
Chaudhry Aqeel Safdar ( Department of Paediatric Surgery, Military Hospital, Rawalpindi. )
MA. Hashmi ( Department of Paediatric Surgery, Military Hospital, Rawalpindi. )
December 1992, Volume 42, Issue 12
Original Article
ABSTRACT
Effect of antibiotic prophylaxis was studied in 400 children undergoing various types of surgery. Patients were divided into different classes according to the type of operation and each was further randomized into a routine or trial group. The routine group received antibiotics for prolonged periods. In the trial group, "clean" cases (class A) did not getany antibiotics. The “clean-contaminated” (class B) and "contaminated" cases (class C) received pen-operative antibiotics only. Frankly infected cases were not included in this trial. There were 131, 213 and 56 cases in classes A, B and C respectively; of these 13 (3.25%) cases were diagnosed as infected, four in the trial group and nine in the routine group. It was found that a short course of pen-operative antibiotics was equally, if not more effective. Prolonged courses of antibiotics were not only useless and expensive but could also be harmful. For clean cases there is no need for antibiotic prophylaxis. Children behave no differently and these results may be extrapolated to adults (JPMA 42: 286, 1992).
INTRODUCTION
The concept of prophylactic antibiotic therapy in surgical practice is the outcome of detection of organisms in clean wounds1-4. Although unnecessary5 but most clinicians continue to prescribe antibiotics prophylactically owing more to “dogmatic anecdote” than to informed evaluation6. Information about wound infections in children hospitals is scarce. Infection rate in children was low when they were included in adult series7. This study reports a randomized case control trial of antibiotics conducted in the department of paediatric surgery at Military Hospital, Rawalpindi.
PATIENTS AND METHODS
This randomized case control trial was based on the criteria laid down by Chodak and Plaut8. At the time of surgery, depending on the type of operation, the patients were ascribed to one of the surgical classes (Table I),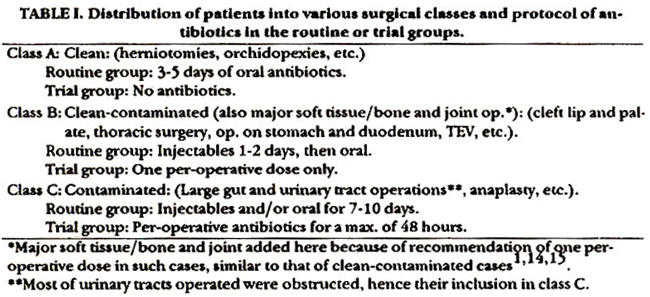
as described by Altemeier8. Consecutive patients admitted to surgical unit were randomized into routine or trial group. Every routine or emergency operation was included in the trial without any patient selection. Only cases already infected like abscesses and osteomyelits were excluded, as they needed therapy and not prophylaxis Neonates were excluded because of their impaired host-defence mechanisms and the necessity for relatively prolonged antibiotic prophylaxis10. A computer print Out of a structured proforma was attached to the patients notes. This proforma had three parts: first dealing with the patients’ particulars, second about the operative part and the third recording wound condition.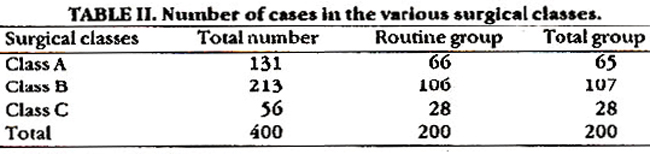
Besides this, other variables like duration of hospital stay, number on operation list, name of surgeon, type of skin closure and suture used and effect of drains (if any) was also recorded. Most of the operations were performed by one of the two authors. The details of surgical preparation was standardized and protocol for various surgical procedures worked out in advance. The antibiotics used were strictly as given in Table I. In the routine group ampicillin, gentamicin and metronidazole were used parenterally for 5-7 days (class B and C); in class A, ampicillin or erythromycin was administered orally for five days. All antibiotics in routine group were given post-operatively.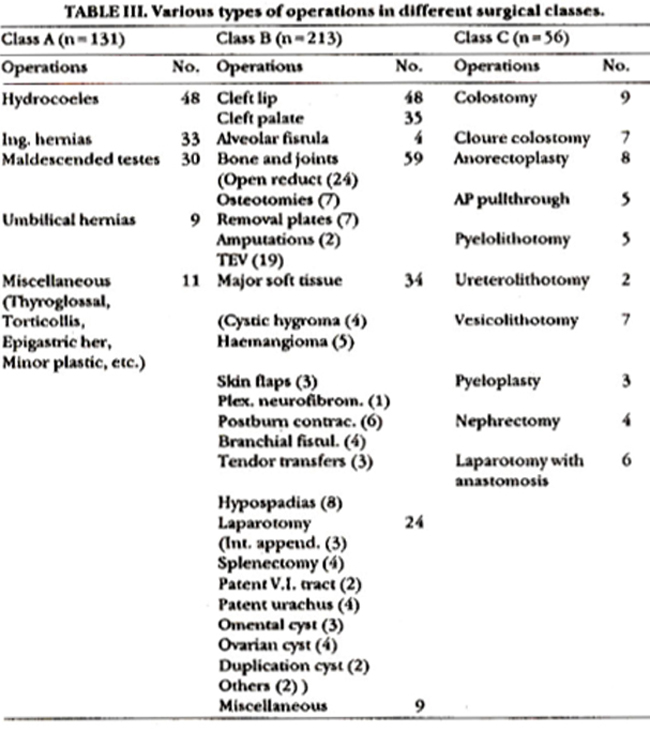
In the trial group, however, clean cases (class A) were not given any antibiotic; while parenteral antibiotics were used for the short periods in class B and C patients. They always received a pre-operative dose 15 to 30 minutes before the skin incision. The antibiotics selected were ampicillin and gentamicin in the standard doses, according to the patient’s weight. The main difference between the two groups being the duration and the timing of antibiotics. Metronidazole was added where indicated. All the wounds were inspected by one of us (C.A.S.) on day 3,5 and 10-14. A wound was considered infected if pus and/or abscess was present and swabs were taken for culture7. For statistical analysis t-test where applicable and x2 test were used.
RESULTS
A total of 400 cases were included in the study. Patients in each group were matched for numbers, age, sex and type of operation performed. The breakdown of the numbers and types of operations in various classes is shown in tables II and III. Wound infection occurred in 13 (3.25%) cases of which 4 belonged to the trial and nine to the routine group, the latter receiving prolonged antibiotics (Table IV).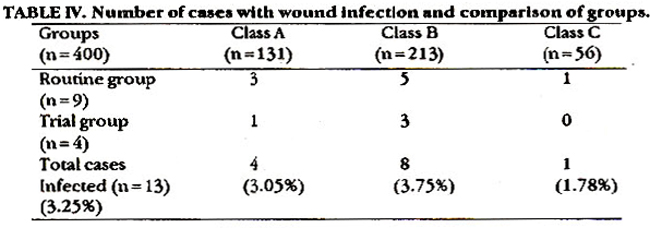
Other variables when analyzed showed no significant difference among the infected cases as regards their duration of hospital stay, number on the operation list, surgeon, types of sutures and closure and whether a drain was present or not (Table V).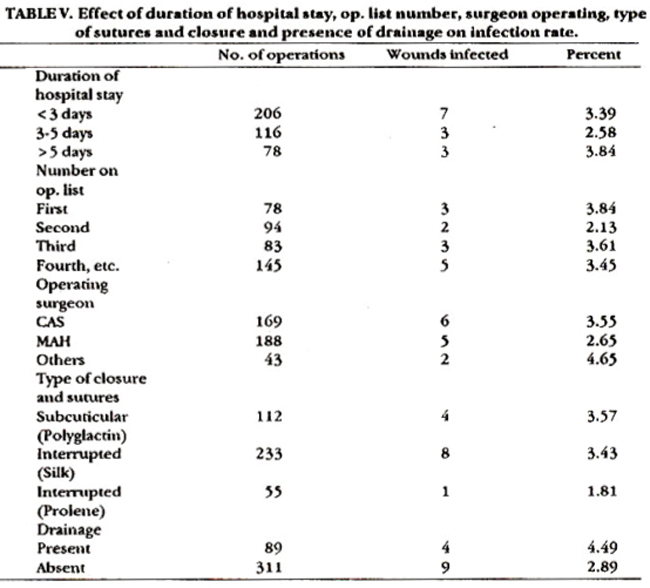
Six cases were excluded from the trial (four had chest infection and two large haematomas). The pus culture reports of 10 infected cases showed staphylococci in 8 cases (61.5%) and E. coli and haemophilus in one (7.7%) case each. Culture was not available in three (23%) cases.
DISCUSSION
The overall infection rate (3.25%) in this trial was much less than expected, in fact it was about half of that mentioned for another comparable group7,11. This low infection rate might have been due to the fact that neonates who tend to have higher infections due to various reasons7,12,13 were not included in this study. The reasons for prescribing of strong parenteral antibiotics in most of the hospitals in Pakistan, after any type of surgery are mostly due to primitive sterilization methods, inadequate hospital care, lack of cleanliness, malnourished patients, climate and dusty environment. Most of these reasons are anecdotal without any critical evidence. It was observed from this trial that infection rate in our setup is not as much as we presume. The principles of antibiotic prophylaxis advocated by authors from other parts of the world are equally applicable here. Their use is therefore unwise, dangerous and very expensive and purely based on conjecture. It is recommended that for clean class A patients no antibiotics should be used. For class B one pre-operative dose or at the most a second dose six hours after the operation is enough. Class C patients, who are potentially infected, may be given antibiotics for longer periods but beyond 48 hours they are unnecessary. When oven infection or faecal spillage is encountered at surgery, antibiotics are usually given for longer periods; this is not prophylaxis but treatment and the concepts should not be confused1. Every surgical unit should have their own controlled trials to assess the role of their own peculiar circumstances, before dismissing the results of this trial today’s climate of obsessive fervour for prophylactic antibiotics, it should not be forgotten that “no amount of antibiotic, however potent, can compensate for clumsy operating and hypoxic conditions” 14.
REFERENCES
1. Burke, J.F.The effective periodof preventive antibioticaction in experimentalincisions and derinsi lesions. Surgery, 1961;50161-68.
2. Alexander, J.W. and Altemeier, WA. Penicillin prophylaxis of experimental stapbylococcalwound infections. Surg. Gynecol., Obstet, 1965;120:243-54.
3. Shapiro, M., Shimon, D., Freund, U. and Sacks, T. A decisive period in antibiotic prophylsais of cutaneous lesions caused by bacteroides fragilis in guinea pigs. ).lnfect. Dis., 1980;141:532.
4. Bartiett, i.G. Experimental aspects of intra-abdominal sbacess. Am.J.Med., 1984;76(5A):91-98.
5. Finland, M. Antibacterial agents: uses and sbusesin treatment and prophylaxit. Rhode Island Med.J., 1960;43:490-504.
6. Eykyn, S.J. The prophylscticuse of antibiotics in surgery. Surgery, 1988;55:1304-7.
7. Doig. CJvLsnd Wilkinson, A.W. Wound infection in a childre&s hospital. Br.J. Surg,, 1976;63:647-30.
8. Chodak, G.W. and Plaut, M.E., Use of systemic antibiotic for prophylaxis in surgeryt a critical review. Arch. Surg., 1977;112:326-34,
9. Ahemeier, W. Control ofwound infection. J.R. Coll. Surg. Edinb., 1966;11:271-82.
10. PublicHealtb Laboratory Service. lncidenceofsurgicalwound infection in England and Wales. Lances, 1960;2:6S9-63.
11. Plueckhshn, V.D.The staphylococcus and the newborn child. Br.MedJ.. 1961;2:779-85.
12. Polakoff, S., Richards, ID., Parker, M.T., et al. Nasal sndskin carriageofstaphylococcus aureus bypstients undergoingsurgical operation. J.Hyg. (Csmb.), 1967;65:559-66.
13. Pollock, A.V. Surgical prophylaxis- theemerging picture. Lances, 1988;1:225-30.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: