
Wasim Jafri ( Department of Medicine, Aga Khan University Hospital, Karachi. )
Zaigham Abbas ( Department of Medicine, Aga Khan University Hospital, Karachi. )
Saeed Hamid ( Department of Medicine, Aga Khan University Hospital, Karachi. )
Hasnain Shah ( Department of Medicine, Aga Khan University Hospital, Karachi. )
Haleem Khan ( Department of Medicine, Aga Khan University Hospital, Karachi. )
December 1992, Volume 42, Issue 12
Original Article
Omeprazole inhibits the gastric secretion by altering the activity of H + /K+ ATPase1,2. The drug itself is inactive but is converted to the active form, a sulfonamide in the acid milieu of canaliculi of actively secreting gastric parietal cells3. Though the plasma half life is 60 minutes, the drug binds covalently with H+/K+ATPase and duration of action is thereafter increased to greater than 24 hours4. Distal oesophagitis is a complication of gastro-oesophageal reflux. Number and duration of episodes of reflux are important in the pahogenesis5-7. The aim of this study was to assess the efficacy of omeprazole 20 mg once daily in our patients for short term treatment of refiux oesophagitis.
PATIENTS, METHODS AND RESULTS
This was an open labeled, non-comparative single centre study. Outpatients aged 18-70 with endoscopic findings of reflux oesophagitis (grade I to III) were included in the study. Exclusion criteria were pregnant and lactating mothers, treatment with anti-ulcer or anti-refiux drugs within a week prior to inclusion, patients with concomitant gastric or duodenal ulcer, pyloric stenosis, or any malignant lesion as evident on gastroscopy, oesophageal varices, stricture or Barrett’s oesophagus, previous gastro-oesophageal surgery, patients with abnormal renal or hepatic functions and patients requiring regular use of NSAIDs. Before entry, the severity of symptoms and personal habits were assessed. A complete physical examination was performed. Lab investigations including complete blood count (CBC), ESR, urinalysis, blood urea nitrogen (BUN), creatinine, biirubin, alanine aminotransferase (ALT) and alkaline phosphatase were done. Endoscopy was performed within a week prior to the inclusion. Informed consent was taken from all the patients. Patients’ symptoms like heart burns and pains were graded from 0 (none) to 3 (severe). Occasional episodes not interfering with the normal activity corresponded to grade 1 (mild), episodes interfering with normal activity as grade 2 (moderate), frequent episodes constantly interfering with normal activity as grade 3 (severe). Oesophagitis was graded as follows: Grade I, erythema, hyperemia or mucosal friability; grade II, superficial erosions; grade III, ulcerations and grade W, complications, e.g., strictures. Patients were seen at two and four weeks to record severity of symptoms and any adverse effects, physical examination and check of left over capsules. Concomitant use of anti-refiux or other anti-ulcer drugs was forbidden during the study period. Endoscopy was repeated by the same endoscopist at 29±3 days and laboratory tests performed. Thirty consecutive patients were entered in the study. The clinical characteristics and results are summarized in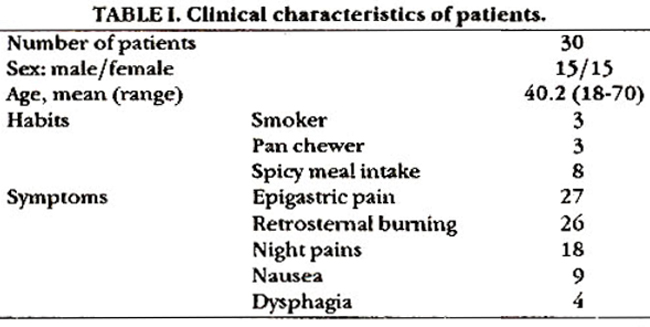
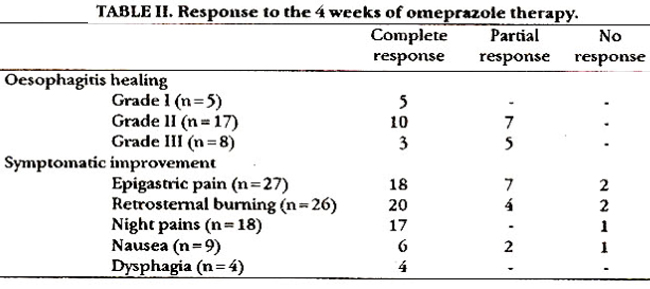
Table I and II and Figure 1 and 2.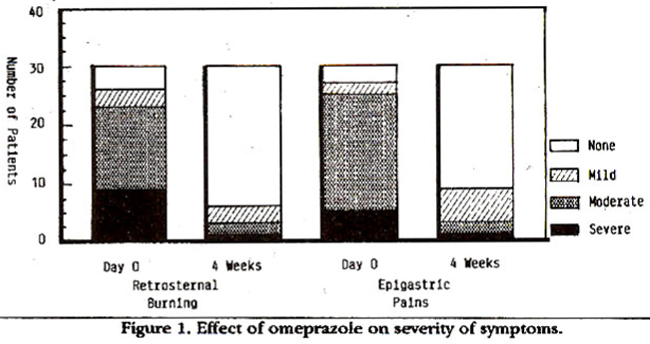
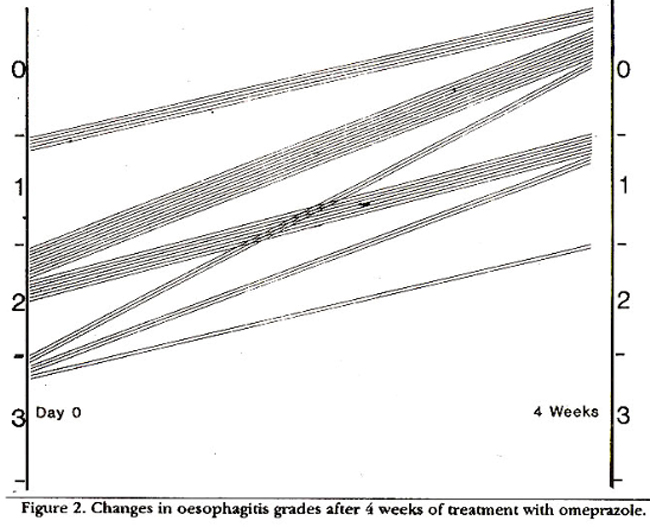
Healing defined as complete disappearance of all the lesions and re-epithelization of oesophageal mucosa on endoscopic examination was seen in 19 of 30 patients (68%). Twenty of 30 patients became asymptomatic and another 9 patients improved symptomatically. No major clinical or biochemical side effects were observed. Only one patient complained of some decrease in appetite but he completed the trial.
COMMENTS
The randomized clinical trials have proved the superiority of omeprazole over H2 - receptor antagonists8-13. The healing rate at 4 weeks varied between 67-85% as compared to 27-31% when using ranitidine. Much higher healing rate was observed at 8 weeks with omeprazole; 85-96% with omeprazole vs 38-50% with ranitidine11-13. There was significantly better symptomatic improvement with omeprazole. Our results are in accordance with the previous studies. We used 20 mg of omeprazole daily and assessed our patients at 4 weeks. The healing rate was 63%. Complete healing was observed in all the cases of grade I oesophagitis and in majority of the patients of grade 11(10 out of 17). The studies indicate that the acid is the major factor in the development of reflux oesophagitis. Omeprazole 20 mg produces 90% reduction in the intragastric acidity whereas 40-60 mg produces 96-98% reduction14-16. Elevation of gastric pH heals peptic oesophagitis but it does not significantly effect the frequency of postprandial transient lower oesophageal sphincter relaxations and magnitude of basal lower oesophageal sphincter pressure17,18. Also omeprazole has no significant effect on gastric emptying in humans19.
REFERENCES
1. Sacbs, G., Carlsson, E., Lindberg., P. and Wallmark, B. Gastric H. K-ATPase as therapeutic target. Annu. Rev. Pharmacol. Toxicol., 1988;28:269-84.
2. Lind, T., Ccderberg., C., Ekenved, 0., Haglund, U. and Obte, L Effect of omeprazole. -a gastric proton pump inhibitor, on pentagastrin stimulated acid secretion in man. Gut, 1983;24:270- 76.
3. Lindberg,. P., Nordberg, P., Alminger, T., Brandstrom, A. and Wallmark, B. The mechanism of action of the gastric acid secretion inhibitor omeprazole. J.Med.Chem., 1986;29:1327-9.
4. Clissold, S.F. and Campoli-Richards, D.M. Omeprazole: a preliminary review of its pharmacodynamics and pharmakinetic properties and therapeutic potential in peptic ulcer disease and Zollinger-Ellison Syndrome. Drugs, 1986;3215-47.
5. Hendrix, T.R. and Yardley, J.H. Consequences of gastroesophageal reflux. Clin. Gastroenterol., 1976;5:155-74.
6. Johnson, LF. and DeMeester, T.R. Twenty-four hour pH monitoring of distal esophagus. Am.J. Gastroenterol., 1974;62:325.32.
7. DcMeester, T.R., Johnson, LF., Joseph, GJ., Toscano, M.S., Hall, A.W. and Skinner, D.B. Pattern of gastroesophageal reflux n health and disease. Ann.Surg., 1916;184:459
8. Dehn, T.C.B., Shepherd, HA, Cohn-Jones, D., Kettlewell, M.G.W. and Carroll, NJ. Double blind comparison of omeprazole (40mg od versus cimetidine 400 mgqid) in the treatment of symptomatic erosive reflux oesophagitis, assessed endoscopically, histologically and by 24 h pH monitoring. Gut, 1990;31:509-13.
9. Zeitoun, P., Rampat, P., Barbier, P., Isat, J.P., Eriksson, S. and Carlsson, R. Omeprazole (20mg daily) compared to ranitidine (150mg twice daily) in the treatment of esophagits caused by reflux: result of a double blind randomized multicenter trial in France and Belgium. Gastroenterol. Clin. Biol., 1989;13:457-62.
10. Havelund, T., Laursen, LS., Skoubo-Kristensen, E., Anderson, B.N., Pedersen. S.A., Jensen, K.B., Fenger, C., Hanberg-Sarensen, F. and Lauritsen, K. Omeprazol and ranitidine in treatment of refluxesophagitis; double blind comparative triaL Br.Med.J., 1988;296:89-92.
11. Klinkenberg-Knol., E.C., Jamsen, J.B., Festers, H.P., Meuwissen, S.G. and Lamers., C.B. Double-blind Multicentre comparison of omeprazole and ranitidine in the treatment of reflux esophagitis. Lancet., 1987;1:349-51.
12. Vantrappen, G., Ratgeerts, L., Scburmana, P. and Coenegrachis, J.L Omeprazole (40 mg) is superior to ranitidine in short-term treatment of ulcerative re0ux esophagitis. Dig.Dis.Sci., 1988;33:529.
13. Sandmark., S., Carisson, R., Fausa, 0. and Lundell, L Omeprazole or ranitidine in the treatment of retlux esophagitis. Results of a double-blind, randomized, Scandinavian multicenter study. Scand.J.Gastroenterol., 1988;23:625-31
14. Naesdal, 3., Bodemar, S. and Walan, A. Effect of omeprazole, a substituted benzimidazole, on 24-h intragastric acidity in patients with peptic ulcer disease. Scandi. Gaatroenterol., 1984;19:916-22.
15. Sharma, BK., Walt, R.P., Pounder, R.E., Gooses, M.D.. Wood, E.C. and Logan, LH. Optimal dose of oral omeprazole for maximal 24 hour decrease of incragastric acidity. Gut, 1984;25:957.64.
16. Walan, A. Clinical perspectives of drugs inhibiting acid secretion -H+ K+- ATPase inhibitors. Scand.J.Gastroenterol. (SuppL), 1986;125:50-54.
17. Dowoton, J., Dent, 3., Heddle, R. et al Elevation of gastric pH heals peptic esophagitis. J. Gastroenterol. Hepat.ol., 1987;2317-24.
18. Adams, M.H., Ostrosky, J.D. and Kirkwood, C.F. Therapeutic evaluation of omeprazole. Clin. Pharm., 1988;7:725-45.
19. Horowitz, M., Hetzel, DJ., Buckle, PJ., Chatterton, B.E. and Sbearman, D.J. The effect of omeprazole on gastric emptying in patients with duodenal ulcer disease. Br.J. Clin. Pharmacol., 1984;18:791-94.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: