
Amjad Ali ( National Institute of Health (NIH), Islamabad. )
M. Motiur Rehman Khan ( National Institute of Health (NIH), Islamabad. )
Zaka Ur Rehman Malik ( National Institute of Health (NIH), Islamabad. )
Barkat Ali Charania ( Aga Khan Health Services, Karachi. )
Faiyaz A. Bhojani ( Department of Community Health, Aga Khan University, Karachi. )
Shahid Mahmood Baig ( Nuclear Medicine Oncology and Radiotherapy Institutute (NOM), Islamabad. )
June 1992, Volume 43, Issue 6
Original Article
ABSTRACT
The study was designed to assess the impact of the supplementation levels of iodine in salt supplied since the last 12 years to Gilgit and Hunza, an endemic goitre area of Pakistan. The ovefall prevalence of visible goitre is reduced from 61.36% to 4.68%. Results of ufinafy excretion of iodine (UEI) indicate severe to mild iodine deficiency among 70.41% of the randomly surveyed households. Severely deficient are 3%, moderate 2g.54% and mild 37.87%, criteria of UEI being <2.0 ug/dI, 2-5 ug/dl and 5-10 ug/dI respectively. Levels of iodine supplementation in 267 iodized salt samples at production (n = 128) and consumption (n = 139) points are compafed With a mean ± SD are 70.86 ± 29.73 ppm and 37.24 ± 20.47 ppm respectively, representing 566.8 ± 237.8 ug and 297.9 ± 163.7 ug of iodine per 8.0 gram of salt. It is suggested to replace common salt With iodized salt in the goitre area to ensure the use by all households and quality control measures for iodination of salt should strictly be adhered so that uniform and consistent supply of iodine be ensured. The magnitude of contributory factors other than iodine deficiency, i.e., environmental and hereditary should be monitored and considered When levels of iodine supplementation are adjusted (JPMA 42: 141, 1992).
INTRODUCTION
Endemic goitre occurs in a large population in a specific area inducing goitre and hypothyroidism. It affects both sexes, but is more common among females in their teens and 20’s; some patients develop gigantic goitres. Since chronic and persistent iodine deficiency is one of the speculative causes of this disease, the term iodine deficiency disorders (IDD) is now commonly used1. Some of the most severe iodine deficiency occurs in relatively young mountainous areas, such as in the Alps, Andes and Himalayas, where iodine in the soil has been washed away by rain and glaciers2. The southwestern side of the Himalayan peaks constitutes one of the classical goitre endemic belts in the world; one such area in Pakistan is that of Gilgit and Hunza valleys. Intervention measures against iodine deficiency disorders began in this area in late 1977. At that time iodized salt was supplied/distributed to the residents of Gilgit and Hunza valleys through the help of an international philanthropic organization. The population of this target area is estimated, based on the 1981 census of the government of Pakistan, to be just under 200,000. The production and supply of the iodized salt for the area has consistently been around 800 metric tonnes which is consistent with the assumption that the average annual salt requirement per capita is approximately 3kg, i.e., just over 8 gm per day3. This study was designed to ascertain the impact of supplementation levels of iodine in the iodized salt supplied to the target area on prevalence of visible goitre and urinary excretion of iodine.
METHODS
The target area in Gilgit comprised four valleys: Chizer, Yasin, Ishkomam and Puntal and that in Hunza two valleys Hunza and Gojal. Sixteen villages were randomly selected for the study located along the main road five to ten miles from the main road and across the river. In each of the villages selected approximately 30 households were visited at random to get iodized salt samples. Urine samples were also collected in one in three of the households visited. The detailed methodology is described elsewhere3. Iodine in the salt was estimated by official methods of the AOAC titrating sodium chloride solution containing iodine with standard sodium thiosulphate solution. One ml 0.005N Na2S2O3 = 0.1058mg I. Urinary excretion of iodine was estimated by the modified Zak method4. Iodine is oxidized to iodate by chloric acid digestion in the presence of sodium chromate. After digestion iodate is estimated by its catalytic action on the ceric-arsenate system.
RESULTS
Overall prevalence of visible goitre in the target area before launching of iodized salt programme was around 61.36% in all age groups and in both sexes (Table I).

After the intervention with iodized salt programme the overall prevalence of visible goitre has dropped to 4.68%. The period of use of iodized salt was from 1-< 10 years. The urinary excretion of iodine in all age groups and in both sexes indicate that 3% people severely deficient in iodine, 29.54% with abnormally low iodine intake, 37.87% people with mild iodine deficiency and 29.54% people with satisfactory levels of iodine excretion in the 132 surveyed household (Table II).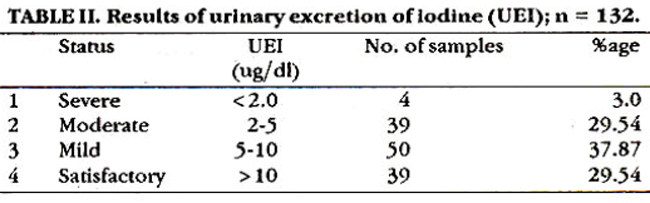
The salt in the target area was supplied by one international philanthropic organization. The levels of iodization at production unit over the last ten years were monitored and were around 70.86 ± 29.73 ppm in 128 randomly selected samples. 139 salt samples from the field were randomly collected and levels were around 37.24 ± 20.47 ppm. It is assumed that salt requirement per capita is approximately 8.0 gram per day, so 566.8 ± 237.8 ug of iodine were calculated at production point which dropped to 297.9 ± 163.7 ug at household level (Table III).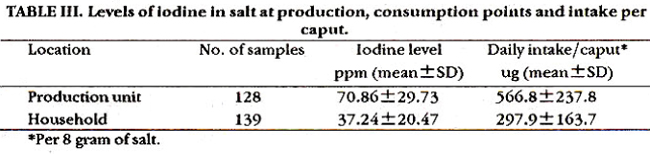
it is assumed that this much quantity of iodine is consumed per person per day.
DISCUSSION
With the use of iodized salt the overall visible goitre prevalence is reduced from 61.36% to just 4.68%. It is noted that goitre is prevalent even after the iodized salt is being supplied to that area for the last 10-12 years. Goitre and iodine deficiency is still prevalent mostly in areas which were 5-10 km away from main roads. It is found that some households are not using iodized salt at all and some households are using iodized salt in combination with locally available rock salt. This situation is confirmed by the results of urinary excretion of iodine where 3% of the visited households are still severely deficient in iodine, 29.54% abnormally low iodine intake and mild iodine deficiency is persistent in 37.87% people. The results of the visible goitre and urinary excretion of iodine presented in the Tables I and II are well explainable when the iodine content of salt at production and consumption levels are compared. There is significant loss (48%) of iodine during transportation, improper storage at household level and highly significant deviation of iodine levels from mean, both at production/consumption ends. The supply of iodine, if 8 gram of salt is consumed per day, is 297.9 ug with very high value of SD ± 163.7 which indicate highly inconsistant intake and these levels further decreased by cooking practices and when salt is used in combination with non-iodized salts resulting in still low consumption of iodine. Low levels of urinary excretion of iodine in 70.41% population visited is in conformity with the quantity and quality of salt consumed in respect of iodine intake (according to WHO recommendations at least 150 ug of iodine be consumed when it is to be supplemented in salt). Moreover, there are various environmental and hereditary factors inducing goitre, in addition to iodine, i.e., digestion of foods from genus brassica, containing thioglucoside and beans containing cyanoglucoside produces thiocyanate and isothiocyanate, which are competitors of iodine transport in thyroid cells; The drinking water containing excess of Mg++ and Ca++ and antithyroid substances produced by E. coli5. These goitrogens may aggravate the picture by interfering with the synthesis of thyroid hormones. Faecal contamination of drinking water is also reported6,7. Steward8 has suggested that geological goitrogen in the rocks of Baltistan, due to drifting of crystal plates and melting there is mineral assemblage in the overlying rocks. As the mineral weathers out they enter the diet, where they produce and enhance iodine deficiency disorders. it is suggested to replace common salt with iodized salt in the entire region to assure the use of iodized salt by all households and the magnitude of contributory factors other than iodine deficiency should also be monitored and consideration be given when the supplementation levels of iodine are adjusted.
REFERENCES
1. Ermans, A.M. Endemicgoitre, in the thyroid. Edited byS.H. lngbarand L.E. Braverman. Philadelphia, Lippincott, 1986, p.705.
2. Dunn, J.T. and Haar, F.V.D. A practical guide to the correction of iodine deficiency. WHO Tech. Manual, 1990, No.3, p.10.
3. Charania, B.A., Malik. Z.U., Bhojani, F.A., Khan, M.M.R. and Au, A. A study of the results often yesra supplyof iodized saltin Gilgit and Hunza. EMRHealth Sew. J., 1988; 5:12-18.
4. Zak. B.. Willard, LL, Mayers, G.B. and Boyle. A.J. Chioric acid method for determina tion of protein hound iodine. AnaL chem., 1952;24:1345-8.
5. Shignoubu. N. and Shigeki, M. Metabolic and endocrine disease. Asian Med. J., 1991;34:77-82.
6. Dietauy goitrogens (editorial). Lancet, 1982; 1:1394.
7. Zafar, A., Cheema, K., Hsssan, K, Shehzsd, L. and Saeed, S. Goitre in school going children in Murree hills. Specialist, 1991; 8:27-30.
8. Stewart, AG. For debate; driftingcontinents and endemic goitre in northern Pakistan. Br. Med.J. Pat, 1990; 1:84-88.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: