty degeneration developed diabetes mellitus 2 years after a normal glucose tolerance test at the time of liver biopsy. It is possible that fatty changes in the liver in these two cases could represent a prediabetic phase, but the presence of obesity in these cases precludes a definite conclusion. Patients with hepatomegaly who show normal histology are a group which need further investigation and follow up for any possible evidence of progressive liver damage.
Ten patients showed round cell infiltration with nearly normal liver function tests. Seven out of these 10 cases had positive E. histolytica in their stools but serological test for amoebiasis was positive in only 3. On the other hand past history of jaundice was present in 6 out of 10 patients. These cases could represent either residual changes of past viral hepatitis or nonspecific portal tract reaction to intestinal infec- tion. In these cases the likelihood of past hepatitis is more plausible and is supported by the experience of other workers in Pakistan (Ahmad and Qureshi, 1975). Five cases showing changes of viral hepatitis were characterised by past history of jaundice and significant disturbances in liver function test in 3 patients. Such cases may represent resolving acute viral hepatitis or the possibility that they may develop chronic active hepatitis.
The important role of viral hepatitis in the aetiology of cirrhosis in this country was suggested by a history of jaundice in 5 out of 6 patients, with the histological findings of postnecrotic cirrhosis. This supports the conclusion drawn by workers in Karachi who found postnecrotic cirrhosis to be the most common variety compared to any other type of portal cirrhosis (Zuberi and Rab, 1979).
Primary tuberculosis of the liver is exceedingly rare and it is usually due to haemotogenous spread of the tubercle bacillus from a focus of infection elsewhere (Sherlock, 1963). Five cases in which T.B. granuloma was diagnosed on liver histology, there was no apparent extra-hepatic tuberculous focus and radiology of chest was negative in all. It is possible that in view of the chronic abdominal symptoms intestinal tuberculosis may have been contributory.
The two cases of amoebic liver infection showed early abscess formation with strongly positive serological test for amoebiasis and showed good response to anti-amoebic drugs.
No case of so called "chronic nonsuppurative amoebic hepatitis" was found in this series of patients.
Acknowledgements
We wish to express our thanks to physicians of Mayo, Ganga Ram, Lahore General and Combined Military Hospitals, Lahore for referring the patients for this study. We also express our appreciation for Mr. Khalid Maqbool and Miss Mussarat Jabeen for technical assistance.
References
1. Ahmad, M. and Qureshi, S.M. (1975) Anicteric hepatitis in Pakistan. Incidence in apparently healthy males. JPMA., 25:108.
2. Haider, Z. and Fayyaz, A. (1978) Latex agglutination test for amoebiasis in Pakistani patients with chronic \'obscure\' liver enlargements. J. Trop. Med. Hyg., 81:13.
3. King, E.J. and Wootton, I.D.P. Microanalysis in medical biochemistry. 3rd ed. London, Churchill, 1956.
4. Report of the Panel of Pathologists on Liver Disease (1973). Pakistan Medical Research Council (unpublished).
5. Scheuer, P.J. Liver biopsy interpretation. 2nd ed. London, Bailiere Tindall 1973.
6. Sherlock, S. Diseases of the liver and biliary system. 3rd ed. Oxford, Blackwell, 1963, p. 533.
7. Zuberi, S.J. and Rab, S.M. (1979) Proceedings National Seminar on Liver Disease. PMRC. Monograph No. 2:82.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: