
Zulfiqar A. Bhutta ( Departments of Paediatrics, Faculty of Health Sciences, The Aga Khan University, Karachi. )
Shehla H. Naqvi ( Departments of Paediatrics, Faculty of Health Sciences, The Aga Khan University, Karachi. )
Shahana Durrani ( Departments of Phannacology, Faculty of Health Sciences, The Aga Khan University, Karachi. )
Amin Suria ( Departments of Phannacology, Faculty of Health Sciences, The Aga Khan University, Karachi. )
February 1991, Volume 41, Issue 2
Original Article
ABSTRACT
In a prospective study we compared two different dosage regimens of IV chioramphenicol succinate (100 mg/kg/day and 75 mg/kg/day) in children with culture proven typhoid. Trough and peak blood samples, obtained at 48 hrs, were analysed for free chioramphenicol by high pressure liquid chromatography (HPLC). Although the mean trough (8.8±1.7 versus 5.4±2.6 mcg/ml) and peak (19.9±12.2 versus 15.4±6.1 mcg/ml) chloramphenicol concentrations were comparable in both groups, a ‘significantly wider range was found in the group receiving 100 mg/kg/day. Potentially toxic levels (>30 mcg/ml) developed in two patients with liver dysfunction. Chloramphenicol in a dosage of 75 mg/kg/day Is adequate and safe for the treatment of paediatric typhoid (JPMA 91: 26, 1991).
INTRODUCTION
Chloramphenicol is considered as the treatment of choice in typhoid fever1. The oral preparation, Chioramphenicol palmitate is used in the treatment of typhoid except when vomiting ileus or toxicity preclude oral therapy. Intravenous succinate ester of chloramphenicol are used in such circumstances. Free chioramphenicol. after the succinate or palmitate group has been cleaved, is the microbiologically active form which isexcretçd following glucuronidation in the liver. The various known path- ways2-5 of human metabolism of chloramphenicol suecinate (CS) are shown in Figure 1.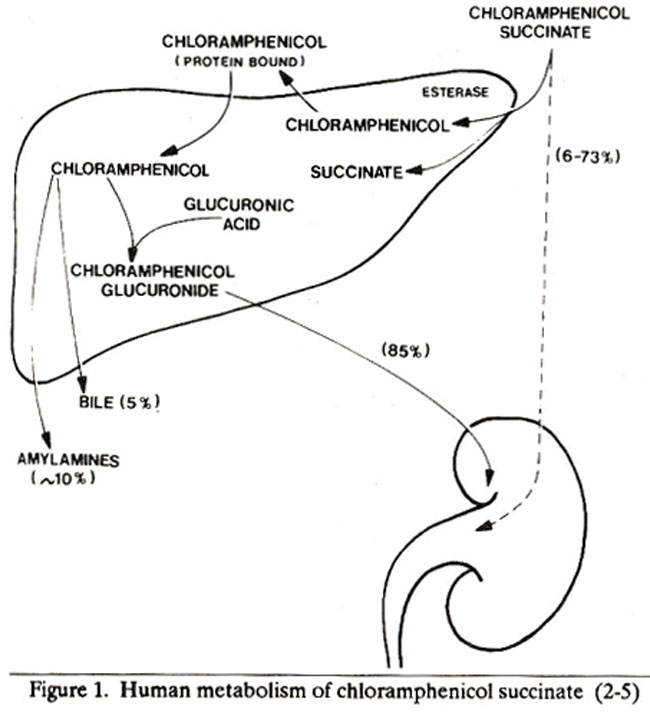
The. metabolism of chioramphenicolpalmitate in the liver is similar, except for the initial hydrolysis of the pahnitate ester in the gastrointestinal tract lumen6. Some studies have demonstrated wide variability in the pharmacokinetics of CS2,3. This is chiefly related to variation in the rate o1 hydrolysis of the succinate ester in the iiver and urinary losses of CS2,7. There is very little data on chioramphenicol pharmacokinetics in typhoidal salmonellosis. Little still, is known about appropriate dosage in children with typhoid fever and dosage schedules ranging from 50 - 100 mg/kg! day have been recommended8. As free chloramphenicol is principally conjugated in the liver, therefore impaired chioramphenicol clearance and potentially toxic serum levels may develop, in patients with liver dysfunction9,10. The association of hepatic dysfunctionwith typhoid has also been demonstrated in adults11,12 and children13 in a number of studies. The use of chlorainphenicol therefore, in children with typhoid and hepatic dysfunction may also be associated with potential toxicity. We conducted a prospective study to compare two different dosage schedules of CS in paediatric typhoidal salmonellosis, and to assess the effect of concomitant hepatic dysfunction on serum concentrations of chloramphenicol.
PATIENTS AND METHODS
The study was conducted over an 18 months period (May 1987 - September 1988) at the Aga Khan University Hospital (AKUH), Karachi. Patient selection: All children (age 6 months - 14 years) presenting to the Department of Paediatrics with suspected typhoid were studied. Patients were prospectively randomized for inclusion in the study using sealed envelopes containing the randomization dose. Children with neutropenia (neutrophils <1000/mm3) and those who had received chloramphenicol therapy in the preceding 7 days, were excluded from the study. Informed consent was obtained from the parents/guardians of the children prior to inclusion in the study. The children were nursed for the duration of the study on the paediatric ward and examined twice daily by a medical officer. Chloramphenicol dosage schedule & administraUon: Patients were randomized to receive intravenous CS either 100 mg/kg! day (Group A) or 75 mg/kg/day (Group B) intravenously in a six hourly dosage for 48 hours. The drug was administered after dilution in normal saline as an infusion over 30 minutes. A daily record of clinical status, including temperature, mental status, hydration, jaundice, abdominal discomfort, visceromegaly, diarrhoea and vomiting was maintained. The patients were discharged home on oral chioramphenicol palmitate in the same dosage after remaining afebrile for 24 hrs (axillary temperature 37°C).
Laboratory investigations: A blood culture was obtained in all cases with suspected typhoid fever. Two blood culture bottles (containing brain heart infusion and thioglycollate broth) were inoculated with 2-3 ml of venous blood and incubated for 7 days at 37°C. A bone marrow culture was also obtained and inoculated similarly, if there was a history of prolonged illness ( >15 days) or antibiotic administration for >72 hours prior to presentation. Each culture bottle was examined daily and subcultured onto blood agar and MacConkey\\\'s media after 24, 48 and 72 hours and on the 5th and 7th day of incubation, non- lactose fermenting colonies from MacConkey’s medium were tested for salmonella by slide agglutination with specific antisera.A stool microscopy and culture were obtained if there was concomitant diarrhoea at presentation and stool specimens were similarly cultured on MacConkey agar. Biochemical tests for identification were performed, using API 20E strips (Analytical Profile Index API System, S.A. Lambalmeles Grottes-38390, Montalieu, Vercien, France). Baseline investigations including complete blood count (CBC), differential count, reticulocyte count, serum bilirubin, SGPT (Alanine transaminase), Alkaline phosphatase and bicarbonate, were obtained at admission prior to institution of therapy.These investigations were repeated after 48 hours of therapy. CBC was analyzed on a coulter counter (Coulter Inc, USA) whereas the bicarbonate and liver function profile were assessed on an autoanalyzer (Beckmann Inc., Astra, Ca).
Chloramphenicol sampling and assay: Blood samples (3 ml) were obtained by venepuncture 48 hours after initiation of therapy, before and one .hour after cessation of chloramphenicol infusion. Plasma was frozen at -80°C until analysis. Analysis was done on 50 microlitre sample of plasma by high pressure liquid chromatography (HPLC) using the method of Nielsson-Ehle et al14 with some modifications. Novapak, microbondapak C18 column, 25cm x 2.1 mm id., (Waters Associates, USA) was used. Mobile phase was acetic acid, water and methanol in ratios of 1:62:37. Flow rate of mobile phase was 1.0 ml per minute. The FIPLC system (Waters Associates, USA) consisted of a pump M- 6000 A; a variable LC spectrophotometer 440 with absorbance set at 280 nm; WISP 710 B injector, Data Module 730 and a System Controller 720. All solvents used were of ultra high purification HPLC grade. Free chloramphenicol for standards, was obtained from Parke Davis (Pakistan) Ltd. Standard curve of chloramphenicol was constructed using 5, 10,20,30 and 50 mcg free chioramphenicol per ml. A four point standard curve, prepared in water, included concentrations of 50 to 6.25 mcg/ml. Peaks were detected under isocratic conditions. Linear regression analysis of Peak heights and chioramphenicol concentrations gave a correlation coefficient of 0.99. Concentration of free chloramphenicol in plasma was calculated from the standard curve and reported as mcg free chioramphenicol /ml (Figure 2).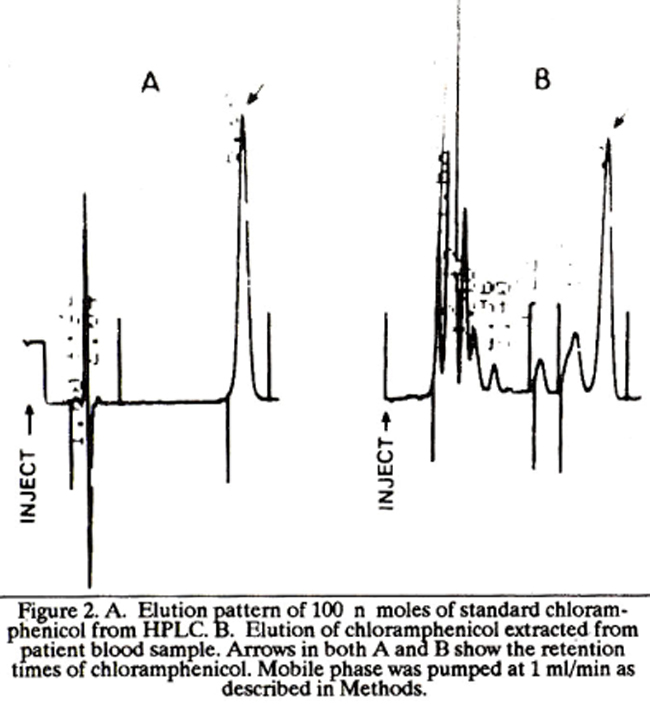
Follow up: All patients were followed up for 12 weeks after discharge to assess clinical status.
Statistical analysis: Data was analysed using chi square analysis with Yates correction and t test.
RESULTS
Twenty five children enrolled in the study had culture proven typhoid.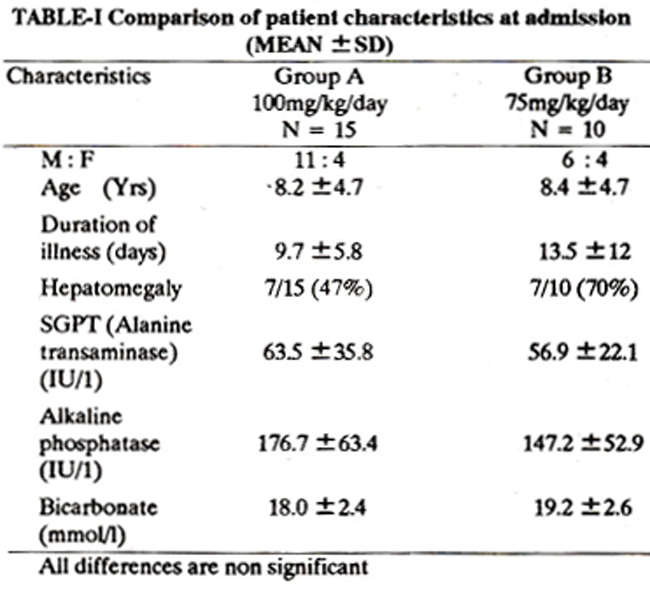
Table lists the clinical details for the two groups of patients studied. There was no significant difference between the two groups for age, weight, severity of illness or baseline liver function. Although hepatomegaly was seen in 15125 (60%) patients at admission, significant hepatic dysfunction as evidenced by hepatomegaly and two folds elevation of SGPT was found in 4/15(27%) and 6/10 (60%) patients in groups A and B respectively, at initiation of therapy. There was a wide range of trough concentrations in group A which had received 100 mg/kg/ day. Two children developed trough levels of chioramphenicolin excess of 30 mcg/ml. This led to a large standard deviation and so the difference in the mean trough concentrations of the two groups was not statistically significant (8.8 ± 7.7 versus 5.4 ± 2.6 mcg/ml, mean ± SD, x2= 0.2, P = NS). Similarly, there was a wider range of peak serum concentrations in group A. Three children (20%) on 100 mg/kg/ day dosage, developed peak levels of chioramphenicol in excess of 30 mcg/ml (Figure 3).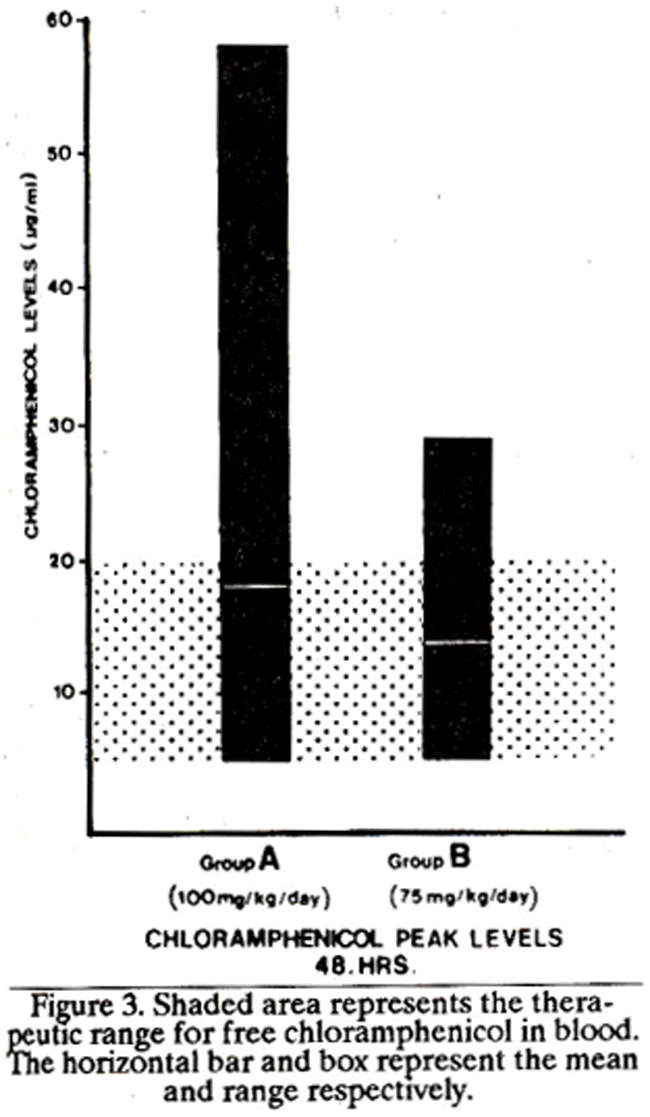
However, the mean peak serum concentrations for both dosage groups are comparable (19.9 ± 12.2versus 15.4 ± 6.1 mcg/dl, mean ± SD, X2 = 0.23, P=NS). Most of the high levels of chioramphenicol were found in children with significant hepatic dysfunction. Four of the five children with chioramphenicol levels greater than 30 mcg/ml had SGPT (Alanine transaminase) values >100 lUll. A significant correlation was also found between chioramphenicol trough levels at 48 hours and corresponding serum SGPT (Alanine transaminase) values (Y = -2.5 + 0.19; r =0.68, P< 0.001) (Figure 4).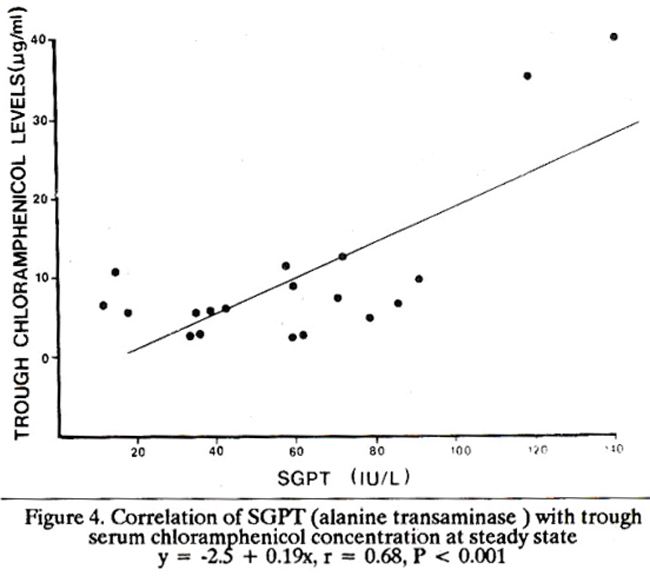
There was no significant difference between the two groups for anyof the haematological indices at 48 hours and no child developed neutropenia or anaemia. The mean reticulocyte count for group A was 1.4 ± 0.6% versus 1.1 ± 0.9 % for group B (P = NS). The SGPT (Alanine transaminase) values at 48 hours were also comparable (57 + 24 versus 54 + 24 IU/I, P=NS). The mean serum alkaline phosphatase value was slightly higher for group. A children at 48 hours in comparison with group B (218 + 128 versus 131 + 47 IU/1, P<0.05). Twenty children (80%) were infected with salmonella typhi and S paratyphi strains which were susceptible to chloramphenicol. When these children were treated with the two treatment regimens, there was no difference between the two groups for time to defervescence (4.4+2.1 versus 4.4 + 1.8 days, mean + SD, P=NS). No child relapsed after completion of the course of therapy. The five children infected with chloramphenicol-resistant strains of salmonella typhi were changed to appropriate antibiotic when the sensitivity results were available, and all recovered uneventfully.
DISCUSSION
Our study aimed to study the serum levels and response to two different dosage regimens of chloramphenicol in children with typhoid, We chose is study the intravenous preparation of chloramphenicol but the post-hydrolytic metabolism and pharmacokinetics of the oral form i.e. chioramphenicol palmitate is similar15 and the results would be equally applicable. The minimal inhibitory concentration of chloramphenicol against most susceptible organisms is 0.5 - 2.0 mcg/dl16 and the usual serum levels required to achieve satisfacto7 antibacterial activity range from 5 - 20 mcg/ml3,15. . The dose related bone marrow suppression generally appears when chlorampbenicol concentration exceed 25 mcg/ml17 and it is therefore imperative that every effort should be made to ensure that the levels remain in the therapeutic range to avoid the risk of toxicity. With wide individual variation in the metabolism of chloramphenicol in the paediatric age group 18,19 this may necessitate measurement of serum levels. Studies in adults have also shown the association of chloramphenicol toxicity with derangement of liver function20,21. Most such studies have found decreased clearance, increased half-life and higher serum levels of chloramphenicol in association with liver disease. Azzolini et al22 found a significant correlation between serum albumin and bilirubin values with cbloramphenicol levels, whereas Slaughter et al7 could not find any association between liver function tests and chloramphenicol dosage. Of the various liver disorders studied by Narang et al20 hepatitis was associated with the highest serum chloramphenicol levels, suggesting a specific relationship with hepatocellular derangement. The presence of significant impairment of hepatic function in some patients with typhoid is well documented and may have a wide spectrum. The bepatic dysfunction may be severe enough to manifest as clinical jaundice23 but is frequently subclinical, discernible on laboratory testing only24. The exact patbogenesis of liver involvement in typhoid remains unclear. The organisms proliferate in the reticuloendothelial system but this should not lead to hepatocellular dysfunction. Other factors such as endotoxaemia, may also have a contributory role in the alteration of liver function in typhoid. In our study, some children with typhoid and concomitant hepatic dysfunction, developed potentially toxic serum concentrations of chloramphenicol after intravenous CS. Our findings of a positive correlation between SGPT (Alanine transaminase) and trough chloramphenicol levels at 48 hours also tends to support this observation. The clinical significance of toxic chioramphenicol levels in our study population is unclear. None of the patients exhibited any signs of clinical and baematological toxicity and all recovered uneventfully. Acidosis, due to probable interference with mitochondrial electron transport has been described as an early manifestation of chioramphenicol toxicity25. It is interesting to note that the lowest serum bicarbonate value in our study (11 mmol/l) was seen in the infant who had significant hepatic derangement and also developed a peak chioramphenicol concentration of 53 mcg/ml. Ideally chloramphenicol levels should be measured in all children but this is clearly an expensive and impractical proposition for most of the developing countries where typhoid is endemic. A safer alternative would be judicious use of chloramphenicol in the right dosage. Our data shows that therapeutic concentrations are obtained with a dose of 75 mg/kg/day. Potentially toxic, serum concentrations of chioramphenicol are likely to occur in children on 100 mg/kg/ day of the drug in the presence of liver dysfunction due to typhoid. Therapeutic serum concentrations are obtained with a dose of 75 mg/kg/day with comparable clinical efficacy to the higher dose. No instance of toxic serum concentration was found in this group of patients. We suggest that 75mg/kg/day chloramphenicol should be used as standard dose for children with typhoid. If the child has evidence of significant hepatocellular involvement, serum concentrations should be monitored, the dose should be further reduced or an alternative drug employed for therapy.
ACKNOWLEDGEMENT
This study was supported by an Aga Khan University research grant 100-397/07-433. The authors are grateful to Ms Amynah Rehimi for her excellent assistance in typing the manuscript.
REFERENCES
1. Rowe, B., Threlfall, EJ. and Ward, L. R. Does chloramphenicol remain the drug of choice low typhoid. Epidemiol. Infect., 1987; 98: 379.
2. Kauffman, R. E., Miceli,J. N., Strebel, L, Buckley,J. L., Done,A.K and Dajani, A. S. Pharmacokinetics of chloramphenicoi and chloramphenicol succinate in infants and children. J. Pediatr., 1981;98: 315.
3. Friedman, C. A., Lovejoy, F. C. and Smith, A. L Chloramphenicol disposition in infants and children. J. Pediatr., 1979; 95: 1071.
4. Laferriere, C. I. and Marks, M. I. Chioramphenicol. Properties and clinical use. Pediatr. Infect. Dis., 1982; 1: 257.
5. Smith, AL and Weber, A. Pharmacology of chloramphenicol. Pediatr. Clin. N. Am., 1983; 30: 209.
6. Lietman, P.S. Oral chloramphenicol therapy (editorial).J. Pediatr., 1981; 99: 905.
7. Slaughter, It L., Pieper, J. A., Carra, F. B., Brodsky, B. and Koup, J. R. Chloramphenicol sodium succinate kinetics in critically ill patients. Clin. Pharmacol. Therap., 1980; 28: 69.
8. Feigin, It D. Typhoid fever, in Nelson’s textbook of pediatrics. Edited byBehrman, R. B. and Vaughan, V. C. 13th ed. Philadelphia Saunder, 1987, p. 602.
9. Ramachandran, S., Godfref, J. J. and Perera, M.V.F. Typhoid hepatitis. JAMA., 1974; 230: 236.
10. Ayhan, A., Gokoz, A., Karacadag, S. and Telatar, H. The liver in typhoid fever. Am. J. Gastroenterol., 1973; 59: 141.
11. Suhrland, L G. and Weisberger, A. S. Chloramphenicol toxicity in liver and renal disease. Arch. Intern. Med., 1963; 112: 747.
12. Koup, 3. It, Lau, A. H., Brodsky, B. and Slaughter, R. L Chloram phenicol pharmacokinetics in hospitalized patients. Antimicrob. Agents Chemother., 1979; 15: 651.
13. Bhutta, Z. A. and Shaikh, S. A. Diagnostic difficulty in partially treated typhoid. York, Paper read at the Annual mccting of British Paediatric Association, 1987.
14. Nilsson-Ehle, I., Kahlmeter, G. and Nilsson-Ehle, P. Determination of chloramphenicol in serum and CSF with high pressure liquid chromatography. 3. Antimicrob. Chemother., 1978; 4: 169.
15. Pickering, L K., Hoecker,J. L., Kramer, W. G., Kohl, S. and Cleary, T. G. Clinical Pharmacology of two chloramphenicol preparations in children; sodium succinate (IV) and palmitate (oral) esters. J. Pediatr., 1980; 96: 757.
16. Panky, G. A. and Horton, 3. M. Chloramphenicol, in antimicrobial therapy. Edited by Ristuccia, A, M., New York, Raven Press, 1984; 249: 53.
17. Scott, J. L., Finegold, S. M., Belkin, G. A. and Lawrence, J. S. A controlled double-blind study of the hematologic toxicity of chloramphenicol. N. Engl. J. Med., 1965; 272: 1137.
18. Sack, C. M., Koup, 3. R. and Smith, A. L. Chloramphenicol phar macokinetic in infants and young children. Pediatrics, 1980; 66:579.
19. Mulhall, A., de Louvois,J. and Hurley, It The phannacokineticsof chioramphenicol in the neonate and young infant. J. Antimicrob. Chemother., 1983; 12: 629.
20. Narang, A. P., Datta, D. V., Nath, N. and Mathur, V. S. Phar macokinetic study of chloramphenicol in patients with liver disease. Eur. J. Gin. Pharmacol., 1981; 20: 479.
21. Kunin, C. M., Glazko, A.J. and Finland, M. Persistence of antibiotic in blood of patients with acute renal failure. II. Chioramphenicol and its metabolic products in the blood of patients with severe renal disease or hepatic cirrhosis. J. Gin. Invest., 1959; 38: 1498.
22. Azzolini, F., Gazzaniga, A., Lodola, E. and Natangelo, It Elimination of chioramphenicol and thiamphenicol in subjects with cir rhosis of the liver. Int. J. Clin. Pharmacol. Ther. Toxicol., 1972; 6: 130.
23. Singh, D. S., Nair, P. N. B.., Krishnasamy, S., Aurora, A. L, Chandrasekar,S. and Bisht, D, B. Jaundice in typhoid fever. 3. Trop. Med. Hyg., 1978; 81: 68.
24. Klotz, S. A., Jorgensen, 3. H., Buchwold, F. 3. and Craven, P. C. Typhoid fever, an epidemic with remarkably few clinical signs and symptoms. Arch. Intern. Med., 1984; 144: 533.
25. Evens, L S. and Kleiman, M. B. Acidosis as a presenting feature of chloramphenicol toxicity. J. Pediatr.,1986; 108: 475.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: