
Shifa Naeem ( Department of Psychiatry, Jinnah Postgraduate Medical Centre, Karachi. )
June 1992, Volume 43, Issue 6
Original Article
ABSTRACT
The vulnerability factors were tested in a retrospective study on 50 cases and 50 controls. Only one of the four factors, i.e., lack of an intimate, confiding relationship, was found to be statistically significant, thus highlighting the need for indigenous research particularly in areas where the Variables are socio-culturally determined (JPMA 42: 140, 1992).
INTRODUCTION
Depression, increasingly recognized as a major health problem in the world today, is twice as frequent in women than in men1,2. It is believed that besides biological differences, psycho-social factors play an important role in making women more prone to depression. Brown and Harris3 have suggested four vulnerability factors; (a) lack of an intimate, confiding relationship, (b) loss of mother before eleven years of age, (c) the presence of three or more children under fourteen years of age at home and (d) lack of paid employment which increases the vulnerability of a woman for depression when exposed to a provoking agent. Many similar studies have been conducted in the West4-6 and a need was felt to replicate this in Pakistan. Other psycho-social factors were also explored but in this paper only the vulnerability factors identified by Brown and Harris will be discussed.
PATIENTS AND METHODS
A retrospective case control analytical study was conducted to compare the presence of the above-mentioned vulnerability factors. Using the St. Louis criteria for depression7, fifty cases between 18-45 years of age were selected from among the consecutive female outpatients seen by one of the five teams at the Department of Psychiatry, Jinnah Postgraduate Medical Centre, Karachi between mid-August, 1989 and mid-February, 1990. Fifty controls were taken from the female relatives or friends accompanying the patients. They were also of the same age group but did not fulfil the St. Louis criteria for depression. The cases and controls were administered a specially designed questionnaire which, besides a semi-structured interview, consisted of standardized rating scales8-12. The data thus collected was subjected to statistical analysis (chi square test).
RESULTS
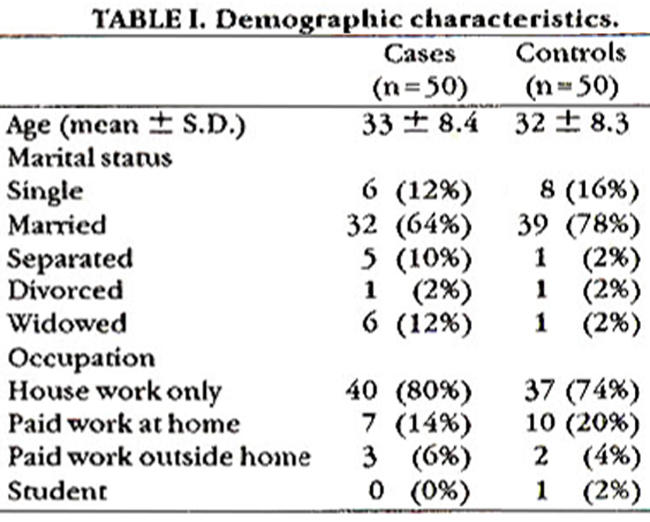
Table I gives the demographic characteristics of the cases and the controls, while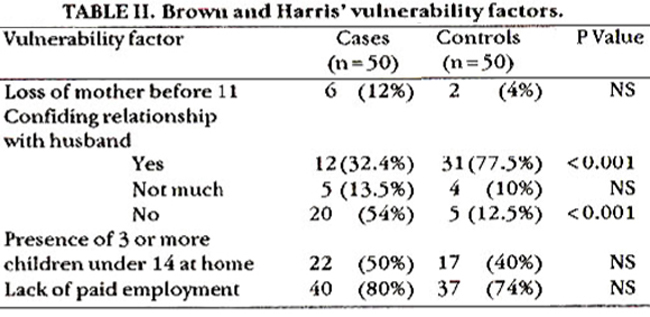
Table II gives the presence or absence of Brown and Harris’s vulnerability factors. The only factor, which showed a significant difference between the cases and controls, was the presence of a confiding relationship with husband. This factor was considered among the married and separated women.
DISCUSSION
Loss of mother before eleven years of age has been investigated as a possible vulnerability factor as it apparently affects a woman’s self-esteem and interferes with her ability to deal with losses in adulthood13. Another possible mechanism is that of “learnt helplessness” where unpredictable and uncontrollable trauma can lead to passive resignation. Brown and Harris found this factor in 22% of the cases and 6% of controls while, in the present study, it was present in 12% of cases and 4% of the controls. Although there was a positive correlation, it was not statistically significant. This could be due to relatively small size of samples. Another possible reason for this factor having less effect in our culture could be the joint family system or general “closeness” of families thus buffering the effect of maternal loss. Lack of intimate, confiding relationship was a difficult area to enquire into or assess. Brown and Harris noted that 38% of women without such a relationship developed depressive symptoths in the presence of a provoking agent, but only 4% of those with such a relationship did so. Other studies have confirmed the association between disturbed marriages and depression in women14,15. In the present study, 54% of cases and 12.5% of controls reported absence of a confiding relationship with their husband (Pc 0.001). Thus a generally poor marriage emerges as a very important factor. The presence of three or more children under the age of fourteen at home did not emerge as a factor, as it was present in 22 cases and 17 controls. Apparently, in our culture, having younger children at home is not as stressful as it is in the West. One reason could be a difference in child-rearing practices. While younger children in the West have fairly tight and demanding schedules regarding mealtime, bedtime, etc., there is generally a more relaxed attitude in our culture. Another possible reason could be that the subjects for this study were taken from the lower socio-economic strata where many young boys are earning hands and young girls are mothers’ helpers and so their presence is more helpful than stressful. Lack of paid employment did not emerge as a vulnerability factor. One reason could be that in the lower socio-economic strata (from which the samples were taken) employment by a woman is taken up only when she is forced by her circumstances and, therefore, does not have the expected ‘protective’ effect. Also, not having an education or training limits a woman’s options and she may end up in a job which she does not find satisfying.
ACKNOWLEDGEMENT
I am grateful to Prof. S. Haroon Ahmed for his invaluable guidance. I would also like to express my gratitude to Mr. Syed Ejaz Alam for his help in statistical analysis.
REFERENCES
1. Kendell, RE. Affective (Mood) disorders, in companion topsychiatric studies. Edited by RE. Kendell and AK. Zealley. 4th ed. Edinburgh, Churchill Livingstone, 1988. p,342.
2. Weissman, MM. and Boyd. ).H. Affective disorders: epidemiology, in comprehensive textbook of psychiatry. Edited by H.I. Kaplan and B.). Sadock. 4th ed. Baltimore, Williams and Wilkins, 1985, pp. 766-67.
3. Brown, G.W. and Harris, T. Social origins of depression: a study of psychiatric disorder in women. London, Tavistock, 1978, pp. 278-88.
4. Bebbington, P. Social epidemiology of depression and the neuroses. Curr. Opinion Psychiatry, 1989; 2:204-7.
5. Birtchnell, 3., Masters, N. and Deahi, MA stud9ofyoung married women on a London housing estate. Br.J. Psychiatry, 1988;153:56-64.
6. Campbell, E.A., Cope, S.J. and Teasdale, J.D. Social factors and affective disorders: an investigation of Brown and Harris\\\'s model. Br.). Psychiatry, 1983; 143:548-53,
7. Peighner, J.P., Robins, E., Guze, SB. et al. Diagnostic cniteris for use in psychiatric research. Arch. Gen. Psychiatry, 1972;26:57-67.
8. Beck, AT., Ward, C.H., Mendelson, M., Mock, 3. and Enbaugh,). An inventory for measuring depression. Arch. Gen. Psychiat., 1961;4:561-71.
9. lIsmilton, M. Development of a rating scale for primary depressive illness. Br.). Social Clin. Psychology, 1967;6:278-96.
10. Sen. B., Wilkinson, 0. and Man, ).). Psychiatric morbidity in primary health care. A two-stage screening procedure in developing countries: choice of instruments and cost-effectiveness. Br.). Psychiatry, 1987;151:33-38.
11. Singh. 0., Kaur, 0. and Kaur, H. P.S.L.E.S. - a new stressful life events scale for use in India. Indian Psychiatry, 1984;26:107-14.
12. Smilkstein, 0., Ashworth, C. and Montano, 0. Validity and reliability of the family APGAR ass testof familyfunction. 3. Pam. Pract., 1982;15:303-11.
13. Brewin, CR. Psychological factors in the aetiology of depression. Cur. Opinion Psychiatry, 1989;2:213-16.
14. Birtchnell, ). and Kennard, ). Marriage and mental illness. Br.). Psychiatry. 1983;142:193-98.
15. Miles. A. Women and mental illness: the social context of female neurosis. Sussex Harvester Press, 1988, pp.27-30.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: