
M.H.A. Beg ( Department of Otolaryngology, K.V. Social Security SITE Hospital, Karachi. )
Amina Rehman ( Department of Otolaryngology, K.V. Social Security SITE Hospital, Karachi. )
S. Malik ( Department of Otolaryngology, K.V. Social Security SITE Hospital, Karachi. )
A. Qayum ( Department of Otolaryngology, K.V. Social Security SITE Hospital, Karachi. )
May 1983, Volume 33, Issue 5
Original Article
Abstract
One hundred and sixty three malignant lesions in the region of the pharynx, oesophagus and oral cavity, in secured workers and thus families, seen over a period of six years (1976 to 1981) have been analysed. The valecula and pyriform fossa were the most common sites in the pharynx and the cheek mucosa in the oral cavity. The incidence was 10 cases in 100,000 secured workers per year. Males between the ages of 41 and 50 years and mostly emigrants from India with specific chewing habits were usually affected. Histopathology revealed 84% of the tumours to be squamous cell carcinoma and TNM staging classified most to be in the advanced stage. No evidence was found to label sub-mucous fibrosis as a premalignant condition (JPMA 33 : 110,1983).
Introduction
Cancer of the pharynx and oral cavity is frequently encountered in the Indo-Pakistan subcontinent. The reports available from these regions are all from cancer centres which exclusively manage such cases (Karim, 1971; Jussawalla, 1973; Zaidi et aL, 1974) and cater to patients from all over the country and abroad. A true incidence can therefore not be had from these statistics as they reflect higher figures.
This study reveals the cases of cancer in. otolaryngology in ENT practice in a general hospital seen over a period of six years. Harrison (1972) has expressed views that a personal series constitutes more valuable and practical information.
Material and Methods
The patients were selected from the population of secured workers attending the KV Social Security SITE Hospital. It has 326 beds and is run by the Sind Employees Social Security Scheme. The ENT Unit of the hospital has 20 beds and it deals with all general E.N.T. problems. All patients were seen in the out patients department. Their symptoms, age, sex and ethnic origin was recorded. A complete otolaryngological examination was conducted and lesions suspected to be malignant were staged according to TNM classification (UICC, 1973). When found necessary, an examination under anaesthesia was carried out and in a few cases the staging had to be altered. All cases were subjected to a biopsy followed by histopathology and coding was done according to the method suggested by ICD-O International classification of Disease for Oncology (WHO, 1976).
In 13 cases the biopsy had to be repeated. as the result was inconclusive due to secondary infection and sloughing.
Results
One hundred and sixty three cases of malignancy located in the oral cavity, pharynx and oesophagus were diagnosed in a period of six years from 1976-1981 (Table I).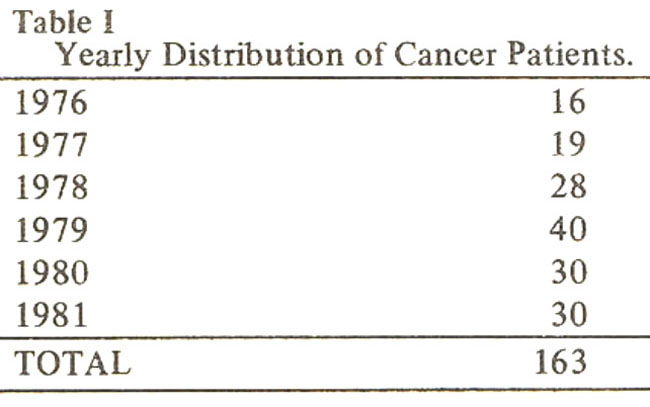
Sixty five patients belonged to the age group between 41 and 50 years and 54 were below 40 years (Table II).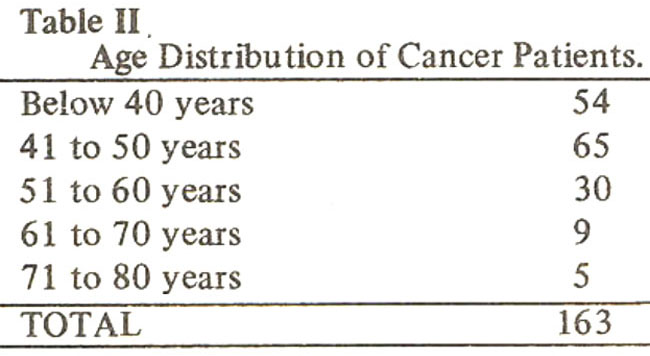
Males were affected mOre than females in a ratio of 4 1 (Table III).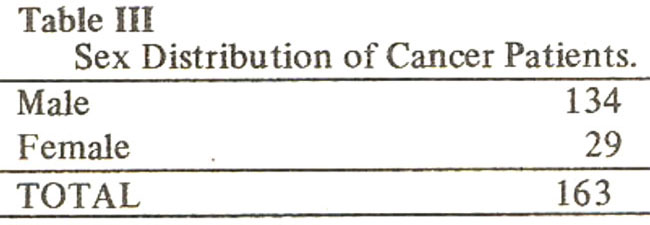
The most common site of the lesion was the pharynx (Fig.1),
followed by the oesophagus and the cheek (Table IV).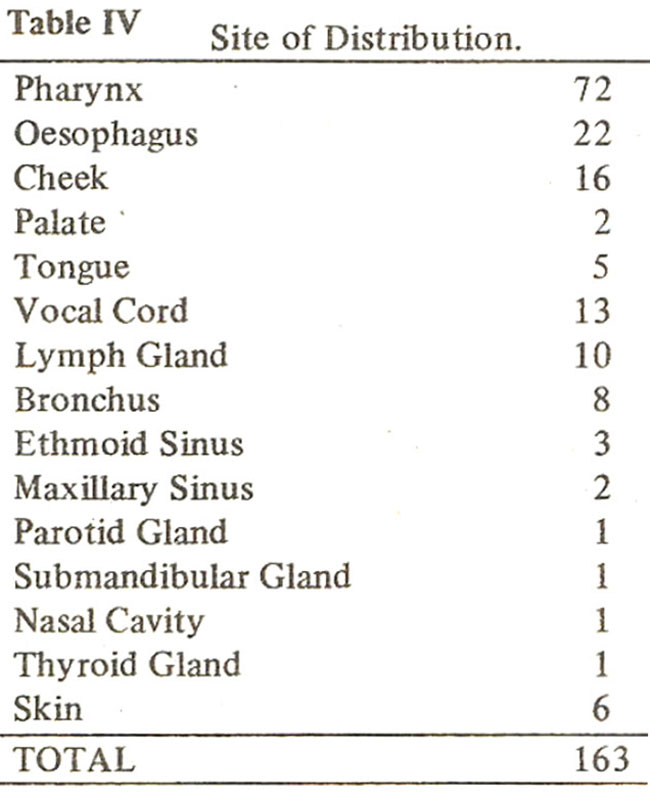
The distribution of the pharyngeal cancer(44%) showed 22 originating in the valecula, 21 in the pyriform fossa, 11 in the tonsils, 2 in the postcricoid and one in the nasopharynx. In 15 cases the lesions were so extensive, that it was difficult to localise the site of origin (Table V).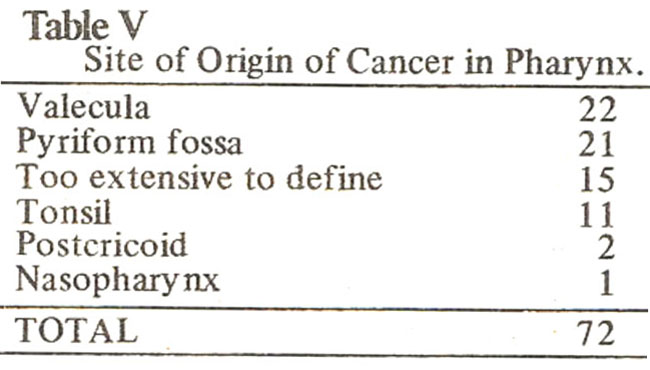
Oesophagus was the second commonest site for cancer. Of 22 cases (13.4%), 12 had lesion in the middle third, 4 in the upper third and 6 in the lower third of the oesophagus. Glottic cancer was found in 13 patients (8%) which is a smaller number when compared to the West (Harrison, 1973). Three patients had lesions in the Ethmoid sinus and 2 in the Maxillary Sinus (Fig.2).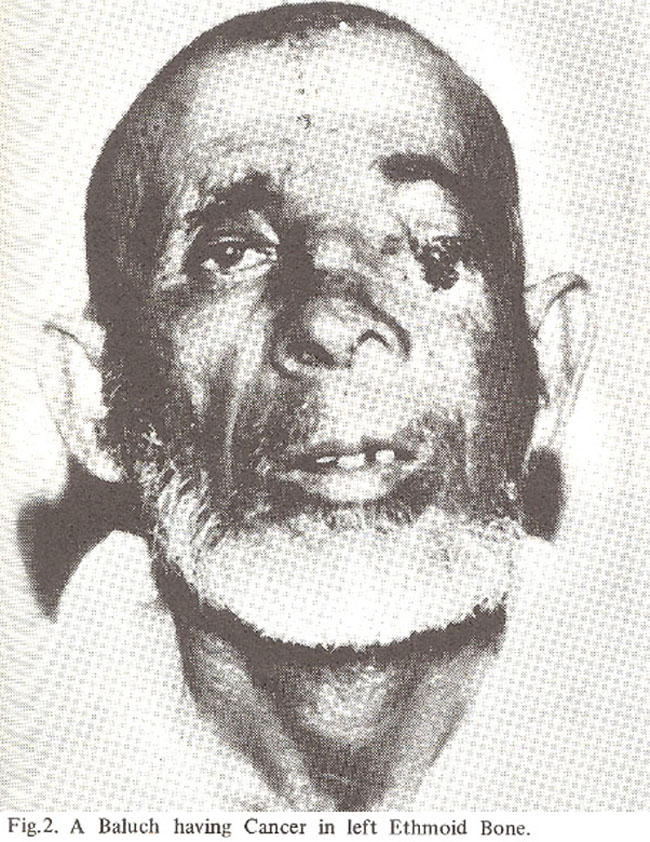
Sixteen cases had cancer of the cheek (Fig.3).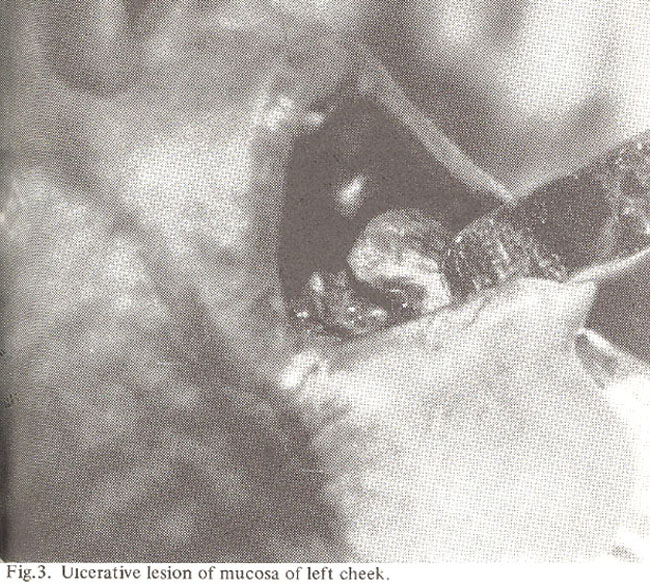
Histological examination showed squamous cell carcinoma in 139 cases (8 5%). Six cases were anaplastic and five revealed basal cell carcinoma.Details of the histology reports are shown in Table VI.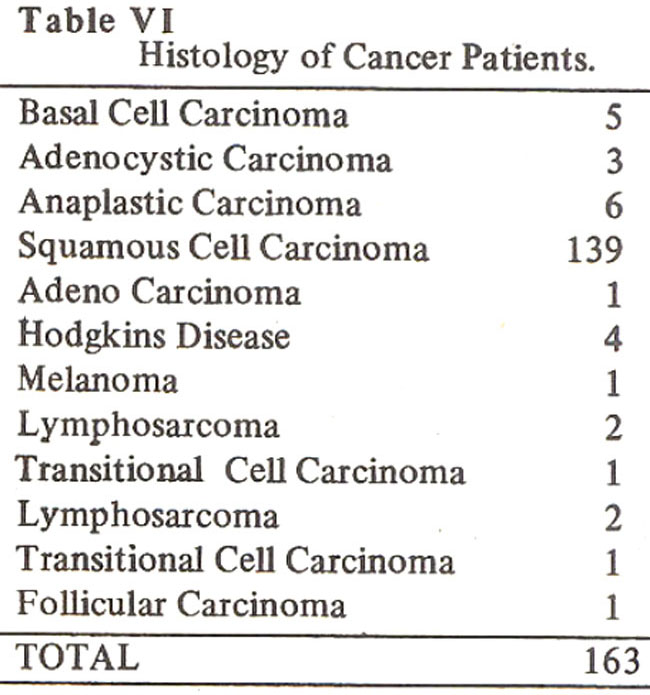
TNM staging revealed 74 cases in T3 stage and 55 in the T2 stage. No case was seen in the Ti stage or carcinoma in situ (Table VII).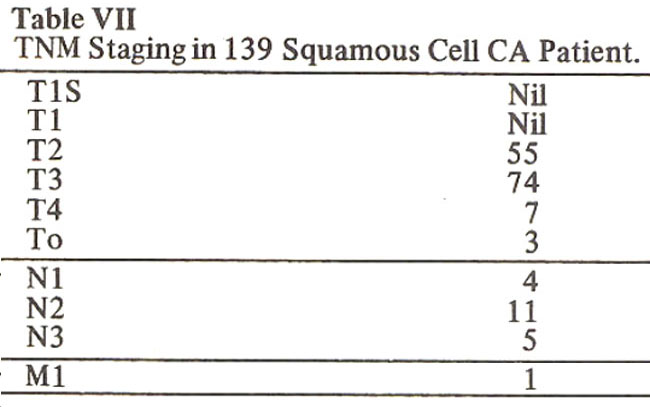
A specific racial pattern was observed in the series. 128 cases were emigrants from India, having prevalent chewing habits of betel and tobacco (58), and this was combined with cigarette smoking in 32 individuals (Table VIII).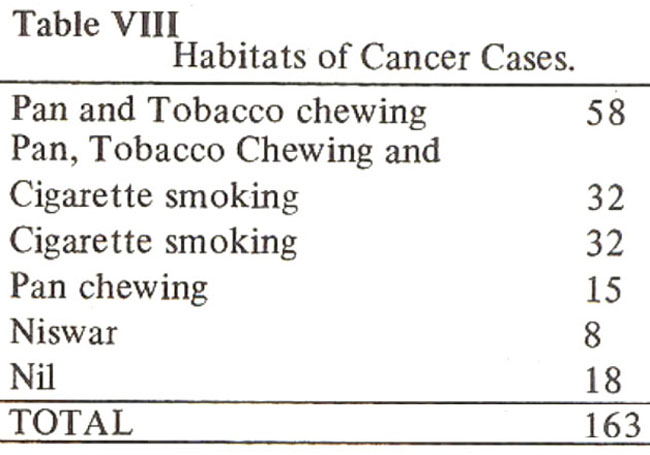
Discussion
Pindborg (1980) has described the incidence of cancer as “the number of new cases of disease in a defined population usually 100,000 in a given period of time, usually one year.” As there is no cancer registry in Pakistan, it is difficult to calculate a definite incidence. Frequency of malignant tumours (Jafarey and Zaidi, 1976) and specially oral lesions (Jafrey et al., 1972) have been reported as the number of cases present at a certain time, which is actually not a correct picture.
Figures from India are available from large cancer centres (Jussawalla, 1973; Hirayama, 1966) which also do not depict a true incidence. The patients attending these centres are from all over the country and also from abroad.
In the present series the incidence is obtained from the secured workers population attending the K,V. Social Security SITE Hospital, which is approximately 381, 444. The statistics of the cancer cases in the field of Otolaryngology thus amounts to one in 9536 individuals and being a total of forty per year.
The relationship between oral cancer and chewing of pan and tobacco has been reported earlier (Jafarey and Zaidi, 1976; Hirayama, 1966; Paymaster et al., 1968). The cheek mucosa,tongue (Fig.4),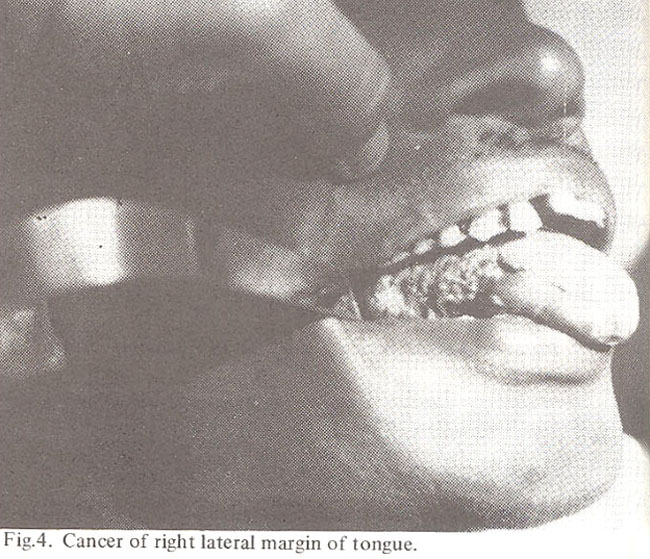
valeeula and the pyriform fossa are the usual sites, as they directly come in contact with tobacco. Paymaster (1957) reported that 70% of Oropharangeal cancers originated in the pyriform fossa. In this series pyriform fossa and valecula were involved in an equal number of cases.
The frequency of chewing and the duration of keeping the quid also contributes to the risk (Hirayama, 1966). The use of large amount of chillies in food is an additive risk factor specially for lesions in lateral pharyngeal gutter of the tongue, valecula and the pyriform fossa. Immigrants from north and west of India who settled in Karachi in 1947 after the partition of the subcontinent, have specific chewing habits and take spicy foods. In this series 78.5% belonged to this emigrant group. The pattern of the disease is very similar to that studied in Bombay (Paymaster, 1957). The only difference noted was in the smoking habits. Bidi is smoked in a smaller quantity in Karachi (Mehmood et at., 1974) as compared to Bombay.
Naswar (Snuff) kept under the tongue has been labelled as an attributable factor for causing cancer of the floor of the mouth. This is a common habit in the north and west of Pakistan. In the present series, the number of pathans using naswar was too small to determine the relationship between the two. There were 19 pathans (11.6%) and 8 Baluchis (4.9%). Another study by Sobin (1969) also shows a low frequency of oral cancer in Afghanistan where the chewing of tobacco and lime is also customary. Other workers have reported a frequency of skin cancer in the North of Pakistan (Zaidi et al., 1977), Afghanistan (Sobin, 1969) and Iran (Habibi. 1965).
Submucosal fibrosis is said to be a premalignant condition (Pindborg and Zacharian 1965) with 30 to 40% of ihe caseCdeveloping cancer. Other workers could not establish any such relationship (Sirsat and Khanolkav, 1962) having only 4% of their cases turning malignant. In another series of 650 cases of oral cancer (Paymaster, 1956), 52% involved the tongue which is not affected by sub-mucous fibrosis, 18% were in the buccal mucosa where this condition is uncommon. The palate mucosa or anterior tonsillar pillar which are the common sites for sub-mucous fibrosis (Fig. 5)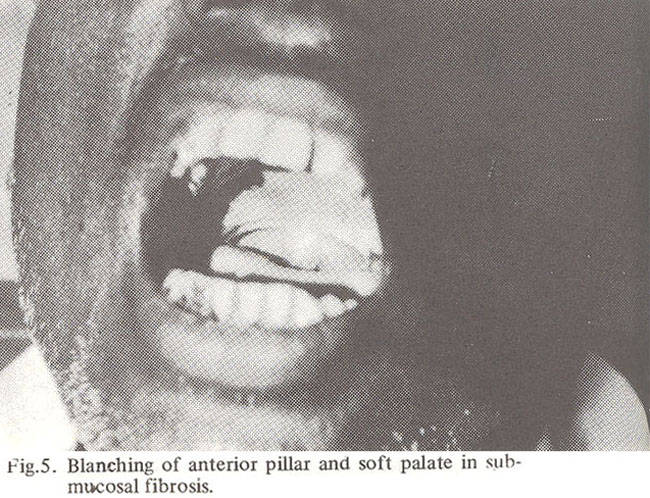
showed no involvement. In the present series no case with sub-mucous fibrosis was seen.
Acknowledgement
The authors are extremely grateful to late Dr. Haziq-ul-Yaqeen General Surgeon, K.V. S.S. SITE Hospital, Karachi for referring the cases of lead and neck lesions to centralise their manage-ment.
We are also indebted to Lt. Col (Retd) Shahabuddin, Medical Superintendent, K.V.S.S. SITE Hospital and Brig. Naqvi, Commissioner, S.E. S.S.I.for the use of hospital and records per- mission to publish this study.
References
1. Habibi, A. (1965) Cancer in Iran. A survey of most common cases.Nat. Cancer Inst., 34 : 533.
2. Harrison, D.F.N. (1972) Thoughts on present day management of Malignant tumours affecting the maxillary and ethmoidal sinuses. Proceedings of the Irish Otolaryngological Society. Report of 13th. Annual Meeting, 9.
3. Harrison, D.F.N. (1973) Laryngeal Carcinoma, Brit. Hosp. Medi.. 10 597.
4. Hirayama, T. (1966) An epidemiological study of oral and pharyngeal cancer in Central and South East Asia. Bull. World Health Org., 34 : 41.
5. ICD-O (1976) International Classification of Diseases for Oncology. World Health Orgn., GENEVA.
6. Jafarey, N.A.. Sheikh, S., Zaidi, S.H.M. (1972) Prevalence of Oral lesions in three localities of Karachi. JPMA., 22 : 125.
7. Jafarey, N.A. and Zaidi, S.H.M. (1976) Frequency of malignant turnours in Jinnah Postgraduate Medical Centre, Karachi. JPMA., 26 : 57.
8. Jafarey, N.A., and Zaidi, S.H.M. Carcinoma of oral cavity and Oropharynx in Karachi. Tropical Doctor, 6 : 63.
9. Jussawalla, D.J. Cancer incidence patterns in subcontinent of India. Proceedings Royal Soc. Med., 66 : 308.
10. Karirn, F. (1971) A pilot survey to detect cancer in symptom, biased patients in three distant district, Headquarters of East Pakistan. JPMA., 21 : 3.
11. Mehmood, Z., Jafarey, N.A., Samiuddin, M., Rais, A.K., Malick, S. and Qureishi, S.A. (1974) Dietry and other habits of people of Karachi. 24 : 222.
12. Paymaster, J.C.Cancer of baccal mucosa. A clinical study of 650 cases in Indian patients. Cancer, 9 : 431.
13. Paymaster, J.C. (1957) The problem of oral, oropharyngeal and hypolaryngeal carcinoma in India. Brit. J. Surg., 44 : 467.
14. Paymaster, J.C., Sanghvi, L.D., Ganghadharan, P. (1968) Cancer in gastrointestinal tract in Western India. Epidemiological Study. Cancer, 21: 279.
15. Pindborg, J.J. and Zacharian, J. (1965) Frequency of oral submucous fibrosis among 100 South Indians with Oral Cancer. Bullet. World Health Orgn., 32 : 750.
16. Pindborg, J.J. In oral Cancer and precancer, John Wright and Sons Limited, Bristol, P.1.
17. Sirsat, S.M. and Khanolkar, V.R.(1962) Submucous fibrosis of the palate and pillars of the fances. Ind. J. Med. Sci., 16 : 189.
18. Sobin, L.H. Cancer in Afghanistan. Cancer, 23 : 678.
19. UICC (1973) International Union Against Cancer. TNM Classification of Malignant Tumours (Supplement) GENEVA.
20. Zaidi, S.H.M., Jafarey, N.A., Ali, S.A. (1974) Cancer trends in Karachi. JPMA., 24 : 87.
21. Zaidi, S.H.M., Ahmed, S.A., Burney, M.A., Jafarey, N.A., Din, J., Khatoon, M., Masood, S.M., Rehman, M.A., and Siddiquee, M.A. (1977) Frequency of malignant tumours in seven centres of Pakistan. JPMA., 27 335.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: