
Michelle Karim ( Departments of Medicine, Faculty of Health Sciences, The Aga Khan University, Karachi-74800. )
Waheed Khan ( Departments of Medicine, Faculty of Health Sciences, The Aga Khan University, Karachi-74800. )
Badar Farooqi ( Departments of Microbiology, Faculty of Health Sciences, The Aga Khan University, Karachi-74800. )
Imtiaz Malik ( Departments of Medicine, Faculty of Health Sciences, The Aga Khan University, Karachi-74800. )
February 1991, Volume 41, Issue 2
Original Article
ABSTRACT
One hundred consecutive patients with documented bactéremia and neutrophil count of 0.5x109 /L or below were retrospectively studied to determine the pattern of infection at the Aga Khan University Hospital in Karachi. These included patients with primary haematologic malignancies presenting with low counts, and those patients with cancer who developed neutropenia as a result of chemotherapy. The gram negative organism pseudomonas aeruginosa was the most common bacterial organism isolated constituting 31% of all positive blood cultures. Gram positive organisms were frequently isolated comprising 24% of all isolates of which 15% were Staph.aureus. Staph. epidermidis was not isolated in this series. Salmonella species were isolated in 9 patients. The other gram negative rods included non-lactose fermenting organisms frequently isolated in a nosocomial setting including Serratia and Acinetobacter. Four patients had positive fungal blood cultures. A single positive anaerobic culture was obtained. Sensitivities of the Pseudomonas aeruginosa reflected the high frequency of resistance seen in nosocomial isolates and those from the community. More than half (54.8%) of the isolates were resistant to carbenicillin and 9.6% resistant to gentamicin. Although 3.2% were resistant to cefotaxime, none were resistant to ofloxacin or ceftazidime reflecting the relatively recent arrival of the latter. In contrast, 23% of Staph: aureus were still sensitive to penicillin. Methicillin (cloxacillin) resistant Staph. aureus did not occur. However 26.6% of the Staph. aureus were resistantto erythromycin. Knowledge of the prevailing pattern of infection permits the development of investigative and therapeutic approaches of optimal efficacy (JPMA 41: 35, 1991).
INTRODUCTION
Patients with haematologic and other malignancies are susceptible to infections. Many factors predispose this patient population to infection including tumor specific deficiencies in host defence mechanisms due to malignant processes and cytotoxic chemotherapy. Neutropenic patients are most susceptible to infections caused by gram negative bacilli and gram positive cocci. Candida and aspergillus1. The spectrum of infection may be further altered by changes in medical practices (use of indwelling catheters, etc), changes in the ecology of infective agents, demography of patients at risk or by prevailing community infections2. Hence to achieve the highest percentage of survival, it is necessary to determine the pattern of infection in these patients, so that the most effective empiric therapy maybe used at the earliest sign of infection. In the present paper we retrospectively analyze, 100 positive blood cultures in patients with neutropenia. The data presented here show the similarity in patterns of infection3 and emerging bacterial resistance at a tertiary referral center in a developing country.
PATIENTS AND METHODS
Patients
This study included 100 consecutively bacteremic patients with neutropenia defmed as a neutrophil count of 0.5x109 /L or less, who developed a sustained temperature of 38 C or above. Patients who became febrile in proximity to having received blood products were excluded. Patients were included regardless of whether they had primary neutropenia related to their underlying haematologic malignancies and were therefore new admissions from the community or they were neutropenic secondary to cytotoxic therapy while in the hospital.
Microbiologic evaluation
Two sets of blood cultures were obtained. Brain heart infusion broth was used for aerobic cultures and thioglycolate broth for anaerobic cultures. Cultures were incubated for 7 days. Blind sub- cultures of medium and gram stains were done daily on blood agar plates and after 48 hours additionallyon Sabouraud Dextrose Agar for betteryleld of fungus. On the 5th day both anaerobic and aerobic cultures were plated on chocolate and blood agar plates.
RESULTS
Analysis of 100 positive blood cultures in neutropenic patients with both haematologic and other malignancies (Table I)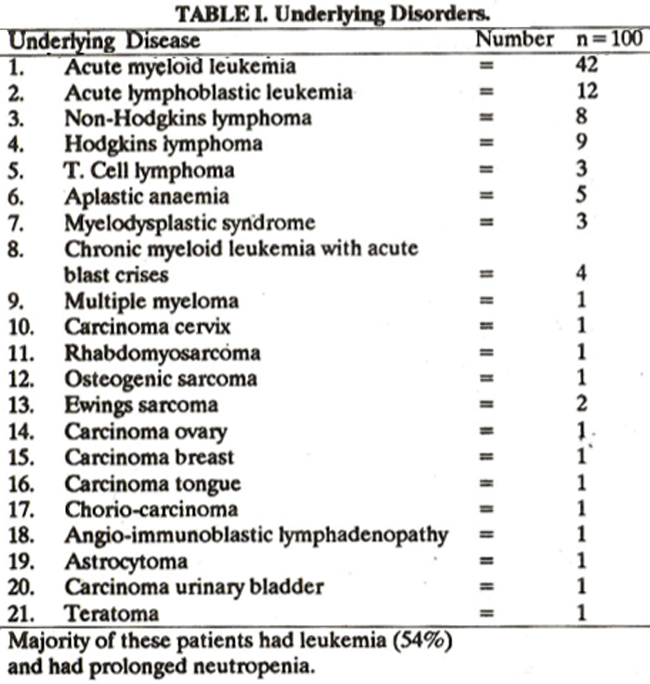
revealed Pseudomonas aeruginosa as the most common organism. Majority of the patients had underlying leukemia and remained neutropenic for prolonged time periods. The different types of organisms and the numbers cultured are shown, in Table II.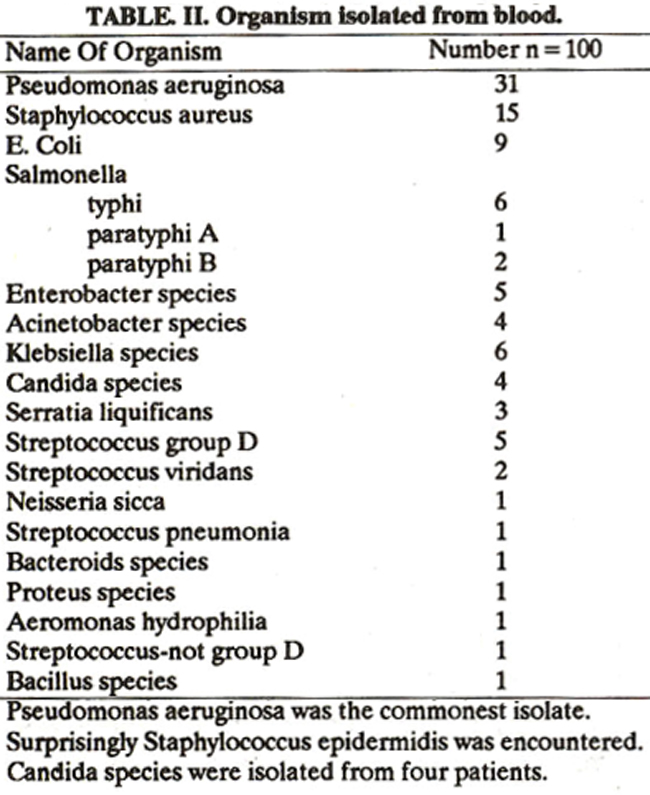
Pseudomonas aeruginosa was isolated from 31% of the cases, followed by Staph. aureus in 15%. Salmonella species isolated in 9% of cases is much higher than reported elsewhere. These isolates have not been separated according to the type of malignancy or the time of positivity i.e.on admission or afterwards.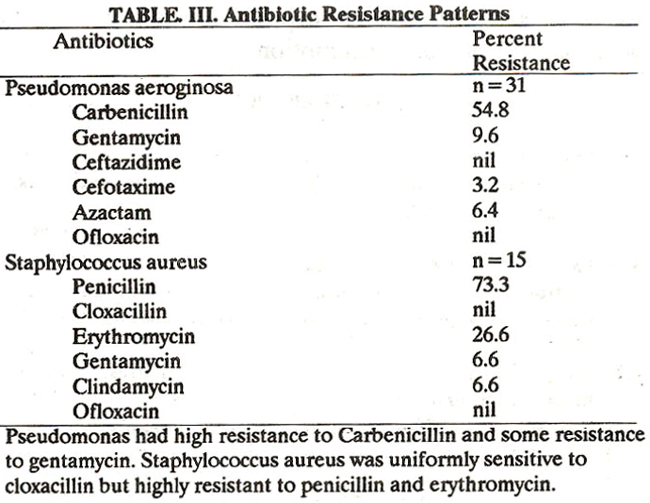
Table III indicates sensitivity patterns of pseudomonas aeruginosa and Staph. aureus. Pseudomonas was highly (54.8%) resistant to carbenicillin and 9.6% isolates were resistant to gentamycin whereas, 73% of Staphylococcus aureus were resistant to penicillin and 26% to Erythromycin.
DISCUSSION
Malignancies, as well as their treatment, are associated with potentially serious and even life-threatening complications. One of the commonest of these is the development of infections, caused by a wide variety of pathogenic organisms. Although many reasons exist for the enhanced susceptibility to infections, neutropenia is the single most important factor. These patients require prompt empiric antibiotic therapy, if they become febrile, as delay often results in fatality4. Selection of the antibiotic regimen should take into consideration the organisms that are prevalent in the hospital and their usual pattern of antibiotic susceptibility. The spectrum of organisms causing infections in neutropenic patients changes according to the duration of neutropenia5. The concept of empiric antibiotic therapy was in itiated for febrile leukemic patients in the 1960’s because of the exceptionally high mortality rate in neutropenic patients if antibiotic administration was delayed until the organism was identified6 . Since neutropenic patients are unable to mount an adequate inflammatory responses, they are mostly dependent on antibiotics to control infections. Results of clinical studies have clearly demonstrated that synergistic antibiotics with high serum bactericidal activity are critical in the management of gram negative bacillary infections7. There has been a shift in the microbial flora at many oncology centers during the last 10 years. Increasing number of gram positive organisms specifically Staph. epidermidis, Staph. aureus, Streptococcus and Bacillus species are being encountered8. However, although these infections produce moderate morbidity (e.g.fever), mortality is fairly low. Therefore empiric treatment is mostly directed at the gram-negative organisms. Most clinical studies suggest that empiric therapy using combinations of two bactericidal antibiotics is necessary9-12. Effective antibiotic combinations have usually included an aminoglycoside plus an extended spectrum penicillin (e.g. ticarcillin or carbenicillin) or a broad spectrum antipseudomonal cephalosporin (e.g. ceftazidime, cefotaxime). Double beta-lactam combinations have also been used but some concern has been expressed that these combinations may interact in an antagonistic fashion13,14. Inmost studies, however, the double beta-lactam regimen has been as effective as the beta-lactam plus aminoglycoside15,16. In the patients with prolonged neutropenia, on multiple antibiotics, the likelihood of fungal infections, e.g., Candida and Aspergillus increase tremendously17. In these cases empiric amphotericin therapy may have to be considered. This study demonstrates that in our hospital setting Pseudomonas aeruginosa is the commonest bacterial isolate, followed by Staph. aureus. We have routinely used cloxacillin and amikacin as the empiric antibiotic therapy. Besides covering the two most likely organisms, it also covers against gentamycin-resistant Pseudomonas. In those responding poorly, we add cefotaxime or azactam to enhance gram negative coverage. Growth of fungus in four patients indicates that it may not be an uncommon problem in Pakistan and empiric amphotericin therapy is indicated in those who continue to befebrile and neutropenicwithout any evident infection We conclude that gram negatives are the commonest bacterial isolates in neutropenic febrile patients, followed by Staph. aureus. Choice of empiric antibiotic therapy should be tailored towards these organisms. Similar studies need to be repeated at regular intervals to evaluate any changes in bacteriologic spectrum or their antibiotic susceptibility.
REFERENCES
1. Whimbey, E., Kiehn, T. E., Brannon, P., Blevins, A. and Armstrong. D. Bacteremia and fungemia in patients with neoplastic disease. Am. J. Med., 1987; 82: 723.
2. Pizzo, P.P. Practical consideration for the management fever and infections in neutropenic patients. Clin. Oncol., 1985; 4: 405.
3. Schimpff, S. C., Young, V. M., Greene, W. H., Vermevlen, G. D., Moody, M. R and Wiernik, P. H. Origin of infection in acute nonlymphocytic leukemia. Significance of hospital acquisition of potential pathogens. Ann. Intern. Med., 1972; 77: 707.
4. Bodey, G. P. Infection in patients: continuing association 1986. Am. J. Med., 1986; 81 (Suppl. 1A): 11.
5. Bodey, G. P., Buckley, M., Sathe, Y. S. and Freireich, E. J. Quantitative relationships between circulating leukocytes and infection in patients with acute leukemia. Ann. Intern. Med., 1966; 64: 328.
6. Bodey, 0. P., Jadeja, L. and Elting, L. Pseudomonas bacteremia; retrospective analysis of 410 episodes. Arch. Intern. Med., 1985; 145:1621.
7. Klastersky, J., Cappel, R. and Daneau, D. Clinical significance of in vitro synergism between antibiotics in gram-negative infections. Antimicrob. Agents Chemother., 1972; 2: 470.
8. EORTC Antimicrobial cooperative group. Gram-positive septicemia in cancer patients (abstract no. 679), in Program and abstracts of the 26th Interscience Conference on Antimicrob. Agents Chemotherapy. Washington. American Society for Microbiology, 1986.
9. Wade, J. C. and Schimpff, S. C. Approaches to therapy for bacterial infections in the granulocytopenic patients in infections in cancer patients. Edited by J. Klastersky, New York, Raven Press, 1982; p.105.
10. Anderson, E. T., Young, L. S. and Hewitt, W. L. Antimicrobial synergism in the therapy of grain-negative rod bacteremia. Chemotherapy, 1978; 24: 45.
11. Love, L. J., Schimpff, S. C., Schiffer, C. A. and Wiernik, P. H. Improved prognosis of granulocytopenic patients with gram -negative bacteremia .Am. J. Med., 1980; 68: 643.
12. Klastersky, J., Cappel, Rand Daneou, D. Clinical significance of in vitro synergism between antibiotics in gram negative infections. Antimicrob. Agents Chemotherapy, 1972; 2: 470.
13. Kuch, N. A., Testa, R T. and Forbes, M. In vitro and in vivo antibacterial effects of combinations of beta-lactam antibiotics. Antimicrob. Agents Chemotherapy, 1981; 19: 634.
14. Sander, C. C., Sander, W. E. Jr. and Goering, R. V. In vitro antagonism of beta-lactam antibiotics by cefoxitin. Antimicrob. Agents Chemother., 1982; 21: 968.
15. Winston, D. J., Barnes, R. C., Ho, W. 0., Young, L. S., Champlin, R E. and Gale, R. P. Moxalactam plus piperacilin versus moxalactam plus amikacin in febrile granulocytopenic patients. Am. J. Med., 1984; 77: 442.
16. Feld, R, Louie, T. J., Mandell, L., Bow, E. J. et al. A multicenter comparative trial of tobramycin and ticarcillin vs moxalactam and ticarcillin in febrile neutropenic patients. Arch. Intern. Med., 1985;145: 1083.
17. Pizzo, P. A., Robichaud, K. J., Wesley, Rand Commers, J. R Fever in the pediatric and young adult patients with cancer, a prospective study of 1001 episodes. Medicine, 1982; 61: 153.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: