
Waquar Uddin Ahmed ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Huma Qureshi ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Ejaz Alam ( PMRC Research Centre Jinnah Postgraduate Medical Centre, Karachi. )
Sarwar J. Zuberi ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Qamar Jamal ( Department of Pathology, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
S. Mahmood Alam ( Department of Pathology, Basic Medical Sciences Institute, Jinnah Postgraduate Medical Centre, Karachi. )
June 1992, Volume 43, Issue 6
Original Article
ABSTRACT
Between January, 1979 to August, 1990, 107 histologically proven cases of oesophageal carcinoma were seen. The ages of the patients ranged from 19-85 years (mean 55±14 years) with a male to female ratio of 1.2:1. Majority (70%) of the cases belonged to lower socioeconomic group and 56% were migrants from India. History of tobacco chewing or smoking was present in 78% cases. In 54%, the lesion was located in the middle third of the oesophagus, followed by lower third in 44%. Histology showed squamous cell carcinoma in 86% and adenocarcinoma in 10% cases. Of the 19 cases followed, 16 underwent surgery and 3 received chemotherapy. Two cases died within 7 months following surgery and in 6 carcinomas recurred. All cases receiving chemotherapy died within 8 months of treatment (JPMA 42: 133, 1992).
INTRODUCTION
World-wide, geographic differences have been observed in the incidence as well as frequencies of oesophageal carcinoma. Variations as low as less than 5/100,000 to as high as 100/100,000 population have been reported1-3. The data, obtained from a multicentre report of malignant tumours in Pakistan, shows carcinoma of the oesophagus to be the 8th commonest tumour in males and 5th in females4. In Sindh it was the 4th commonest tumour in both sexes while in the other three provinces it was not even one of the ten commonest tumours4. In 1973-74, it was the 9th commonest tumour in males and 5th in females and in 1977-80, it became the 8th and persisted as the 5th commonest tumour in females4. The above figures indicate that either the frequency of oesopbageal carcinoma is increasing in our country or with the availability of better diagnostic facilities, the lesion is being diagnosed more frequently. Although carcinoma of the oesophagus is a common malignant tumour in Pakistan, especially in Sindh, no baseline data is yet available on the site, extent, presentation or follow-up of these cases. The aim of the present analysis was to collect baseline data so that further work may be done in the etiopathogenesis of this common malignancy.
PATIENTS AND METHODS
Case records of patients with endoscopically and histologically confirmed cases of carcinoma oesophagus seen from 1979-1990 were analysed. Information about age, sex, occupation and addictions was evaluated along with place of origin, place of longest stay and mother tongue to see if oesophageal carcinoma had any predisposition for any specific region or population group. Site of lesion was classified as upper, middle and lower according to the classification of American Cancer Society2. Most of the patients, once diagnosed, were sent to the radiotherapy department for cancer registration and radio/chemotherapy, therefore, follow-up data was available on a limited group of patients who underwent surgery.
RESULTS
One hundred and forty four endoscopically proven cases of oesophageal carcinoma were seen at PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. Thirty seven cases were excluded because of inconclusive biopsy and 107 histologically proven cases were finally analysed. Of these 59 (55%) were males and 48 (45%) females, giving a male to female ratio of 1.2:1. Age of the patients ranged from 10-85 years with a mean of 59±13 years in males and 50±13 years in females. Age adjusted frequency of our cases is compared with the age distribution of the population in Figure.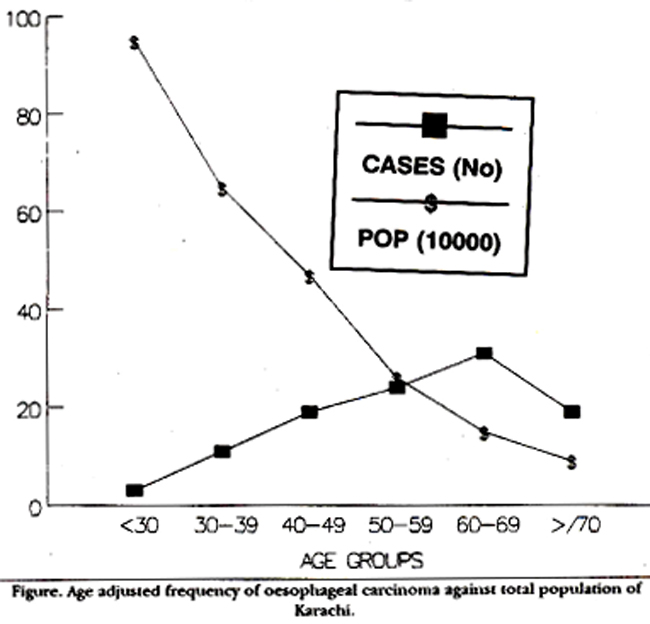
Duration of disease at the time of presentation ranged from one month to 3 years in males (median 4 months) and upto 7 years in females (median 3 months). Sixty cases (56%) were born in undivided India and later migrated to Pakistan, with majority settling in Karachi. Origin and the place of longest stay of these cases is shown in Table I.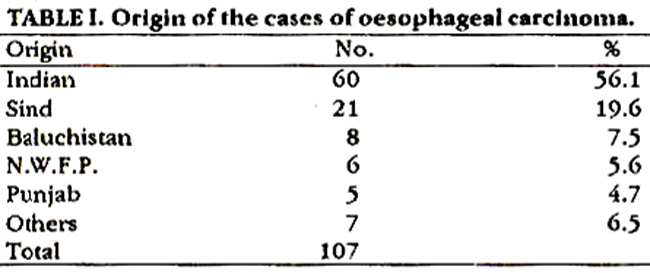
Occupation of the patients were taken as an indirect measure of their soeioeconomic status. Majority (70%) of the cases belonged to lower socioeconomic group comprising of daily wage workers. Overall 83 (77.5%) cases were addicted to either tobacco chewing or smoking or both with smoking being frequent in males (n = 40) and tobacco chewing in females (n = 22). Mean consumption of cigarettes/day were 17 in male and 12 in female. Only one patient gave history of opium addiction while none drank alcohol. Median time of addiction was 20 years, ranged 5-40 years. Only 7 males and 16 females had no addictions. Comparative figures of various types of addictions in general population is shown in Table II.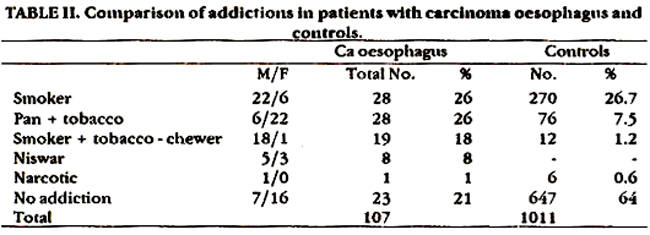
Major presenting symptoms were dysphagia 100 (93%), weight loss 79(74%), vomiting 66(62%), anorexia 52 (49%), abdominal pain 39 (36%) and G.I. bleeding (7%); Seven patients had no dysphagia on presentation. Endoscopy revealed a fungating growth in 68 (64%) followed by ulcerating and nodular growth in 17 cases each and polypoid in 5 cases. Site of lesion was middle 1/3 in 58(54%), lower 1/3 in 47 (44%) and upper 1/3 of the oesophagus in 2 cases. Histology showed squamous cell carcinoma in 92 (86%), adenocarcinoma in 11 (10%) and undifferentiated in 4 cases. Distant metastasis was present in 19 cases on first presentation, of these the spread was noted in the lymph nodes in 7 (cervical and supraclaricular 3, mesenteric 2, para-aortic and ciliac 2), stomach and liver in 4 cases each and abdomen and lung in 2 cases each. Most cases were previously sent to the radiotherapy department for cancer registry and chemo/radiotherapy, therefore, no attempt was made to follow these cases. Follow-up was available only in operated cases. Of 19 cases in whom follow-up was available, 16 were operated (resection and anastomosis) and 3 received chemotherapy alone. Post-operative recurrence within 2-30 months (mean 13±8 months) occurred in 6 cases, while 2 expired 7 months later. Eight patients are still in follow-up varying from 2-24 months (mean 8±7 months) and are asymptomatic. All 3 cases receiving chemotherapy expired within 8 months of completion of therapy.
DISCUSSION
The present study shows the frequency of oesophageal carcinoma at one centre, in one of the hospitals of Karachi. The actual frequency of this lesion in the same hospital would be higher because patients with oesophageal carcinoma are admitted and treated in the surgical, medical, ENT and radiotherapy departments. Highest prevalence of oesophageal carcinoma (100/160,000 population) has been reported from Kazakhistan province of Russia, Gonbad region of northern Iran, Hunan province of China and southern Transkei district of South Africa3. Major risk factors include alcohol abuse and heavy smoking2. No evidence of the role of alcohol abuse emerged from studies done in Iran5, instead mutagenic products of opium and tobacco which are frequently ingested in Iran and Transkei, respectively, have been proposed to cause cancer in these regions6. Deficiencies of certain minerals7-10 and the role of mineral deficiencies in promoting fungal invasion and mycotoxin contamination of good stuff” have some association in occurrence of oesophageal carcinoma. Cigarette smoking alongwith alcohol consumption potentiate the mutagenic effect of each other2. In the present study, although a large number (78%) of patients were tobacco users, either as smokers or chewers, but none were taking alcohol. Similarly only one case in the present study was an opium user. Therefore, at least alcohol and opium are not the causative factors for oesophageal carcinoma in our patient population. Deficiency of vitamin A causes alteration of epithehal tissues and squamous metaplasia like that induced by chemical carcinogens12. Low levels of vitamin A (less than 20 mcg/100) were found in 20% and 16% males and females under 15 years of age, in a survey carried out in general population in Karachi while in adults over 15 years of age only 1% and 2% males and females showed deficiency respectively13. Low levels of vitamin A were found in 51% patients suffering from squamous cell carcinoma of the oropharynx and oral cavity in Karachi14. Seventy percent of patients in the present study were less than 60 years of age in contrast to only 18-35% in the West and 43% in Saudi Arabia15. Early occurrence of squamous cell carcinoma in our patients probably suggests an early exposure to the carcinogen. Although no known carcinoma providing agent has been identified in our patients but the role of vitamin A deficiency, fungal contamination of food stuff, pan chewing and contamination of drinking water with petroleum products in the occurrence of oesophageal carcinoma in our patients should be studied.
REFERENCES
1. Tuyna, A.J., Pequignot, G. and Jenson, D.M. Role of diet, alcohol and tobacco in oeaophageal cancer aa illustrated by two contrasting high-incidence areaa in the North of Iran and West of France. Front. Gaatrointeat. Res., 1979; 4:101-10.
2. Rogera, EL., Goldtind, L. and Goldkind, S.F. Increasing frequency of oeaopbageal cancer among black maleveterana. Cancer, 1982;49:610-17.
3. Doll, R. Geographical variation in cancer incidence. A clue to causation. World). Surg., 1978;2:595-602.
4. Pakittan Medical Retearch Council Malignant tumoura. Reportof a multicentre atudy. Karachi, PMRC., 1982; 1-12.
5. Cook-Mozallari, P.J., Azordegan, F., Day, N.E., Reaaicaud, A., Sabai, C. and Aramcah, B. Oeaophageal cancer studies in the Caapian Littoral of Iran; results of a caae-control atudy. Br.). Cancer, 1979;39:293-309.
8. Hewer, T.F., Roae, E., Ghadirian, P., Bartach, H., Malaveille, C. and Day, N. Ingested mutagens from opium and tobacco and cancer of oeaophagua. Lancet, 1978;2:494-96.
7. The Coordinating Group for Research on etiology of oeaophageai cancer in North China. The epidemiology and etiology of ocaophageal cancer in North Chine. Chin. Med.J., 1975; 1:167- 183.
8. Burell, R.J., Roach, W.A. and Shadwcll, A. Ocsophageal cancer in the bantu of the Transkei aaaociated with minerat deficiency in garden planta. JNCI., 1966; 36:201-9.
9. Kmet, J. and Mahboubi, E. Eaophageal cancer in the Catpian Littoral of Iran: initial atudiea. Science, 1972;175:846-53.
10. Berg. 1W., Diet persona at high risk of cancer. Edited by J.F. Fraumeni. San Diego, Academic, 1975,pp. 201-19.
11. Maraeaa, W.F.,van Renaburg, S.J. and Mirocha, C.J. Incidence of futarium species and the myeetoxine, deoxyivalenol and zearaleone, in cprn produccd in oesophageal cancer areas in Transkei. 3. Agric. Food Chem., 1979; 27:1108-12.
12. Mellow, M.H., Layne, E.A., Lipman, T.O. Kaushik, M., Hoatetlcr, C. and Smith, J.C.Jr. Plaama zinc and vitamin A in human squamous carcinoma of the oeaophagua. Cancer, 1983; 51:1615-20.
13. Ibrahim, K. Plaema vitamin A and carotene inch in general population residing in Karachi. Karachi, University of Karachi, 1980, p.65 (thesk).
14. Ibrahim. K., Jafarey, NA. and Zuberi, S.). Plasma vitamin A and carotene levels in squamous cell carcinoma of oral cavityand oropharynx Clin. Oncology., 1977; 3:203-7.
15. Amer, M.H., Gazigi, A., Hannan, M.A. and Mohammed, M.E. Water contamination and oeaophageal cancer at Gaaim region, Saudi Arabia. Gastroenterology. 1990;98:1141-47.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: