
Murntaz Lakhani ( Departments of Paediatrics and Pathology, The Aga Khan University Hospital, Karachi. )
Mohammad Khurshid ( Departments of Paediatrics and Pathology, The Aga Khan University Hospital, Karachi. )
Shehla H. Naqvi ( Departments of Paediatrics and Pathology, The Aga Khan University Hospital, Karachi. )
Mohammad Akber ( Departments of Paediatrics and Pathology, The Aga Khan University Hospital, Karachi. )
November 1989, Volume 39, Issue 11
Original Article
Abstract
Congenital hypothyroidism is a preventable cause of mental retardation. Since clinical signs of congenital hypothyroidism do not generally become obvious before three months of age, screening programmes have been introduced in North America and Europe, which consist of T4 or TSH screening on newborn infants on the third day of life. The screening for congenital hypothyroidism was initiated in Pakistan by the Aga Khan University Hospital (AKUH) in March 1987. By April 1988, 5000 neonates were screened and five cases of congenital hypothyroidism were diagnosed. The study revealed the incidence of hypothyroidism to be one case per 1000 newborns which is about 4 times more than that in the West (JPMA 39: 282, 1989).
INTRODUCTION
Association of mental retardation with congenital hypothyroidism was first described in the 15th century but the horror of cretinism was expressed by Osler in 18971. In the same decade the treatment of congenital hypothyroidism with thyroid extract was reported. Sixty years after the introduction of thyroid replacement therapy, it was realised that although the treatment abolished the physical manifestations of congenital hypothyroidism, “unless it was started within the first few weeks of life serious intellectual and neurological deficits frequently persisted2”. The pre and post-natal periods are critical for brain development. Thyroid hormone is essential for the development and growth of brain3-5. Autopsies in the human infant with congenital hypothyroidism shows hypoplasia of the cerebellar and cerebral cortices, edema and incomplete myelination6. Neither T% T4 or TSH cross placental barrier to any significant degree. The fetal pituitary thyroid axis binctions independently of the maternal axis, and maternal thyroid hormones do not protect against congenital hypothyroidism. In 1972, Klein and associates7 showed that if the treatment of hypothyroid infants was started before the age of 3 months, mean 1.0. of patients was 89 whereas it was 70 when treatment was started between 3 and 6 months of age and only 54 if treatment was delayed beyond six months. Early clinical diagnosis is difficult. Few infants show diagnostic features of hypothyroidism at birth. The early manifestations are subtle, non-specific and the stigmata of “aggravated creatinism” develop only slowly. For these reasons, even in the best of circumstances less than half the children with congenital hypo-thyroidism are identified before three months of age, making the potential benefit of neonatal screening evident. A preliminary report of mass screening programme from Quebec (Canada) showed a hypothyroidism incidence of 1/7000 new-borns8. It also showed that radio-immunoassay for detection of T4 in dried filter paper blood spot was effective in detecting thyroid hormone abnormalities with an acceptable percentage of false positive measurements and no false negative results. The second International Conference on Neonatal Thyroid Screening9 indicated a prevalence of primary hypothyroidism to be aproximately one in 3800 to 4000 infants worldwide9. Screening in North West health region of England showed a significantly higher incidence of congenital hypothyroidism in Asian families - 1/918 compared with 113391 in non-Asians10. To measure both thyroxine (T4) and thyroid stimulating hormone (TSH) on all specimen is ideal but expensive. The pros and cons of using either hormone as primary screen are listed in Table I11. Japan, most of the European countries and some states in North America are using TSH screening as primary method12. The reported increased incidence of congenital hypothyroidism in babies born to Asian mothers had initiated our interest in carrying out screening in Pakistan where the incidence of congenital hypothyroidism is not known:
PATIENTS AND METHODS
From March 1987 to September 1988, 5000 neonates were screened. All neonates delivered at Aga Khan University Hospital and 4 maternity homes situated in metropolitan Karachi were included in the study. Capillary blood samples were collected on 3 circles on the filter paper provided by AKUH laboratory. A questionnaire regarding maternal health was filled before the collection of blood, especially regarding family history of thyroid disorder. The site chosen to obtain blood was the planter surface of the toot (Figure).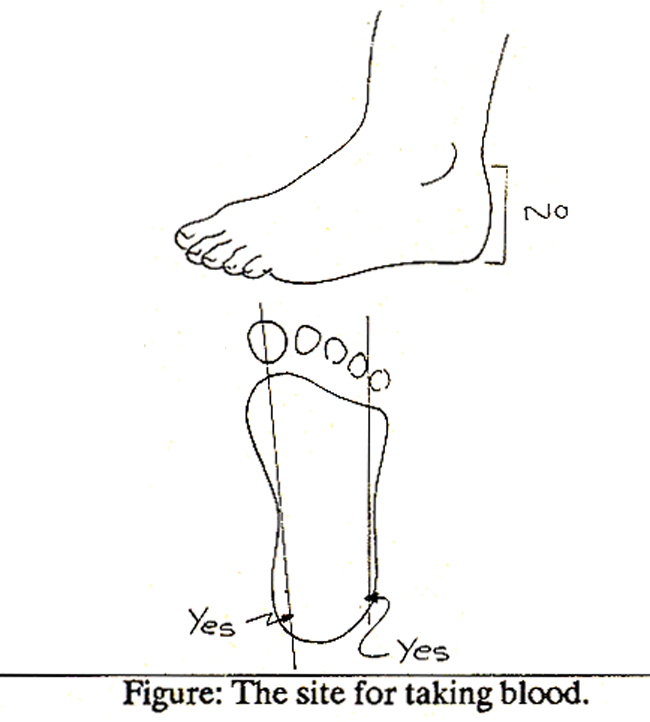
The area was wiped with 70% alcohol for one minute and allowed to dry. Skin was punctured in one continuous deliberate motion in a direction almost perpendicular to the puncture site to a depth of about 2.5 mm with a lancet. The first drop of blood was wiped off with a dry sterile swab and then the blood was collected directly from the heel on to the three circles of the filter paper. After the blood spots had dried, filter paper was sent to the laboratory. The T4 and TSH levels were measured from the blood on the filter paper by radioimmunoassay using Coat-A-count Neonatal T4 and TSH double antibody system by RIA (Diagnostic Products Corporation, Los Angeles, USA). If the specimen was found to have low T4 and high TSH then the cons centrations of T4 and TSH were confirmed on the venous sample. The established laboratory normal values ranged from: for capillary spccimens:T4, 6.9-26.4 and TSH, <20,uIU/ml., for venous sam-pies: T4, 4.5- 12.5 ug/dl and TSH 0.3-4.5 uIU/ml.
RESULTS
Of the 5000 neonates screened, 6% (300) had low T4 and normal TSH, 13% (65) had high TSH but normalT4,whiie six (0.12%) had lowT4 and high TSH. Six neonates with low T4 and high TSH were recalled for Venous sampling.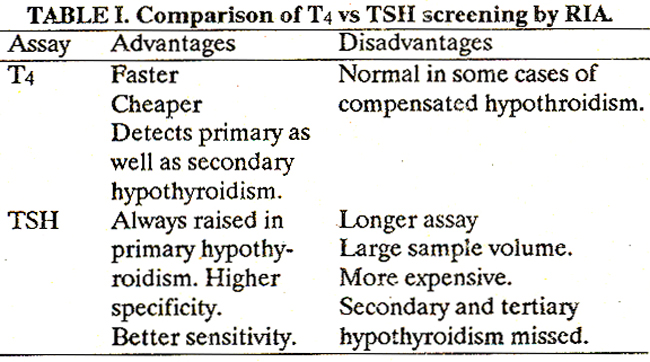
Five out of six were confirmed to have congenital hypothyroidism even on this basis of low T4 and high TSH level in serum specimen. One neonate had normal T4 but slightly elevated TSH on venous sampling which could be seen in compensated hypothyroidism. Out of 300 (6%) neonates with low T4 and normal TSH 9 were recalled for Venous sampling 8 out of 9 had normal T4 and TSH in serum. One infant with very low T4 and normal TSH in serum sample was further tested with T3 resin uptake which was significantly elevated. This is an indirect evidence of TBG deficiency. Of 65 neonates with high TSH and nonnalT4, nine were recalled. Eight out of 9 had normal values of T4 and TSH in serum sample, while one neonate had normal T4 and slightly elevated TSH which is usually seen in cases of compensated hypothyroidism. Details of five diagnosed cases is given in Table II.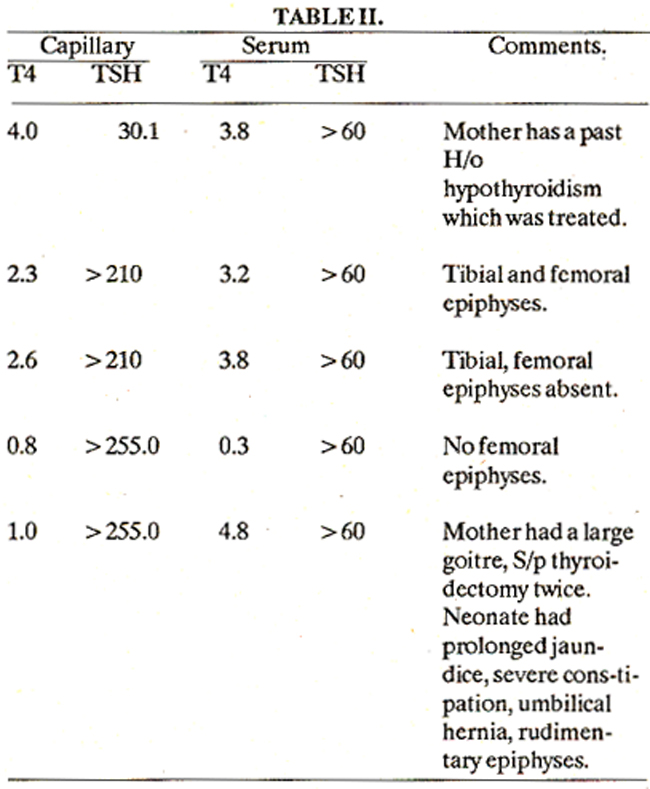
In case I there was a past history treated maternal hypothyroidism. In case V, mother had a large goitre inspite of thyroidectomy done twice. This neonate at the time of recall already had symptoms of congenital hypothyroidism which were prolonged neonatal jaundice requiring hospitalisation, severe constipation and umbilical hernia. In four cases diagnosis were further confirmed radiologically. X-ray of both knees revealed either absent or rudimentary tibia! and/or femoral epiphy-sis which is an evidence of delayed bone age in a term infant, an important feature of congenital hypothyroidism.
DISCUSSION
The objective of a screening programme for congenital hypothyroidism is early detection and treatment to minimise neurological deficiencies1. This report has revealed four-fold higher incidence of the disease in the screened population as compared to figures from North America and Europe. This incidence has been calculated excluding two cases of compensated hypothyroidism. The cause for this high incidence in our population is not clear. Radioisotope scanning of thyroid gland in these infants was not possible due to lack of facilities. This would have helped in identifying the etiology. Nutritional iodine deficiency leading to thyroid disorder is a common problem in the northern mountainous regions of Pakistan. However, this is not a common clinical problem in the seaside locale of Karachi. Although the disease is known to be more common in females, in this study there were 3 males and 2 females. Since there is a maternal history of thyroid disorder in two out of five cases, maternal antibodies may be responsible for this increased incidence but they were not tested. However, in one case where there was no history of maternal thyroid disorder, maternal serum was tested for antibodies which was negative. Our study also confirmed the previously described higher rate of false positive with T4 as compared to TSH testing. Since 90% of the cases of congenital hypothyroidism are primary in nature, TSH screening will become the future screening measure in our laboratory.
ACKNOWLEDGEMENT
The help of physicians and nurses of the Aga Khan University Hospital, The Aga Khan Maternity Homes and Sobraj Maternity Home is gratefully acknowledged. We are also indebted to Abdul Aziz for Secretarial help. We also thank medical student Jamal Mubarak for working out normal laboratory values of T4 and TSH in laboratory at AKUH.
REFERENCES
1. Osler, W. Sporadic cretinism in America. Transactions of Congress of American Physicians and Surgeons 1897; 4:169.
2. Smith, D.W., Blizzard, R.M. and Wilkins, L. The mental prognosis in hypothyroidism of infancy and childhood; a review of 128 cases. Pediatrics, 1957; 19:1011.
3. Carr, E.A. Jr., Beierwaltes, W.H., Raman, 0., Dodson, V.N., Tanton, J., Befts, J.S. and Stambaugh, LA. The effect of maternal thyroid function on fetal thyroid function and development. 3. Clin. Endocrinol. Metab., 1959; 19:1.
4. Pickring, D.E. and Fisher, D.A. Therapeutic concepts relating to hypothyroidism in childhood. J. Chron. Dis. 1968; 7: 247.
5. Eayers, J.T. Influence of the thyroid on the central nervous system. Br. Med. Bull., 1960; 16: 122.
6. Lafranchi, S.H. Hypothyroidism. Symposium on Pediatric Endocrinology. J. Pediatr. Clin. North Am., 1979; 26:1.
7. Klein, A.H., Meltzer, S. and Kenny, F.M. Improved prognosis in congenital hypothyroidism treated before age three months. J. Pediatr., 1972; 81:912.
8. D, ussault, J.F1. Preliminary report on a mass screening programme for nenmtal hypothyroidism. 3. Pediatr., 1986; 5:670.
9. Fisher, D.A. Second International Conference on Neonatal Thyroid screening Progress report. J.Pediatr., 1983; 102 :653.
10. Rosenthall, M., Addison, G.M., and Price, D.A. Congenital hypothyroidism: increased incidence in Asian families. Arch. Dis. Childh., 1988; 63:790.
11. Griffiths, K.D., and Virdi, N.K. Neonatal screening for congenital hypothyroidism by measurement of T4 and TSH. Br. Med. J., 1985; 291:117.
12. Infant screening Highlights of 4th National Symposium in Ohio Infants screening Newsletter (Harvard University, School of Medicine, Washington, D.C) April 1986, 9:1.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: