
Ijaz Ahmad ( Department of Surgery, K.E. Medical College, Lahore. )
October 1992, Volume 42, Issue 10
Original Article
ABSTRACT
Non-specific reactive hyperplasia (NSRH) accounted for 20% patients of cervical lymphadenopathy collected over a period of 1-1/2 years. The disease affected comparatively younger people of both sexes equally. Routine investigations offered little diagnostic help. The disease resolved spontaneously in 1/3rd of patients, 1/4th developed specific entities, while in the rest it continued as a prolongedailment. Lymph node biopsy should be planned meticulously to avoid missed diagnosis. If the lymphadenopathy of NSRH does not subside spontaneously within two months, a re-biopsy is advised to pick up a specific ailment (JPMA: 237, 1992).
INTRODUCTION
Every clinician frequently encounters biopsy report as “non- specific reactive hyperplasia" while investigating a patient with cervical lymphadenopathy. He takes it a frustrating blind end of the therapy and may start antibiotics empirically to “offer something to the patient”. Such patients usually have a prolonged morbidity and move from one doctor to another without much avail. In this article a follow-up of patients of non-specific reactive hyperplasia is presented in an attempt to know the fate of this perplexing problem.
PATIENTS AND METHODS
One hundred patients of cervical lymphadenopathy were collected over a period of 1-1/2 year between January 1st, 1990 andJune30th, 1991 in the East Surgical Unit, Mayo Hospital, Lahore. Patients presenting as a part of systemi or focal disease were excluded. Their aetiological distribution is given in Table I.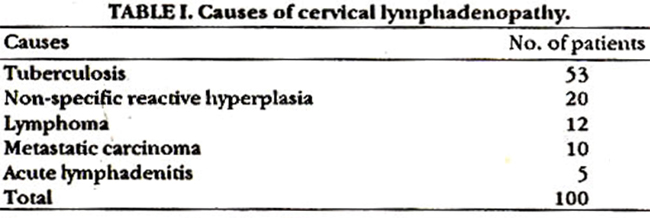
Out of these tuberculosis, lymphoma, metastatic carcinoma and acute lymphadenitis represent well recognised entities with established line of management. Non-specific reactive hyperplasia represents an ill-understood entity without standardised line of management. Their evaluation is presented further. The age range for these 20 patients (11 males, 9 females) was between 10 and 50 years (mean 23 years). Maximum number of patients seen were between 15 and 25 years. Children below 10 years were not encountered because they were admitted to paediatric surgical unit directly. Frequency of various signs and symptoms is given in Table II.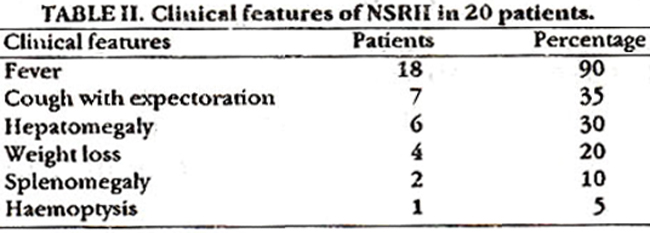
Apart from lymph node enlargement, fever was the predominant symptom followed by cough with expectoration, hepatomegaly and splenomegaly. A few patients complained of deterioration of health, easy fätiguability and sense of malaise. The total leucocyte count was elevated in 3 patients, normal in 14 and low in 3 patients. The differential leucocyte count was within normal range in all patients. Haemoglobin was less than 10G% in 5 and more in the remaining 15 patients. ESR was raised above 50 mm/1st hour in 8 patients and normal in the rest. Lung parenchymal shadows on X-ray were normal in all patients. Mantoux test was positive in 3 patients and negative in the rest. Fifteen patients had involvement of superficial cervical and three patients deep cervical group. Two patients had involvement of both groups. Some patients had enlargement of other lymph nodes as shown in Table III.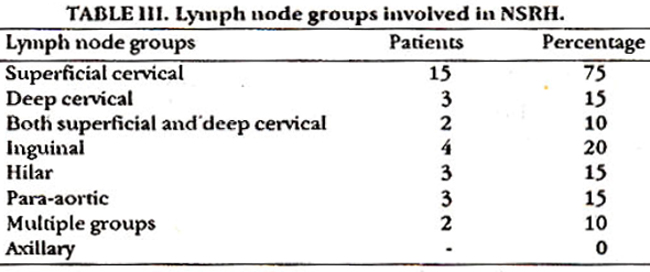
Biopsies were obtained from cervical groups only. Hilar and para-aortic lymph node enlargement was picked upon chest X-ray and abdominal ultrasonography respectively. Follow-up ranged from 9 months to 2-1/4 years. Out of 20, only 18 patients were available for follow up. In 7 patients (39%) there was spontaneous resolution within two months. The remaining 11 patients were re-biopsied. Three (17%) turned out to be tuberculous, two (11%) had lymphoma (one Hodgkin disease, the other non-Hodgkin lymphoma) and one (6%) developed acute lymphadenitis. The remaining five patients (27%) showed non- specific reactive hyperplasia, with lymph node enlargement for more than two years, without further deterioration in general health. There was no mortality in patients during the follow-up period.
DISCUSSION
Non-specific reactive hyperplasia was the second most frequent cause of lymphadenopathy in this series; tuberculosis being the most common, a finding supported by Ahsan1. It affected comparatively younger people (mean age 23 years) although it was still present upto the age of fifty. There was no specific sex predilection. NSRH primarily involved the superficial cervical group although, apart from axillary glands, no group of lymph nodes was spared. The drainage area of superficial cervical lymph nodes is repeatedly subjected to minor trauma and subclinical infection, hence shows nonspecific inflammatory changes2-4. Inguinal lymph nodes nearly always show hyperplastic changes because of minor abrasions and low grade infections in the feet and external genitalia5-8 but were not included in this study. The spectrum of routinely performed investigations did not offer diagnostic hint as has been documented by DePalma9. Follow-up of these patients showed spontaneous resolution within two months in 39% patients. Such patients may have self-limiting viral or non- specific bacterial infection in the area of drainage10 although such could not be substantiated in this study. On rebiopsy, 6 patients (33%) had a specific disease (tuberculosis 3, lymphoma 2 and acute lymphadenitis 1). The possible reason for missed diagnosis in the first instance may be non-representative lymph node selection from too peripherally situated lymph node rather than close to the centre of the lesion11 or crushing of the lymph node during surgery which destroys its morphology12. An omission by the histopathologist. Reactive hyperplasia may distort the structure of lymph node closely simulating lymphoma13. Moreover interpretation of histology of lymph nodes is very difficult in pathology14. It may be initial non-specific response of a specific ailment15.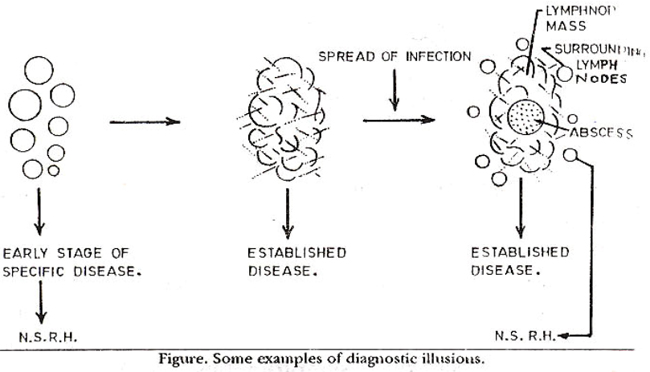
Figure shows how biopsy at an early stage of a specific disease or a biopsy from too peripheral area of an established lesion can miss the diagnosis. The remaining 27% patients showed non-specific reactive hyperplasiaon re-biopsy as well and the problem remained unsettled in them. Selection of lymph node for biopsy should be planned meticulously after thorough examination so as to reduce the chances of missed diagnosis. If possible, the superficial cervical lymph nodes should be avoided in favour of deep cervical group, where a non- specific response will be less likely, a suggestion advocated by Rob and Smith as early as 194716 . Needless to say, the histopathologist should be competent. Patients with non-specific reactive hyperplasia need close follow-up. If the disease does not resolve spontaneously, a rebiopsy should be carried out to reach some definite conclusion.
ACKNOWLEDGEMENT
The author is grateful to Dr. Fauzia Naz, Medical Officer, East Surgical Ward for help in conducting the study. Thanks are also due to Mr. Nayyar Salam for typing the manuscript.
REFERENCES
1. Ahssn, I. Lymphatics and lymph nodes, in textbook of surgery. Byljaz Ahsan. Labors, Qindeel Press, 1991, pp. 389-92.
2. Dudley, H.A.F. and Waxmann, B.P. Neck swellings, in Scott’s an aid to clinical surgery. Edinburgh, Churchill Livingatone, 1989, pp. 114-15.
3. Rains, A.J.H. and Mann, cv. Lymphatics and lymph nodes, in Bailey and Love\\\'s short practice of surgery. 20th ed. London; Lewis, 1988, pp. 124-25.
4. Browse, N.L. Cerviral lymphadenopathy and other neck swelling, in an introduction to the symptoms and signs of surgical disease. 2nd ed. London, Arnold, 1991, pp.249-56.
5. Aird, I. The lymphatic vessels, lymph nodes and reticular tissue, in a companion in surgical studies. 2nd cd. Edinburgh, Churchill Uvingstone, 1958, pp. 228-33.
6. Cotton, L. and Lafferty, K. The lymphatic system, in a new short textbook of surgery. London, Hodder and Stoughton, 1986, pp. 88- 89.
7. WaIter, 3D. and Israel, M.5. The lymphoreticular system, in general pathology. 6th ed. Edinburgh, Churchill Uvingstone, 1987, pp. 418-30.
8. Robbins, S.L. and Kumar, V. Dermatopsthic lymphadenitis, in basic pathology. 4th ed. Philadelphia, Saunders, 1987, pp.402-3.
9. DePalma, RB. Disorders of the lymphatic system, in textbook of surgery. Edited byC. David. 13th ed. Philadelphia, Saunders, 1986, pp. 1696-1708.
10. Rowe, LD. Inflammatory neck masses in current surgical diagnosis and treatment by Lawrence W. Way. 8th ed. Norwalk, Appleton, Prentice, 1988, pp.812-13.
11. Johnstone, J.M.S., Msran, A.G.D. and Rintoul, R.F. Opcratksns on malignant glands of the neck, in Fsrquharsons textbook of operative surgery. 7th ed. Edinburgh, Churchill Livingstone, 1986; pp. 252-56.
12. Russell, R.C.G. Lymph node biopsy, in atlas of general surgery. Edited by H. Dudley, D.C. Carter and R.C.G. RusselL 4th ed. London, Dutterworth, 1986, pp. 28-9.
13. Lutes, R.J. and Tindle, B.H. Immunoblastic lymphadenopsthy - a hyperimmune entity resembling Hodgkin’s disease. N. Engl.J.Med., 1975;292:1-8.
14. Horowitz, CA., Henle, W., Henle, B., Segal, M., Arnold, T., Lewis, LB., Zanick, D. and Ward, P3. Clinical and lalsoratosyevaluation ofelderly patientawith heterophil-antibody positive infectious mononucleosis. Report of seven patients, ages 401078. Am.J. Med., 1976;61:333-45.
15. Greenfield, S. and Jordan, MC. The clinical investigation of lymphadenopathy in primary care practice. JAMA., 1978;240:1388- 93.
16. Robb-Smith, A.H.T. The lymph node biopsy, in recent advances in dinical pathology. London, Churchill, 1947, pp.350-56.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: