
Fariyal F. Fikree ( Department of Community Health Sciences, The Aga Khan University, Karachi. )
November 1993, Volume 43, Issue 11
Original Article
Abstract
Crowding is known to be associated with an increased risk of infant and child morbidity and mortality particularly due to Infections. We examined the association of crowding with perinatal mortality. Our results indicated a paradoxical relationship with the least crowded households showing the highest perinatal mortality (7.7% as compared to 4.7%). However, further analysis indicated that the observed paradoxical relationship is a spurious one, largely explained by the confounding effect of gravidity (JPMA 43: 230, 1993).
Introduction
Studies in developing countries indicate that children living in crowded environments are at a higher risk of infant and child morbidity and mortality, primarily due to an increased exposure to such infectious diseases as diarrhoea, measles and pneumonia1-3. Mosley and Chen4 in their conceptual framework for child survival propose that household crowding is an environmental characteristic that can directly or indirectly influence child morbidity and mortality. The mechanism of an increased risk of spread of infectious diseases is more likely to affect mortality in the post-neonatal than the neonatal and perinatal period. Perinatal and neonatal mortality is primarily related to the maternal environment during pregnancy, labour and delivery. Consequently, the association between perinatal mortality and crowding (if any) may operate through increased psychosocial stress resulting from overcrowded living conditions5 rather than the spread of infections. Newton et al6 have shown that psychosocial stress was significantly associated with a higher prevalence of premature labour resulting in increased perinatal morbidity and mortality. In a review of literature on the relationship between stress and reproduction, Gray7 concluded that there is an increased risk of delivering premature and low birth weight infants by mothers exposed to such maternal stress as major life events and work pressure. We were interested in examining the association between crowding and perinatal mortality using data from lower socioeconomic settlements in Karachi, where the average household size is 6.6 and over 50 percent of the population live in crowded households (number of persons per room> 4).
Materials and Methods
A demographic survey was conducted in eight lower socioeconomic settlements of Karachi, during August and September, 1989. A total of 10,500 households were interviewed with a response rate of 98 percent. Detailed information on household composition, migration, number of living rooms and socioeconomic factors such as household assets and facilities were collected. Information on the pregnancy history of ever-married women aged 15-54 years, truncated to the past five years, was also included. Crowding was classified into low (<4), moderate (4-7) and high (>8) categories depending on the number of persons per living room. Household structure was categorized into extended or nuclear depending on presence or absence of a multigenerational family structure. Household assets (considered as a proxy indicator for socioeconomic status) was a composite index developed on the ownership of eight modern objects: radio, cassette recorder, sewing machine, refrigerator, washing machine, video cassette recorder, motor-bike and car. There were 375 perinatal deaths out of 6,936 births. For the purpose of this analysis, the perinatal deaths are estimated per 100 current survivors (6,070). This paper presents descriptive and stratified analysis, including direct adjustment8, to describe the relationship between crowding and perinatal mortality.
Results
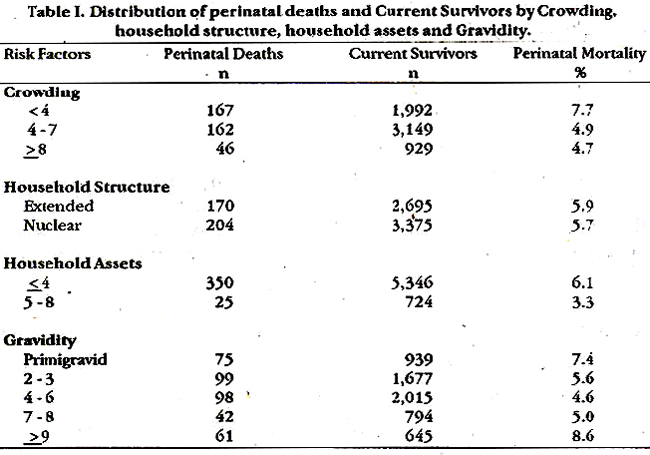
Table 1 presents the perinatal mortality for crowding, household structure, household assets and gravidity. Paradoxically, increased housing density (crowding) had a negative effect, with the most crowded households (>8) having the lowest perinatal mortality. The relationship of perinatal death with household structure, household assets and gravidity were next examined as we hypothesized that these may be potential confounders. There was no significant differente in perinatal mortality between extended and nuclear households (Table 1) even after stratification by crowding (Figure 1).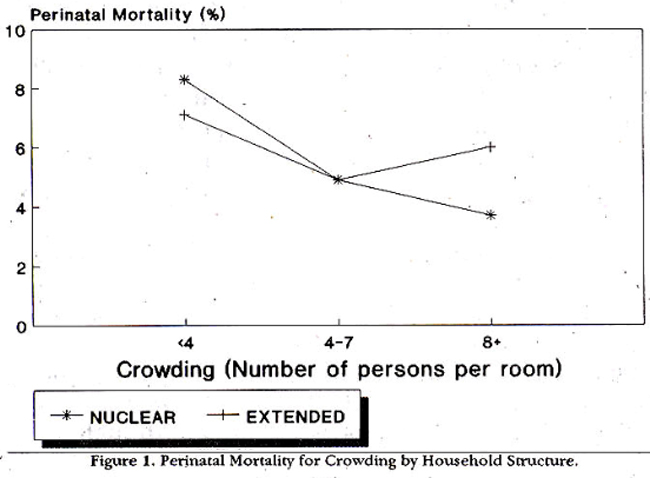
Mthough perinatal deaths were more common in poorer households, the paradoxical relationship between crowding and perinatal mortality was Observed among poorer households household assets), while richer households (5-8 household assets) showed the expected pattern of higher mortality in more crowded dwellings (Figure 2; Table II).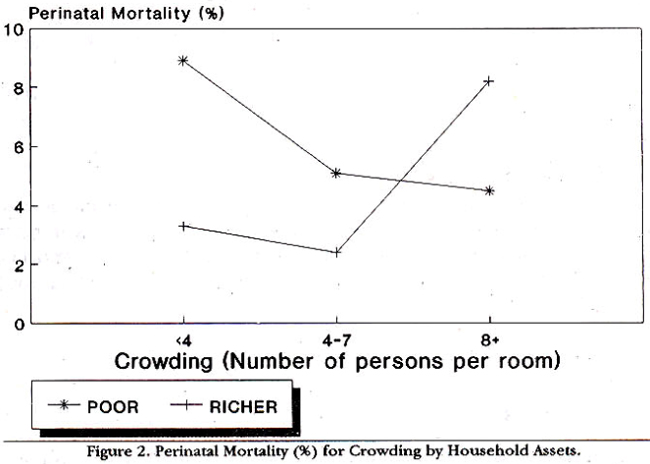
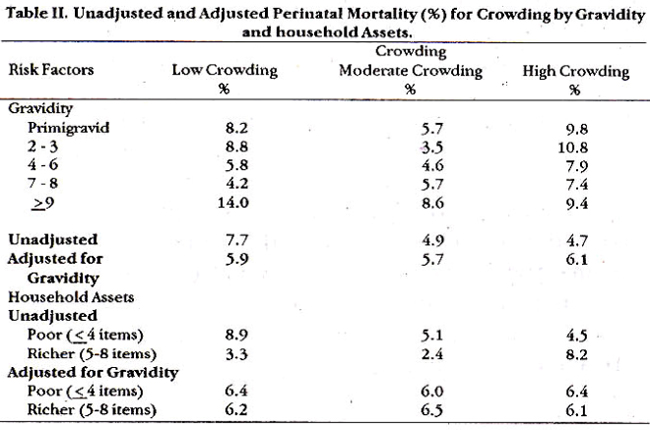
Mortality was highest for primigravid and grand multi gravid (> 9) women. However, stratifying by gravidity, the crowding relationship was taggerated for grand multi gravidity (> 9), though the inconsistent pattern remained for gravidity less than 9 (Figure 3; Table II).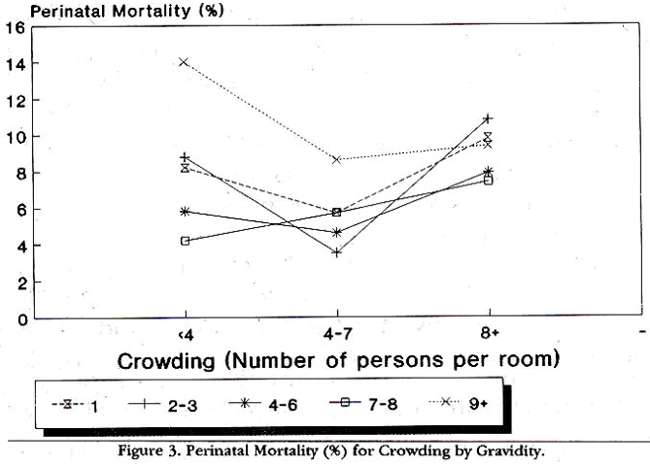
Next, we estimated adjusted perinatal mortality rates, using direct adjustment techniques, initially for gravidity and then simultaneously for gravidity and household assets (Table II). The paradoxical relationship of crowding was eliminated after adjustment for gravidity with no further changes observed whim we simultaneously adjusted for both gravidity and household assets.
Discussion
Crowding is associated with increased infant and childhood mortality partly as a result of increased transmission of infection, and in part because more crowded households are generally of lower socioeconomic status2,4. Studies have also suggested that psychosocial stress can lead to poor pregnancy outcomes6,7 and crowding has been considered a possible cause of psychosocial stress5 with more crowded households experiencing the greatest risk of perinatal mortality. However, our results showed an apparent paradoxical relationship between crowding and perinatal mortality with the most crowded households showing the least risk. This was contrary to what we expected, so we undertook more detailed analyses to assess whether this relationship was due to confounding or interaction with variables such as household structure, household assets and gravidity. We found that this paradoxical relationship was eliminated after adjustment by gravidity suggesting that crowding was substantially confounded by gravidity In summary, the observed paradoxical effect of higher mortality in the least crowded households is a spurious association which is explained largely by gravidity and not by socioeconomic conditions. The high perinatal mortality in least crowded households for grand multigravid (> 9) women may reflect either a poor obstetric history or older mothers whose children have left the household. In conclusion, our results indicate that crowding (considered as a proxy indicator for maternal psychosocial stress or infection risk) showed no association with perinatal mortality. The inconsistent finding was, in part, due to confounding by gravidity.
Acknowledgements
I am deeply indebted to Dr Ronald H. Gray for his invaluable contribution to this manuscript. I appreciate and acknowledge members of the MIMS team: Drs John Bryant, Heinz Berendes, Mehtab Karim, Farid Midhet, Jose Villar, and William Calvert, Saad bin Khalid, Iqbal Azam and field personnel for their valuable support and contribution to the study. This investigation received financial support from the HNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases. I also gratefully acknowledge help from Hewlett Foundation and NICHD/NIH. Support for this study was provided by research grant SFCP 08-024-N.
References
1. Victora, C.G., smith, P.O., Barros, F.C. et al. Risk factors for deaths due to respiratory infections smongBrazilian infants. lnt.J.Epidemiol., 1989;18:918-23.
2. Asby, P., Bukh, J., Lisse, l.M. et al. Overcrowding and intensive exposure as determinants of measles mortality. Am.J. Epidemiol., 1984;120:49-63.
3. Aly, H.Y. Demographicand socioeconomic factors affectinginfsnt mortality in Egypt.J. Biosoc. Sci., 1990;22:447-51.
4. Mosley, W.H. and Chen, L.C. An analytical frsmework for the study of child survival in developingeountries. Popul. Dev. Rev., 1984 (Suppl);10:25-45.
5. Johnson, D.R. and Booth, A. crowding and human reproduction. Q. Milbank, 1976;54(3):321-37.
6. Newton, R.W.,Webster, P.A.C., Binu, P.S. etal. Psychosocial stress in pregnancy and its relation to the onaetof premature labour. Br.Med.J., 1979;2:411-13.
7. Gray, RH. Stress and reproduction: an epidemiologic perspective. In: Stress and Reproduction. Eds: ICE. Sheppard, J.H. Boublik and J.W. Funder. Serono Symposia Publications from Raven Press. vol. 86, New York, Raven Press, 1992, pp.219-228.
8. Armitage, P. Statistical methods in medical research. Oxford, Blackwell Scientific Publications, 1977; pp. 387-388.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: