
Salma Halai Badruddin ( Departments of Medicine, The Aga Khan University Medical Center, Karachi. )
Ayesha Molla ( Department of Pathology, The Aga Khan University Medical Centre, Karachi. )
Mohammed Khursheed ( Department of Pathology, The Aga Khan University Medical Centre, Karachi. )
Sandra Vaz ( School of Nursing, The Aga Khan University Medical Center, Karachi. )
November 1993, Volume 43, Issue 11
Original Article
Abstract
Eighty-eight school children and their parents who had been counselled regarding appropriate dietary and activity patterns aimed at reducing serum cholesterol were followed-up 21 months later to determine changes in dietary and activity patterns and in serum lipid levels. The decline in serum total cholesterol ranged from 8 to 14% in the different age and sex groups (P <0.05 to P <0.001). Serum triglycerides did not change significantly. Cholesterol intake decreased 36% and 54% in 10-14 year old boys and girls respectively (P >0.001 ). The activity level increased significantly in both the 5-9 year and 10-14 year olds (P <0.05 to P <0.005). These results show that nutrition education can bring about a change in dietary and activity patterns, resulting in a decline in serum cholesterol levels (JPMA 43:235, 1993).
Introduction
Our earlier studies on school Children have shown that 58% of children from well to do families1, have serum cholesterol levels above 4.4 mmol/L (170 mg/dl), a level at which it is recommended that children be counselled regarding diet and exercise to lower serum cholesterol levels. Hypercholesterolemia is a known risk factor for coronary heart disease2 and it has been reported that children whose serum cholesterol levels are high tend in general to have high levels as adults3,4. Positive cross-sectional associations between various indices of obesity with serum total cholesterol (TC), triglycerides (TG) and low-density lipoprotein cholesterol (LDL-C) in both adult and children have been reported and high density lipoprotein cholesterol (HDL-C) has been shown to be inversely associated with obesity5-7. Prospective studies in adults and adolescence have indicated that increases in obesity are positively associated with increases in levels of TC, TG and LDL-C8-10. Torland and Gillam11 have reported an association between the level of physical activity and serum lipids values in children. Higher levels of physical activity were correlated with lower TG levels and higher HDL-C to TC ratios. Similarly TC and TG levels tended to be lower or HDL-C levels higher in children from schools where they were strongly encouraged to exercise12. The present study was undertaken to assess the effectiveness of the counselling given to the children and parents in bringing about changes in dietary and activity pattern which would result in a decrease in serum cholesterol levels.
Subjects and Methods
87 children (41 males, 46 females) who were identified as having serum cholesterol levels > 4.4 mmol/L (> 170 mg/dl) and were counselled regarding needed changes in dietary and activity patterns were followed up 21 months after the initial blood test that identified them as hypercholesterolemic.
Biochemistry
All subjects fasted overnight for 12-14 hours before blood collection in the morning. About 5 ml of blood was collected in neutral tubes, centrifuged and stored at 4°C. Cholesterol and’ triglycerides were estimated by enzymatic methods13,14 using a Beckman ASTRA autoanalyzer. HDL and LDL cholesterol were estimated using the Boehringer kit following the methods of Burnstein et al and Lopes-Vireila et al15,16.
Nutritional Assessment
Heights and weights were recorded at the time of drawing blood and a detailed interview conducted by trained nutritionists regarding food intake and activity patterns. Cholesterol intake was calculated using food composition tables17,18.
The children were classified according to the number of physical activity periods of 30 minutes each per week as follows:
Sedentary <3
Moderately active 3-5
Active >5
Counselling
Eight children of the same age and sex were invited with their parents to attend a counselling session. At the beginning of the session each parent child pair was informed of the child’s weight status relative to the height. The focus of the counselling session was on how to meet the nutritional needs of the children by diets that were low in total fat, cholesterol and simple sugars and high in complex carbohydrates and fiber. The total quantity of food required by the children in a day was displayed. The childrens need for physical activity and how this could be incorporated into the daily routine were explored in depth. The whole session was very interactive with parents and children raising questions and concerns. After the joint session, the nutritionists met with each parent-child pair and evaluated the child’s individual needs regarding appropriate body weight, food likes and dislikes and activity patterns. The strengths and weaknesses of the child’s usual dietary pattern as obtained from the dietary interview were pointed out and ways to improve the diets were discussed. The aim of the individualized counselling was to help the parents and child to formulate an action plan which was acceptable to both and in keeping with the scientific guidelines for meeting nutritional needs and lowering cholesterol levels. The parents were followed-up by at least one pjione call 12 weeks after the counselling to remind them to monitor their child’s serum lipid levels, diet and activity and to address any questions or queries the parents may have.
Statistical Analysis
Paired students "t" test was used to test for differences in values for mean serum cholesterol and triglycerides and cholesterol intake before and after counselling. Chi-square with Yates correction was used to test for significance in changes in activity levels.
Results
Serum total cholesterol and triglyceride levels before and after counselling are shown in Table I.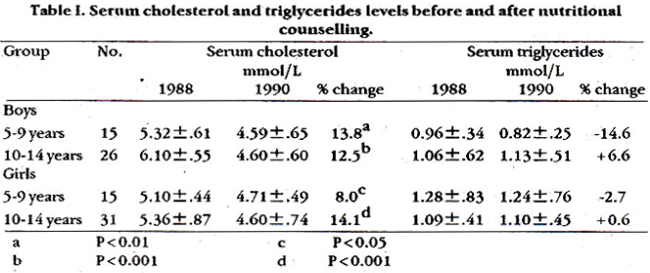
There was a significant decrease in the serum cholesterol levels in all four groups ranging from 8% in the 5-8 year old girls to 14.1% in the 10-14 year old girls. The mean TG values ranged from 0.96 mmol/L for the 5-9 year old boys to 1.28 mmol/L for the 5-9 year old girls. There was no significant change in the serum TG values after counselling. The maximal change was observed in the 5-9 year old’ boys whose TG values decreased 14.6% from 0.96 to 0.82 The mean LDL-C ranged from 2.7 mmol/L in the 5-9 year old boys to 3.1 mmol in the 5-9 year old girls. The mean HDL-C level was 1.5 mmol/L in the 5-9 year old boys, the other three groups all had mean HDL-C level of 1.2 mmol/L. LDL-C and HDL-C levels were not determined prior to counselling, therefore, no- comparative results are available. The cholesterol intake decreased in all four groups but the change was significant only in the 10-14 year olds (Table II).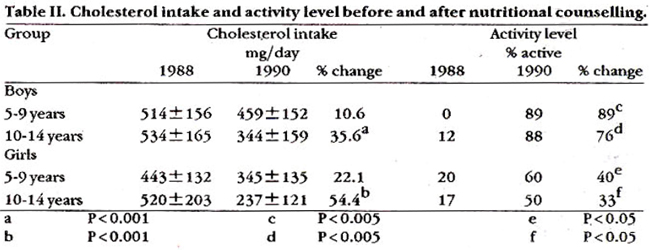
The major change in food intake was a decreased consumption of eggs, milk and cheese. The 10-14 year old girls decreased their mean milk intake from 1.5 glasses/day to 1.0 glass/day, their egg intake decreased from about 4/week to! 1/week and the frequency of cheese intake decreased from 3.5/week to 1.5/week. Most children ate organ meats 1-3 times/month, after counselling the frequency of intake declined to less than once a month. More striking changes were seen in the activity levels especially for the boys, but for all age and sex groups there was a significant increase in the percentage of children classified as active. All the children had gained weight in the 21 months since the time their weight was recorded in 1988 but relative to their height 50.5% had decreased their body weight, 10% remained the same and 39.5% had a higher relative body weight.
Discussion
Although the serum TC decreased considerably in all four groups, the LDL-C levels were still at or above the 75th percentile of values of North American children except for the 10-14 year old girls. The HDL-C levels tended to be low with only the 5-9 year old boys having values above the 50th percentile; the other three groups had HDL-C values that were at or below the 25th percentile of values for North American children of comparable age and sex19. The percent decrease in serum TC is even more remarkable when one considers the fact that an increase in TC levels of 0.16 to 0.41 mmol/L is reported to occur during childhood20. However, the absence of a control group in our study makes it difficult to attribute these changes to the counselling given. The possibility exists that just the awareness that the child’s serum cholesterol level was high might have brought about changes in food intake and activity which in turn resulted in a decrease in serum cholesterol levels. We feel however, that this is unlikely on the basis of our qualitative observation during the counselling sessions. Those children who were >5% above expected weight for height were often perceived by their parents, as being underweight or normal, therefore, they would be unlikely to curtail caloric dense foods. Secondly, there was a great deal of resistance, especially by parents of the younger children to recommendations to decrease intake of foods such as eggs, cheese and where necessary, milk. These were generally classified by parents as “good foods and essential for growing children. It was only after considerable reassurance from the nutritionist (SHB) that the parents agreed to consider decreasing their child’s intake of such foods. Nonetheless, the results show that this decrease was much more marked in the older age groups who made their food choices relatively independently of their parents as compared to younger age groups who were still influenced by parental control over food intake. Parents were much more receptive to the idea of increasing their childrens physical activity and this is reflected in the significant increase in physical activity observed in these children. Becque et al have shown that exercise in addition to moderate dietary restriction can result in a reduction in the serum lipids in obese adolescents21. Similarly, Tamir and co-worker have reported that a health education programme in school resulted in a decrease in TC and BMI and increase in HDL in children age 7-9 years22. The World Health Organization has projected that in another 10 years there will be more deaths from cardiovascular diseases in the developing countries, than - from a number of infectious disease combined including diarrhoeal disease, schistosomiasis, tuberculosis, malaria, measles and whooping cough23. The results of this study show that risk factors for heart disease are modifiable during the school ages and health programmes designed to inculcate healthy lifestyles in school age children may help to avert the epidemic of heart disease that threatens to engulf us.
Acknowledgement
The authors wish to thank the children and administration of the Karachi Grammer School as well as the parents for their co-operation in the study. We also wish to acknowledge the assistance of Mr. Sulaiman Gilani in the preparation of the manuscript.
References
1. Badruddin, S.H., Khurshid, M., Molla, A. etst Factorsassociated with elevated serum cholesterol levels in well-to-do Pakistani school children. I Trop. Med. Hyg., 1991;94:123-29.
2. National cholesterol Education Programme. Report of expert panel on blood cholesterol levels in children and adolescents. Pedistrics, (Suppl. 3, Part 2), 1992;89:525- 84.
3. Lauer, R.M. and Clark, W.R. Use of cholesterol measurements in childhoodfor the prediction ofadult hypercholesterolemia. TheMuscatine study. JAMA., 1990;264:3034-38.
4. Orchard, Ti., Donahue, R.P., Kuller, LI-I. et al. cholesterol screening in childhood: does it predict adult hypercholesterolemia? The Beaver county experience. 3. Pedistr., 1983;103:687-91.
5. Frerichs, R.P., Webber, US., Srinivasan, SR. et al. Relation of serum lipids and lipoprotein to obesity and sexual maturity inwhite and black children. Am.J. Epidemiot, 1987;125:186-96.
6. Freedman, D.S., Srinivaaan, S.R., Shear, CL et at. Correlates of HDL cholesterol and apolipoprotein A-I levels in children: The Bogaluss Heart Study. Arteriosclerosis, 1987;7:354-60.
7. Aristimuno, 0.0., Foster, TA., Voors, A.W. et al. Influence of persistent obesity in children on cardiovascular risk factors: The Bogslusa Heart Study. circulation, 1984;69:895-904.
8. Freedman, D.S., Burke, G.L, Harsha, D.W. et at. Relationship of changes in obesity to serum lipid and lipoprotein changes in childhood and adolescence. JAMA., 1985;254:515-20.
9. Noppa, H. Body weight change in relation to incidence of iachemic heart disease and change in risk factors for ischemicheart disease. Ami. Epidemiol., 1980;111:693-704.
10. Khoury, PMorrison, J.A. and Mellies, M. Weight change since age I8years in 30 to 55 year old whites and blacks: associations with lipid values, lipoprotein levels and blood pressure. JAMA., 1983;250:3179-87.
11. Torland, W.G. andOillam, T.B. comparison of serum lipids between babituallyhigh and low active pre-adoleacent males. Med. Sci. Sports. Exerc., 1981;13:316-21.
12. Yathamoto, A., Horibe, H., Sawada, S. et al. Serum lipid levels in elementatyand junior highachool children and theirrelationahip to relativeweight. Prey. Med., 1988;17:93 108.
13. Allian, CC, Poon, US., chan, CS.G. et at. Enzymatic determination of total serum cholesterol din. chem., 1974;20:470-75.
14. Bucolo, 0. and David, H. Quantitativedetermination of serum triglycerides by the uaeof enzymes. Clin. Chem., 1973;19:476-82.
15. Burnstein, M. Rapid method of isolation of lipoprotein from human serum by precipitation with poly-anions. J. Lipid Res., 1970,11:583-95.
16. Lopes-Virella, M.F. cholesterol determination in high density lipoprotein separated by three differentmetbods. din. chem., 1977;23:282-84.
17. Gopalan, c., Rama Sastri, B.V. and Balasubramanian, s.c. Nutritive value of Indian foods. National Institute of Nutrition. Indian Coun. Med. Res. Hyderabad, India, 1985.
18. Pennington, J.T.A> and church, H.N. Food valuesof portions commonly used. 14th ed. Philadelphia, J.B. Lippincott Co., 1984.
19. Lipid Research clinics, Population Studies, Data Book Vol 1.The prevalence study, Washington DC. Department of Health and Human Services. Public Health Service. National Institute of Health, Publication Number 80-1527, 1980; pp. 28-81.
20. Berenson, 0.5. and Epstein, F.H. Conference on blood lipids in children: optimal levels for early prevention of coronaty artery disease. Prev. Med., 1983;12:725-902.
21. Becque, M.D., Katch, V.L., Rocchini, A.P. et al Coronary risk incidence of obese adolescents: reduction by exercise plus diet intervention. Pediatrics, 1988;81:605-12.
22. Tamir, D., Feurstein,A., Brunner, S. etal. Primary preventionofcardiovasculardiseases in childhood; changes in serum total cholesterol, high density lipoprotein and bodymass index after 2 years of intervention in Jerusalem school children aged 7-9 years. Prey. Med., 1990;19:22-30.
23. World Health Organization. Heart beat: the rhythm of health. CH- 1211, Geneva 27, Switzerland, WHO., 1992.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: