
Ijaz Ahmad ( National Institute of Cardiovascular Diseases, Karachi. )
M. Ishaq ( National Institute of Cardiovascular Diseases, Karachi. )
December 1992, Volume 42, Issue 12
Original Article
ABSTRACT
The effect of intravenous streptokinase (SK) on time course of creatine kinase-MB (OK-MB) release and rapid reduction in ST- segment elevation as two non-invasive markers of reperfusion was prospectively studied in 83 patients with first anterior wall AMI (SK group, n = 61; control group, n =22). OK-MB evidence of reperfusion in the SK group was significantly higher than that in the control group (80% versus 32%; P 0.0001). The rapid resolution of sum of ST segment elevations as an evidence of reperfusion was found in 82% patients in SK group versus 23% in the control group (P 0.0001). Both GK-MB and rapid resolution of ST segment elevations as evidences of reperfusion were found in 69% patients in Sk and 14% in the control group (P 0.0001). The proportions of patients with non-invasive evidence of reperfusion with half-dose SK (750,000 units) regimen were comparable to that reported in the literature with full dose SK (1.5 million) regimen. Thus, serial CK-MB and EGG analysis in patients with AMI undergoing streptokinase therapy provides a non-invasive means for assessing therapeutic success. A dose of 750,000 units of 5K was found clinically satisfactory using previously validated non- invasive markers of coronary reperfusion and produced results previously reported with 1.5 million units of 5K (JPMA 42: 288, 1992).
INTRODUCTION
Thrombolytic therapy in acute myocardial infarction (AMI) has been shown to be effective in limiting infarct size, preserving left ventricular functions1 and reducing short and long term moratality2-4. Coronary angiography immediately after thrombolytic therapy is the most - accurate way to document coronary artery patency. However, only a few medical centres can provide timely angiographic evidence of reperfusion for each patient with AM!. Early relief of chest pain5, rapid reduction in ST segment elevation6-8. early peaking of serum creatine kinase9 and reperfusion arrhythmias10 are some of the markers used to predict reperfusion noninvasively. The present study was done to assess the usefulness of Papid resolution (reduction) of ST segment elevation and early peaking of CK-MB as noninvasive markers of myocarclial reperfusion in patients treated with intravenous streptokinase or conventional therapy and assess the relative efficacy of half-dose (750,000 units) of intravenous streptokinase in causing coronary reperfusion (detennined by above-mentioned non-invasive markers) as compared to the efficacy of full-dose (1.5 million units) of streptokinase (reported in the literature).
PATIENTS AND METHODS
Eighty-three patients with acute anterior wall myocardial infarction seen between May, 1990 and October, 1991 at National Institute of Cardiovascular Diseases, Karachi were included in the study. Sixty-one patients were given streptokinase (5K group) and twenty two patients (control group) were treated with conventional therapy. Inclusion criteria were ischemic chest pain of at least 30 minutes or more but less than 4 hours duration, ST segment elevation of at least 2 mm in two consecutive precordial leads, persistence of chest pain and ECG changes after sublingual nitroglycerin and age less than 60 years. Exclusion criteria were inferior and isolated high lateral wall M.I., age over 60 years, left bundle branch block, dilated cardiomyopathy and contraindication to streptokinase. A dose of 750,000 units streptokinase (streptase) diluted in 50 ml 5% D/W was given intravenously in 30 minutes. Concomitantly, a bolus of 5000 IU of heparin was infused followed by 24,000 IU per 24 hours. The dose was adjusted to keep the activated partial thromboplastin time 1.5 to 2 times the baseline. Heparin infusion was continued for at least five days except when patients bled. Disprin (150 mg) was given daily. Conventional anti-anginal and anti-congestive treatment was used as needed. Blood samples were obtained before the start of streptokinase infusion and sent to laboratory for baseline CK-MB and activated partial thromboplastin time (APTr). Thereafter blood samples were taken at 4 hour intervals for the first 24 hours for determination of CK-MB activity. For each patient, the time from streptokinase administration to peak CK-MB was noted. Electrocardiograms recorded before thrombolysis and 4 hours after start of streptokinase were analysed for resolution of ST segment elevations. The sum of ST segment elevations on the electrocardiograms recorded at admission and 4 hours after the start of treatment was calculated. The reduction in sum of ST segment elevations after thrombolytic treatment was expressed as a percentage reduction from the initial value of sum of ST elevations. Maximal CK-MB activity within 12 hours after the start of streptokinase therapy was considered a positive marker of infarct-related artery reperfusion9,12,13. A positive ST marker was defined as a reduction in sum of ST segment elevation of?: 50% within 4 hours after the start of thrombolysis6-8. The statistical analysis was performed using the Z-test for comparing the difference of two proportions. P< 0.05 was taken as statistically significant. In addition Student’s t test for independent samples was used for comparing the means of two groups.
RESULTS
The study included 83 patients, 22 in the control group and 61 in the streptokinase (SK) group. Clinical characteristics were smular between the two groups. There was a significant difference in time from streptokinase administration to peak CK- MB, between the control and streptokinase groups. This difference resulted in a higher proportions of patients in the streptokinase group having enzymatic evidence of reperfusion (80% versus 32%, P <0.0001) (Table I).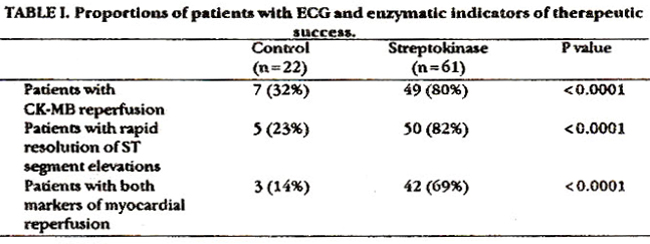
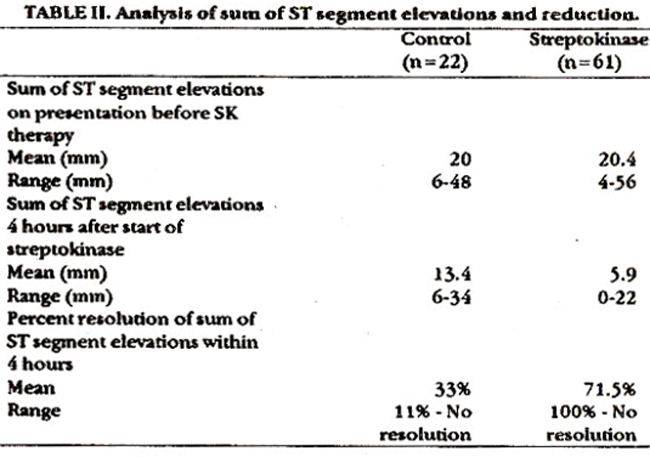
As shown in Table II there was no significant difference in the mean sum of ST-segment elevations (in mm) at presentation between the SK and control groups 120.4 (4-56)) versus [20 (6-48)]. However, there was marked difference in the mean sum of ST segment elevations (in mm) at 4 hours from initiation of streptokinase between SK and control groups [5.9 (0-22)] versus [13.4 (6-34)]. Similarly the mean percent resolution of the sum of ST segment elevations at 4 hours was also markedly different in SK and control groups [7 1.5% (100%-No resolution)) versus [33% (11%-No resolution)). These differences resulted in a much higher proportion of patients in the streptokinase group having?: 50% reduction in the sum of ST segment elevations at 4 hours from the initiation of streptokinase as compared to initial sum as an indicator of reperfusion (i.e., therapeutic success) (82% versus 23%, P <0.0001). The combined analysis of two markers of reperfusion also revealed highly significant between SK group and P<0.0001) (Table I).
DISCUSSION
Results of the present study suggest the ability of non-invasive methods to identify patients who benefit from thrombolysis for AMI and to predict reperfusion status to a clinically useful degree. The study describes the assessment of myocardial reperfusion by two non-invasive methods (early peak of CK-MB and rapid resolution of sum of ST segment elevations). Considering CK-MB peak, a cut off value of 12 h after the start of thrombolysis was derived from a trial conducted by Meinertz et al12. In a recent study, Hohnloser et al9 used the same cut off value as a non-invasive marker of coronary artery patency and revealed a sensitivity of 84% and a specificity of 95%. Gottlich et al13 used following criteria for CK-MB determined reperfusion: time from onset of chest pain to peak CK < 17 hours and time from SK to peak CK< 15 hours. In their study, CK-evidence of reperfusion was found in 75% patients given 500,000 units SK, 89% given 750,000 units SK and 67% given 1.5 million units SK. The present study documents the usefulness of the standard ECG ST segment as a non-invasive predictor of coronary artery reperfusion after intravenous SK for AML In the present study, _ 50% reduction in sum of ST segment elevations at 4 hours after SK was used as an indicator of reperfusion; 82% patients fulfilled this criteria versus 23% control group, (P<0.0001). These findings are consistent with many recent studies. Hogg et at6 reported a high sensitivity (93%) for a fall of _ 50% in the lead showing maximum ST elevation, with a specificity of 67%. Workers evaluated whether angiographically determined reperfusion could be predicted from changes in ST segment elevation8,14. According to Saran et at8 reduction in ST elevation of >25% within 3 hours of thrombolysis indicates either a patent infarct artery or preservation of left ventricular function. When the ST segment elevation does not fall by >25% persistent coronary occlusion is likely (predictive accuracy 86%). Clemmensen et al14 compared the sum of ST segment elevation before and after (<8 hours, pre-angiographic from onset of symptoms) thrombolytic therapy and concluded that a decrease of only 20% in the sum of ST elevation in the standard ECG after thrombolytic therapy is a useful non-invasive predictor of reperfusion status in patients with evolving AMI. In a recent study, Hohnloser et at9 defined _ 50% reduction in ST segment elevation as a positive non- invasive marker of coronary reperfusion and found a value of 60% sensitivity, 95% specificity and 97% positive and 42% negative predictive value regarding prediction of coronary artery patency. The half dose (750,000 units) regimen of streptokinase therapy used in the present study is supported by another study13, where it was concluded that if sufficient streptokinase is given to produce a systemic fibrinolytic state, smaller doses (500,000 and 750,000 units) are as effective as larger ones (1.5 million units) in inducing coronary reperfusion. This is a small pilot trial done in local patients, using previously validated non-invasive markers of coronary reperfusion against the gold standard of coronary angiography. Patients were not randomized with standard and half dose SK regimens. Before the half dose SK regimen can be recommended on routine basis, large randomized trials comparing the standard and half dose groups mortality would be required.
ACKNOWLEDGEMENTS
We thank the house staff, nurses, technicians and attending physicians at National Institute of Cardiovascular Diseases for their dedicated assistance during this study.
REFERENCES
1. Simoona. M.L., Serruys, P.W., van den Brand, M. et al. Early thrombolysia in acute myocardial infarction, limitation of infarct aize and improved survival. J.Am.Coll.Cardiol., 1986;7:717.
2. Gruppo Italiano per lo studio deJa streptotinaae nell infarto miocardico (GISSI). Effectiveness of intravenous thorombolytic treatment in acute myocsrdial infarction. Lancet, 1986; 1:397-401.
3. Gruppo Italiano per Jo Studio della Streptokinase nell infarto miocardico (GISSI): Effectiveness of intravenous thrombolysis in acute myocardial infarction: final report of the GISSI study. Lancet, 1987;2871.
4. ISIS-2 (Second International Study of Infarct survival) Collaborative Group: Randomized trial of intravenous streptokinase, oral aspirin, both, or neither among 17187 cases of suspected acute myocardial infarction: ISIS-2 Lancer, 1988;2:349-60.
5. Kricher, B.J., Topol., EJ., O’Neil, W.W. and Pitt, B. Prediction ofinfaretcoronaryartery recanalization afterintravenous thrombolytic therapy. Am.J.Cardiol., 1987;59.513-15.
6. Hogg, K.J., Hornung, R.S., Howie, CA., Hockings, N., Dunn, F.G. and Hillis, W.S. Electrocardiographic prediction of coronary artery patency after thrombolytic treatment in acute myocardial infarction: use of the ST segment as a non-invasive marker. Br.Heart.J., 1988;60.275-80.
7. Barbash, G.l., Roth, A., Hod, H., Miller, H.I., Roth, S., Hsr- Zshsv, Y., Msdsn, M., Seligsohn, U., Battler.A., Ksplinsky, B., Rabinowitz,B. and Laniado, S., Rapidresolution of ST elevstion and prediction of clinical outcome in patients undergoing thrombolysis with alteplase (n-PA): results of lsrseli study of early intervention in myocsrdisl infarction. Br.Heart.J., 199064:241-47.
8. Saran, R.K., Been, M., Furniss, 5.5,, Hawkins, t and Reid, U.S. Reduction in ST segment elevation after thrombolysis predicts either coronary reperfusion or presentation of left ventricular function. Br. Heart.J., 1990; 64:113-17.
9. Hohnloser. S.H., Zabel. M., Kasper, W. et al Assessment of coronary srtery patency after thrombolytic therspy: accurate prediction utilizing the combined snslysis of three non-invasive markers, J.Am.ColL Cardiol., 1991;18:44-49.
10. Goldberg, S., Greenspon, AJ., Urban, P.L, Muza, B., Berger, B., Walinsky, P. and Msroko, P.R. Reperfusionsrrhythmis; smarkerofrestorationofsntegrsdeflowduring intracoronsty thrombolysis for acute myocardial infarction. Am.Heart J., 1983;105:26-32.
11. Clemmensen, P., Grande, P., Pedersen, F. et sL ECU and enzymstic indicators of therapeutic success after intravenous streptokinase for scute myocardial infsrction. Am.Heart.J., 1990;120:503-9.
12. Meinertz,T., Kasper, W., Schumacher, M. sod Just, H.The Germsn multicenter trial of anisoylsted plasminogen streptokinase activstor complex versus heparin for acute myocardial infarction. Anti. CardioL 1988;62:347-5 1.
13. Gottlich, CM., Cooper, B., Schumacher, 3.lt and Hills, U. Do different doses of intravenous streptokinase affect the frequency of coronsry reperfusion in acute myocardial infsrction?AmJ. CsrdioL, 1988;62:843-46.
14. Clemmensen, P., Ohmsn, EM., Sevills, D.C. et sL Chsnges in standard electrocsrdiographic ST-segment elevation predictive of successful reperfusion in acute myocardial infarction. Am.J. Cardiol., 1990,66:1407-11.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: