
J.E. Ahaneku ( Department of Pathology, college of Health Science, Nnamdi Azikiwe University, Nnewi Campus, Anambra State, Nigeria. )
G.O. Taylor ( Departments of Chemical Pathology, College of Medicine, University of Ibadan, Ibadan, Nigeria. )
I.O. Olubuyide ( Department of Pathology, college of Health Science, Nnamdi Azikiwe University, Nnewi Campus, Anambra State, Nigeria. )
E.O. Agbedana ( Departments of Medicine, College of Medicine, University of Ibadan, Ibadan, Nigeria. )
November 1992, Volume 42, Issue 11
Original Article
ABNORMAL LIPID AND LIPOPROTEIN PATTERNS IN LIVER CIRRHOSIS WITH AND WITHOUT HEPATOCELLUIAR CARCINOMA
ABSTRACT
Plasma lipid and lipoprotein profile was determined in 12 cirrhotics, 15 patients with cirrhosis and hepatocellular carcinoma (HOC) and 20 healthy volunteers. When compared with controls plasma total cholesterol (IC), high density lipoprotein cholesterol (HDLC), high density lipoprotein phospholipids (HDLPL), HDLPL/PL levels were low, phospholipid (PL) was normal and HDLC/TC and PLJTC wero high in cirrhosis. In cirrhotics with HOC, TO, PL, PL/TC levels were elevated while HDLC, HDPL, HDLC/TC and HDLPL/PL were normal. A comparison within the patient groups showed that in cirrhosis alone, the levels of TO, HDLO, PL, HDLPL and HDLPLJPL were lower and PL/TC level was higher than in cirrhotics with HOC. Plasma albumin levels showed a negative correlation with PLJTO and a positive correlation with HDL-cholesterol in cirrhosis. In cirrhosis with HOC plasma, phospholipid levels showed a significant negative correlation with total bilirubin and alanine amino transferase. The variations in the level of plasma lipids and lipoproteins may assist in describing the nature of these two forms of liver disease (JPMA 42: 260, 1992).
INTRODUCTION
Plasma lipid levels vary with the stage of liver disease and associated complications. Plasma cholesterol levels are high in hepatocellular carcinoma (HCC) and low in cirrhosis1-3. Low cholesterol levels in cirrhotics and insignificant changes in HCC reported by Taylor and Bamgboye4 were contrary to the findings of Ayoola5 in the same community and Alpert et al6 in Ugandans. The present study is a comprehensive investigation of plasma lipids and high density lipoprotein patterns and their correlation with other liver function tests in cirrhotics with or without HCC.
PATIENTS AND METHODS
Twenty-seven patients (15 males and 12 females) aged 39-86 years with liver disease were studied at the liver unit of University College Hospital, Ibadan, Nigeria. Twelve patients had cirrhosis and 15 cirrhosis with HCC. Diagnosis was based on clinical features (icterus, ascites, hepatomegaly or decreased liver size) and histological findings at liver biopsy. Patients with HCC were not on any cytotoxic drugs at the time of study. Twenty healthy volunteers (11 males, 9 females) served as controls. Patients and control subjects were of the same socioeconomic status. After an overnight fast, venous blood samples were taken from the controls and the patients in bottles containing dry Na2 EDTA for lipids and lithium and heparin for liver function tests.
Biochemical determinations
High density lipoprotein (HDL) was isolated from the other lipoproteins by a modification of the method described by Burstein and Samaille7. The supernatant containing HDL was removed by pipetting and stored with the remaining plasma at -20°C until analysed. HDL phospholipids (HDLPL) and plasma total phospholipids (PL) were determined by the method described by King and Wootton8. HDL cholesterol in the supernatant and the plasma total cholesterol were also determined by the modified Liebermann Burchard reaction as described by Searcy and Berquise9. Other biochemical tests included alkaline phosphatase10, alanine aminotransferase (ALT) 11, total bilirubin12, total protein and albumin by the Biuret and Bromocresol method, respectively. For each assay, a commercial quality control (Wellcome reagents) and a pooled plasma control of known values were always included. Results were acceptable only when determined values were within the specified values.
Histological investigations
Histological diagnosis was based on the criteria described by Scheuer13.
Statistical methods
Analysis of variance (ANOVA) and the student’s t-test were used to compare paired values and the differences with a P <0.05 regarded as significant. Pearson perfect correlation coefficient was used to assess the strength of association between lipid levels and liver function tests.
RESULTS
The mean ages in both controls and patients with cirrhosis alone were similar but significantly lower than those with cirrhosis and 11CC (P <0.001). The mean body weights were similar in cirrhosis alone and cirrhosis with HCC but significantly lower than the corresponding control values (P< 0.001). liver function tests In cirrhosis alone, plasma total proteins, albumin and alanine aminotransferase (ALT) were significantly reduced when compared with the controls (Table I).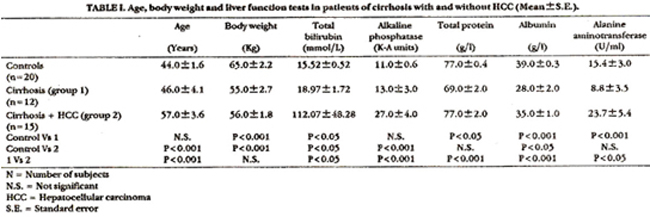
Total bilirubin concentration was significantly increased (P<0.05) while the difference in ALP was not significant. In cirrhosis with HCC the albumin vulue showed a significant reduction (p<0.05) while the slight increases in total protein and ALT levels were not significant when compared with the corresponding control values. Total bilirubin and ALP levels were significantly elevated (P<0.05; P<0.001 respectively). Mean total protein, albumin, total bilirubin, ALP and ALT levels in cirrhosis with HCC were significantly higher than the corresponding values in the patients suffering from cirrhosis alone (Table I). The variations in the mean values of the liver function tests of the different groups were also found to be significant using one way ANOVA (P<0.05).
Table II shows the plasma lipid and lipoprotein concentration in different groups. A multiple comparison using one way ANOVA showed that the variations in the mean values of different groups (control 1 and 2) were significant. In cirrhosis alone, total cholesterol and HDL cholesterol values were significantly reduced when compared with the corresponding control values. However, there was a significant increase in the ratio HDLC/TC. In cirrhosis with HCC, the TC was significantly increased while HDLC and HDLC/TC ratio were not significantly different from the control values. Statistical comparisons also showed that the TC and HDLC in cirrhosis with HCC were significantly higher than the corresponding levels in cirrhosis alone, while the slight difference in HDLC/TC was not significant. The mean values of PL, HDLPL and the ratio HDLPL/PL in cirrhosis alone were low when compared with the corresponding control values but the reduction in PL was not statistically significant. The ratio PL/TC in cirrhosis alone showed a significant increase (P<0.05) (Table II). In cirrhosis with HCC, PL and PL/TC ratio were significantly elevated while the changes in HDLPL and HDLPL/PL ratio were not significant when compared with the corresponding control values. Mean values of PL, HDLPL and ratio HDLPL/PL were significantly increased in cirrhosis with HCC when compared with the corresponding values in cirrhosis alone. However, the increase in the ratio PL/TC was higher in cirrhosis alone (P<0.05). In all groups, there were no significant correlations between age and any of the lipid parameters.
Correlation between liver function tests and plasma lipid and lipoprotein
Alkaline phosphatase was positively correlated with the ratio HDLC/TC (r=0.527; P<0.05) ad negatively correlated with the PL level (r=0.492; P<0.05) only in the control group. The plasma albumin showed a significant negative correlation with PL/TC (r=0.574; P<0.05) in cirrhosis, a negative correlation with HDLC in control (r=-0.472 P<0.05) and a positive correlation n cirrhosis (r=0.784; P<0.001). Alanine amino transferase (ALT) was positively correlated with TC (r = 0.635; P<0.001) and PL (r = 0.503; Pc 0.05); but negatively correlated with HDLC/TC (r = 0.567; P<0.001) and HDLPL/PL (r = -0.512; P<0.05) ratios in control subjects. Total protein showed a significant negative correlation with PL (r = 0.556; Pc 0.05) in cirrhosis with HCC and phospholipid was correlated positively with total bilirubin (r = 0.743; Pc0.001) and ALT (r = 0.548; P<0.05) in cirrhosis alone.
DISCUSSION
The observed biochemical abnormality of liver function tests in cirrhosis and in cirrhosis with HCC are well known. The elevated values of ALP observed in cirrhosis with PLCC in this study is a recognised finding14. Biochemical changes in cirrhosis are different from those in cirrhosis with 11CC; in the former, ALP value was within the normal range. Reduced levels of albumin, total protein and alanine aminotransferase (ALT) in cirrhosis when compared with the levels in cirrhosis with HCC could be related to the advanced stage of hepatocellular damage in cirrhosis. The increase in the mean total cholesterol in cirrhosis with HCC have been related to a malignant obstructive lesion of the biliary tree. The loss of negative feedback mechanism for cholesterol regulation15 as well as an increase in cholesterol synthesis by undifferentiated hepatocellular carcinoma cells16 may be responsible for the hypercholesterolemia in cirrhosis with HCC. HDL-cholesterol and HDL cholesterol/total cholesterol levels in cirrhosis with PLCC were not significantly different from the control values. These observations are in disagreement with the decreased HDL-cholesterol reported by Haechem et al17. In cirrhosis alone, total cholesterol and HDL-cholesterol values were reduced and this may be due to cellular necrosis in cirrhosis18. A positive correlation observed between albumin and HDL-cholesterol in cirrhosis further confirms the above suggestion. However, the ratio HDL-cholesterol/total cholesterol was increased in cirrhosis when compared with the control value, but did not show any significant variation when compared with the level in cirrhosis with HCC. This could suggest that the ratio HDL cholesterol/total cholesterol was maintained in cirrhosis with or without 11CC. The observed changes in phospholipid level in these two diseases are of much interest. Phospholipid level showed an increase in cirrhosis with HCC, while the levels of HDL-phospholipid (HDLPL) and HDL phospholipid/phospholipid (HDLPL/PL) were normal when compared with the control values. The increase in phospholipid may be due to a malignant obstructive lesion of the biliary tree as has also been suggested above for the changes in cholesterol level in cirrhosis with 11CC. Total phospholipid level in cirrhosis alone was not significantly different from the values for the control. This was not expected in a disease associated with extensive hepatocellular damage; thus this observation is contrary to the findings of a reduced phospholipid level in cirrhosis19-21. However, HDL- phospholipid level was reduced in cirrhosis and therefore the ratio HDL phospholipid/phospholipid (HDLP/PL) was also reduced when compared with the control values. A comparison within the patient groups also showed that phospholipid levels were reduced in cirrhosis alone when compared with the corresponding levels in cirrhosis with HCC. The ratio PL/TC was Increased in cirrhosis alone when compared with the values in cirrhosis with 11CC and the control. A negative correlation between albumin and PL/TC in cirrhosis further confirms this observation. It is evident that there are differences in lipid profiles between cirrhosis and cirrhosis with 11CC and this could relate to the extent of liver damage in these conditions. Although the patients with cirrhosis were on the average slightly younger than those with cirrhosis plus 11CC, the age difference could not explain the differences in lipid profiles observed in two groups as the results showed no significant correlation between age and any of the lipid parameters in different groups. Similarly there is no sex bias in our observations as we observed no sex-related differences in lipid profiles in the different groups. This study clearly defines the lipid and lipoprotein profiles in our community and emphasises the importance of deranged liver function in lipoprotein metabolism in liver diseases.
REFERENCES
1. Santer, M.A. Jr., Waldmann, T.A. and Fallon, H). Erythrocytoaia and hyperlipiderniaas manifestations of bepatic carcinoma. Arch. Intern. Med., 1967;120:735-39.
2. Viallet, A., Senhamore, J.P. and Fauvet, it Primary carcinoma of the liver and hyperlipidemia. Can. Med. Asaoc. J., 1982;86:1118-22.
3. Ellefson, R.E. and Caraway, W.T. Lipids and lipoprotcin, in fundamentala of clinical chetniatry. Edited by Norbert W. Tieta. Philadelphia, Saunders, 1976 pp.474-541.
4. Taylor, 0.0. and Bamgboye, A.E. Serum cholesterol and diseases in Nigerians. Am). Clin. Nutr., 1979;32:2540-45.
5. Ayoola, E.A. Paraneoplastic syndrome in primary liver cell carcinoma. Experience in Ibadan, Nigeria. Afr.J.Med. SaL 1980;9:163-67.
6. Alpert. M.E., Hutr, M.S.R., Wogan, G.N. and Davidson, CS. Association between aflatoxin contentof food and hepatoma frequency in Uganda. Cancer, 1971;28:253-60.
7. Burstein and Samaille. A rapid determination of the cholesterol bound to the serum (2 sndfl lipoproteins. Clin. Chim. Acta, 1960;5:609.
8. king, E.J. and Wootton, LOP. Microsnalysisin medical biochemistry. 3rded. New York, Grune andStratton, 1956.
9. Searcy, ILL. and Berquist, L.M. A new colour reaction for the quanritation of serum cholesterol. Clin. Cbim. Acta, 1960;5:192- 99.
10. king, E.J. and Armstrong, A.R. A convenient method for determining serum and bile phoaphatsse activity. Can.Med.Assoc.J., 1934;31:376.
11. Dade Biagnosticloc. Aguds PuertoRico. Aspartateaminotransferaae (AST:GOT) and alanine aminotrsnsferase (ALT, OF’!) reagents for the quantitative determination of AS’!’ and ALT in human serum or plasma (modified Reitman-Frankel method). 1983;11:1-4.
12. Malloy, H.T. and Evelyn, LA. Determination çsf bilirubin with photoelectrIc colorimeter. J. Biol. Chem., 1937;119:481-90.
13. Scheuer, P.J. Liver biopsy interpretation. 2nd ed. London, BailliereTindali, 1973.
14. Curutcher, H.P., Terz, J.J., Kay, S. and Lawrence, W. Primary liver cancer. Surgery, 1971;70:467-79.
15. Siperstein, M.D. and Fagan, V.M. Detection of the cholesterol- negative feedback system in liver tumoura. Cancer Ret, 1967;24:1108-15.
16. Siperstein, M.D. Regulation of cholesterol synthesis in normal and malignant tissue Curr.Top.Cell.Regul., 1970;2:65.
17. Hachem, H., Rayal, 0.F.G., Blary, 0. et aL Serum apolipoproteins. A-I and in hepazic metastasis comparison with other liver diseases hepatoms and cirrhosis. J. Gin. Chem. Clin. Riochem., 1986;24:161-66.
18. Luoma, P.V., Sotaniemi, ES., Peltonen, 0.0. and Savolainen, M.J. Induction and lipoproteins (letter). Lancet, 1982;1;625.
19. Rehmsn, A., Zuberi, S.J. and Hasnain, S.N. Lipid pattern in liver disease. 3.Pak. Med. Assoc., 1982;32:275-78
20. Phillips, G.B. The lipid composition of serum in patientswith liverdisease.J. Clin. Invest., 1960;39:1639-50.
25. McIntryre, N.Plssms lipidsand lipoproteinsin liverdisesse. Out, 1978;19:528-30.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: