
Parveen Haider ( Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. )
Sadiqua N. Jafarey ( Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. )
November 1992, Volume 42, Issue 11
Original Article
INTRODUCTION
Endometrial tuberculosis is an uncommon but an important clinical entity1-4. Although it is becoming increasingly rare in the developed world5-7, endometrial tuberculosis still continues to be an important medical problem in Pakistan and its exclusion is necessary in the investigation of Infertile women. In our department it has not been a standard practice to subject the endometrium to routine culture for mycobacteria in cases of infertility purely for economic reasons. Histological evidence was considered to be adequate for diagnosis and initiation of chemotherapy2,5,6,8, but during the last two years it has been observed that in two cases where endometrium was cultured, a growth was obtained although the histology was found to be negative. This prompted us to undertake the present study where the endometrium of infertile women was studied both histologically and bacteriologically.
PATIENTS, METHODS AND RESULTS
From January, 1990 to August, 1990, 142 infertile women were investigated for endometnal tuberculosis in the Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. A careful enquiry was made about any present or past evidence of tuberculosis. Investigations included complete blood picture, ESR, Mantoux test and x-rays of the chest and abdomen for any evidence of extragenital tubercular lesion. Semen analysis was done to rule out male factor as being the possible cause. Ultrasound of pelvis was performed in selected cases where some pathology was suspected on pelvic examination. A premenstrual diagnostic curettage was done in all cases and the endometrium was examined both histologically and subjected to bacterial culture. The ages of the patients ranged from 17 to 38 years (mean age 27 years) and the duration of infertility varied between 1.5 to 20 years (mean 5.5 years). There were 104 (73.2%) cases of primary and 38 (26.8%) of secondary infertility. There were 38 viable deliveries and 14 abortions. Puerperium was uneventful in all. Fifteen (10.5%) patients had a past history of extrapelvic tuberculosis; of these 10 had pulmonary and 3 abdominal tuberculosis. Two cases had tuberculous cervical lymphadenitis. Ten cases gave a history of receiving anti-tuberculous treatment in the past. In one case laparotomy was performed at the age of 18 years and tuberculosis was confirmed on histopathology. She had been given a course of chemotherapy for 12 months following surgery. Complete blood picture did not reveal any characteristic picture. ESR was elevated in 84 (59%) cases; of these 75 had values between 20-39 mm in the first hour (Westergren) and9 had a value of 40 and above. Mantoux test was negative in 40 cases and positive in the rest. Seventy-eight (55%) patients had a positive Mantoux test of 7 mm and above, 28 (19.7%) had 15 mm and above. X-ray chest was suggestive of past tuberculous involvement of lungs in 32 cases (22.5%) in the form of calcified nodes. One patient had calcified node on x-ray abdomen. Ultrasound examination of pelvis was performed in 30 (21%) cases. Adnexal masses were detected in 5 and fibroids in 2 cases. Of these 2 had ovarian cysts and underwent laparotomy later; none of these bad findings suggestive of pelvic tuberculosis as described by others9,10. Hysterosalpingograms were available in 17 cases (12%) and all were normal with no evidence of tuberculosis. Endometrium was subjected to histopathology in 18 cases because the curettings were scanty. No curettings were obtained in 8 and in one of these endometrial aspirate was cultured for mycobacteria. In two cases there was failure to dilate the cervical Os. On histopathological examination (n= 132) chronic granulomatous inflammation compatible with tuberculosis was found in 4 cases. Bacterial culture (n= 115) revealed a growth of mycobacterium tuberculosis in one case only. The clinical data of cases with tuberculous endometritis summarised in Table.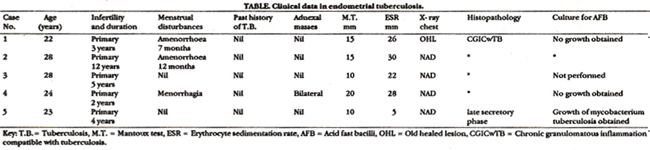
All cases had primary infertility. A change in menstrual pattern was seen in 3, two presenting with associated amenorrhoea and one with menorrhagia. In none was the past history suggestive, however one patient bad old healed lesion on x-ray chest. The frequency of endometrial tuberculosis as determined in the present study is 3.5% of all cases of infertility investigated, 1.2% of all D and Cs done in the department and 0.7% of all gynaecological admissions.
COMMENTS
Tuberculous endometritis has been detected in 3.5% of all our cases undergoing curettage for infertility and accounts for 0.7% of all gynaecological admissions. These figures are high than those reported from developed countries5-7. Nevertheless, the prevalence is consistent with the reports from the developing countries where it still continues to be an important problem in infertility clinics1,3,4,11. Although haematologic studies, Mantoux test, roentgenographic - examinations12, hysterosalpingography5,6, cytology13, ultrasonography9,10 and laparoscopy12 can be useful aids in the detection of tuberculosis, the eventual diagnosis depends upon the characteristic histopathological picture and is confirmed by bacterial culture. Four cases in the present study had a positive histopathological appearance of chronic granulomatous inflammation compatible with tuberculosis, but no growth was obtained on culture for mycobacteria in 3 cases while the fourth case had scanty curettings which were not subjected to bacterial examination. Curettage was not repeated on account of the risk of a flare up2. The patient who had a growth on culture, had a completely normal appearance of secretory endometrium on histology. In the cases investigated no histopatbological and bacteriological correlation was noted. This can be attributed to the focal nature of the lesion, small quantity of innoculum and slow growth of mycobacteria. Moreover, curettage may not have been performed during the period when granulomas are best developed. Although our sample size is small, the absence of correlation between the two tests emphasizes the need for subjecting the endometrium of infertile women ideally to both histopathological examination and bacterial cultures for mycobacterium tuberculosis. Histopathology alone will pick up the large majority of the cases but occasional ones may be missed if culture is not done.
ACKNOWLEDGEMENTS
Our deep gratitude to Dr. Iqbal of The Laboratory for performing complimentary bacterial cultures and to Dr. Qamar Jamal of Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi for her help with the histopathology results.
REFERENCES
1. Malik, G.B., Maheshwari, B. and Lal, N. Tuberculous endometritis. A clinicopathological studyof 1,000 cases. BrJ. Obstet. GynaecoL, 1983;90:84-86.
2. Sutherland, A.M. Tuberculosis of female genital traCL Tubercle., 1985;66:79-83.
3. Tripathy, S.N. and Tripathy, S.N. Endometrial tuberculosis. 3. Indian Med. Assoc., 1987;85:136-40.
4. D\\\'Costs, G.F. and Nagle, S.B. Tuberculous endometritis. A histopathological study. 3. Postgrad. Med., 1988;34:7-11.
5. Klein, T.A., Richmond, J.A and Mishell, D.R. Jr. Pelvic tuberculosis. Obstet. GynaecoL, 1976;48:99-104.
6. Punnonen, R., Kbilholma, P. and Meurman, N.L. Female genital tuberculosis and consequent infertility. Int.J.Fertil., 1983;28:235.38.
7. Falk, V., Luviksson, K. and Agren, G. Genital tuberculosis in women. Am.J.Obstet. Gynaecol., 1980;138:974-77.
8. Hutchins, C.J. Tuberculosis of the female genital tract. A changin picture. Br.J.Obstet. GynaecoL,1977;84:534-38.
9. Walzer, A. and Koenigsherg. M. Ultrasonographic demonstration of pelvic tuberculosis. 3. Ultrasound. Med., 1983;2:139-40.
10. Lee, J., Warner, L and Khaleghian, N.R. Sonographic features of tuberculosis endometritis. J.Clin. Ultrasound, 1983;11:331-33.
11. Tripathy, S.N. and Tripathy, S.N. Genital manifestations of pulmonary tuberculosis. Int.J. Gynaecol. Obstet., 1981;19:319-26.
12. Zummo, B.P., Sered, H. and Falls, F.H. The diagnosis and prognosis of female genital tuberculosis. Am.J.Obstet. Gynecol., 1955;70:34-43.
13. Khilnani, P.H., Pandit, A.A. and Krishna, U.R. Cytology as an aid in the diagnosis of genital tuberculosis.). Postgrad. Med., 1988;34:100-102.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: