
Fazal H. Khan ( Department of Anaesthesia, The Aga Khan University Hospital and Medical College, Karachi. )
Fauzia A. Khan ( Department of Anaesthesia, The Aga Khan University Hospital and Medical College, Karachi. )
Robyna Irshad ( Department of Anaesthesia, The Aga Khan University Hospital and Medical College, Karachi. )
Rehana S.Kamal ( Department of Anaesthesia, The Aga Khan University Hospital and Medical College, Karachi. )
September 1996, Volume 46, Issue 9
Original Article
Abstract
During a period of one year, 126 patients were prospectively audited to analyse complications of endotracheal intubation in a general intensive care unit setting. A total of 62 complications were observed in 48 patients. The most frequent complications during intubation were hypotension and bradycardia. The blockage of endotracheal tubes significantly increased with the duration of intubation. Sore throat was the commonest (22%) complication following extubation. Other complications like stridor and ulceration of mouth and lips which followed extubation were not related to the duration of intubation (JPMA 46: 195, 1996).
Introduction
Endotracheal intubation and mechanical ventilation are performed for potentially life threatening disorders, such as, respiratory failure. In addition, a large number of patients are electively intubated and mechanically ventilated in the postoperative period.
During the last decade prolonged intubation of trachea has commonly been used in the treatment of respiratory failure in intensive care units, but only few reports are available on specific complications ofendotracheal intubation in inechanicallv ventilated patients1,2. This study reports the observation of a prospective audit of complication of endotracheal intubation in an intensive cane unit.
Patients and Methods
All patients above 16 years of age who required orotracheal intubation and mechanical ventilation in the 8 bedded intensive cam unit at the Aga Khan University Hospital with a yearly turnover of approximately 250 to 300 patients, were included in the audit. The duration of study was one year. The proforma designed to document the complication of orotracheal intubation, included indications for intubation, whether it was elective or emergency, type and size of endotracheal tube used and place of intubation, i.e., intensive care unit, operating room, emergency room or the ward and duration of intubation (0-7 days, 8-14 days or 15-21 days). Low pressure high volume cuffed polyvinyl chloride endotracheal tubes were used for intubation in all the patients. The complications were divided into three groups according to the classification of Blanc and Trembley1.
The class 1 complications that occurred during the act of intubation were recorded by anaesthesia residents (2nd or 3rd year trainees in ICU). They included damage to the lips, teeth and upper airway, hypo or hypertension, arrhythmias, aspiration into the lungs and oesophageal intubation. Obstruction of the endotracheal tube, endobronchial intubation and inadvertent extubation were the complications noted while the endotracheal tube was in place and comprised class 2. Class 3 complications were the immediate post-extubation complicalion which were sore throat, any ulceration of mouth and lips, laryngeal oedema/stridor, tongue numbness and unilateral or bilateral vocal cord palsy. These observations were documented by the anaesthesia residents on duty in the Intensive Care Unit daily ata predetermined time of the day. Mechanical complications like pneumothorax etc. were not included in the audit.
For purpose of analysis, the patients were divided into two groups, group A comprising of patients who were successfully extubated and group B were those who expired while being ventilated or on whom tracheostomy was performed. In group A patients, all three classes of complications were noted while in group B only the first 2 classes of complications were noted and analysed.
Results
During one year, 126 patients were audited, of which, 63 (50%) were intubated electively and 63 (50%) under emergency conditions. The mean age of the patients was 47 years (SD±18) and the mean duration of endotracheal intubation was 6 days (SD±5.61). A total of 62 complications were recorded under three groups comprising of complication during intubation, while the endotracheal tube was in place and 6 hours post-extubation. These results are presented in the Table.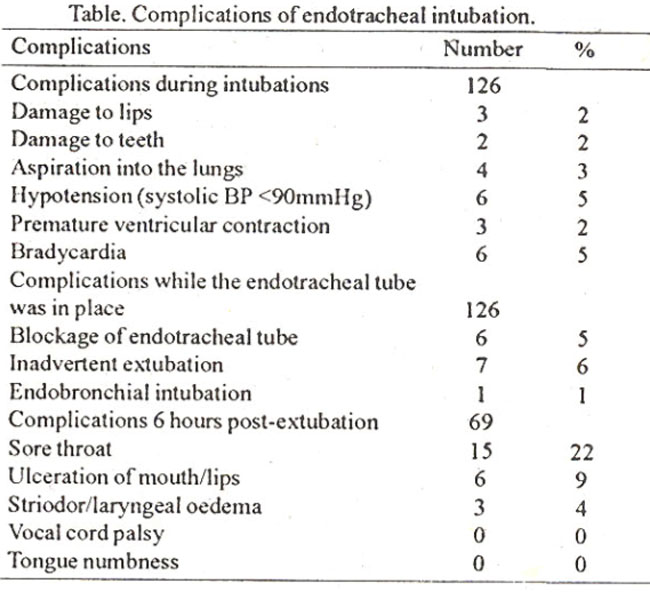
Twenty-four complications were noted during intubations done under emergency circumstances. The most common complications in this group were hypotension and bradycardia (Table). Complication while the endotracheal tube was in place and 6 hours post- extubation were recorded against three sub-groups depending upon the duration of intubation, i.e., whetherbetweenO-7 days, 8-14 days or 15-21 days.
Blockage of the endotracheal tube was observed in 6 (5%) patients. In five instances, the tube was blocked with secretions, while in 1, kinking was the cause. The frequency of blocked tube significantly increased (p<0.05) with the duration of intubation. It was observed once in patients who remained intubated for 0-7 days, twice in each group of patients who remained intubated for 8-14 days (7%) and for 15-2 1 days (12%). Inadvertent extubation was observed in 7 (6%) patients. There was no statistical relationship with duration of intubation and this complication. It was only seen in patients who were breathing spontaneously during weaning from mechanical ventilation. Slipping of the endotracheal tube in one of the main bronchi resulting in endobroncheal intubation was observed only in I (1%) patient. Post-extubation complications were observed in 69 patients who were successfully extubated. Sore throat was the most common complication followed by ulceration of mouth, lips stridor and laryngeal oedema (Table). None of these complications had any relationship with the duration of intubation. Vocal cord palsy either unilateral or bilateral and tongue numbness did not occur in any of the 69 patients.
The outcome of the ventilated patients showed that 70 (55%) were successfully extubated, 50 (40%) expired and 7(5%) required tracheostomy. No relationship was observed between mortality and duration of mechanical ventilation and intubation. One patient who expired was found to have a blocked tube.
Discussion
The exact incidence of complications due to endotrachealintubation in mechanically ventilated patients is difficult to determine and varies widely in published reports1-2. Factors implicated in the etiology of complications include tube size, characteristics of tube and cuff, skill of the physician performing endotracheal intubation, duration of intubation, metabolic and nutritional status of the patient, tube motion and laryngeal motor activity2,3.
1. Complications seen during the act of intubation
Trauma can occur any where from lips to the glottis and is common during routine intubations but the frequency increases in emergency situations since most patients are intubated without using a muscle relaxant. In this study, trauma to lips (3 cases) and teeth (2 cases) occurred in patients intubated in emergency without muscle relaxation. Dentition may be damaged by excessive digital prying and during laryngoscopy. The lips, tongue and buccal mucosa may become entrapped between the blade of laryngoscopc and dentition producing abrasions and lacerations. This can be avoided by applying gentle pressure during laryngoscopy and use of tooth protector.
In the present study, hypotension during intubation was seen in 6 patients. 4 of these were intubated for acute respiratory failure secondaiy to cardiac problems. Reasons for hvpotension in other two cases could not be ascertained. These patients did not receive any drug before intubation. Their hypotension could have been due to the Iaiyngovagal reflex as explained by Blanc and Trembley1 or it could be attributed to the underlying cardiac problem. Transient arrhythmias were observed in 9 patients. Six developed bradycardia with a heart rate of less than 60 per minute, while 3 had multifocal premature ventricular contractions. These patients reverted to sinus rhythm immediately after intubation. Laiyngovagal reflex may be responsible for the bradycardia and larvngosympathetic reflexes leading to increased catecholamine levels could have produced premature ventricular contractions.
Aspirations occurred in fourofourpatients who had full stomach at the time of intubation. It was diagnosed by the presence of regurgitated material in the oral cavity and later confirmed radiologically. Special precautions should be taken in such patients and cricoid pressure should always be applied. In all of these patients cricoid pressure could not be applied because of non-availability of help in emergency conditions. Aspiration can also occur when the endotracheal tube is in place because of poororal suctioningoraccidental deflation of endotracheal tube cuff. There is also evidence that prolonged intubation of trachea (8 hours or more) may impair the ability of the larynx to sense foreign material for several hours after extubation, even though the patient is fully awake3 and patients can aspirate after extubation. Recovery of normal reflex function in some patients does not occur uptil 4-8 hours following extubation and during this period patients arc vulnerable to aspiration.
2. Complications while the ëndotracheal tube was in l)lacC
Obstruction of endotracheal tube occurred in 6 patients. This occurs due to secretions, blood, kinking or inward collapse of the tube lumen by pressure of the inflated cuff. In one patient, the tube was kinked in the phaiynx, while in others, it was blocked with secretions. One instance of blockage due to secretions was between 15-21 days. Early diagnosis with inability to pass a suction catheter orabsence of expiratoty sounds on auscultation should alert the physician immediately to this complication. Indications for tube change includes tube cuff failure, obstruction or change in size of tube to allow bronchoscopy or to decrease ainvay resistance. It is generally recommended that the endotracheal tube should not be changed prophylactically4. However, based on our finding, we recommend to change the endotsacheal tube every seventh day.
Inadvertent extubation is an unplanned extubation. It was seen in 7 patients. All these patients were on a 1-piece circuit prior to extubation without any sedation or muscle relaxation. Little et al5 identified several risk factors for accidental extubation in neonatal and paediatric patients which included factors like inadequate sedation, improper tube fixation and changing the position of patient. In this study accidental extubations occurred in two restless patients who pulled their tubes out and in rest of the cases due to excessive movement associated with change in the position of the patient.
Endobronchial intubalion was seen in one patient where the tube had inadvertently slipped into the bronchus during mechanical ventilation. This complication can occur at the time of intubation or during ventilation. If the tube is improperly fixed, it can descend into a bronchus as a result of the weight of the attachment, due to low positioning of during suctioning. Auscultation of chest at regular intervals and radiological examination is recommended in doubtful circumstances6. Inadvertent endobronchial intubation can be minimized by calculating the proper tube length for every patient then noting the centimeter marking on the tube at the point of fixatioing daily.
3. Complications 6 hours post-extubation:
Sore throat occurred in 9 patients who remained intubated for 0-7 days, in 3 who were intubated for 8-14 days and 3 who remained intubated for 15-21 days. Sore throat is so coninion following extubation that some authors refuse to classify it as a complication7. The reported incidence of post-intubation sore throat varies from 6-7%8. It results from mechanical irritation and usually resolves with 48-72 hours. The cuff tracheal wall contact area also influences the incidence of sore throat. In one study when the cuff tracheal contact area was 20 mm the incidence of sore throat was 12% incomparisonwith 26% when this area was 37mm. It was also demonstrated that incidence of sore throat increases if lignocaine ointment is used to lubricate the tube but others have failed to demonstrate this relationship9,10. Ulceration of mouth and lips occurred in 9% of the patients. It occurs as a result of tube pressure on one side of the mouth for more than 48 hours11. The endotracheal tubes fixation site should therefore be changed every day to avoid this complication.
Stridor is usually evident within 1-2 hours following extubation and the most conunon cause is laryngeal oedema. Sometimes it is so severe that re-intubation is required. Post extubation stridor was observed in 3 patients ventilated for 0-7 days. Reintubation was required in two patients. No patient ventilated for 15-21 days had post extubation latyngeal oedema. Bishop and Fink12 also reported that prolonged periods of endotracheal intubation doesn’t seem to increase the incidence or severity of rnucosal oedema. Prophylactic administration of methyl prednisolone before extubation after prolonged intubation, may not be effective. The development of laryngeal oedema can be prevented by gentle and a traumatic intubation, by keeping the movement of head to a minimum and by avoiding over inflation of tube cuff.
References
1. Blanck. UP. and Trcmhley, NAG. The complications oftracheal intubation: A new classification with a review of the literature. Anesth. Analg,, 1974;53;202-213.
2. Gaynor. E.B. and Greenberg, SB. Untoward sequelac ofpnolongcd intubation. Laryngoscopc. 1985;12:1461-1467.
3. Kastanos, N., Estopa, MR., Marin, PA. et al. Laryngotrachcal injury due to endotracheal intubation: Incidence evolution and predisposing factors, A prospective long tarm study. Crit Care Med.. 1983; 11:362-367.
4. Burgess, G.E.. Cooper. J.R.,Manino, Ri. et al Laryngeal competence after tracheal extubatton Anacathesiology. 1979;51 :73-77.
5. Mitchell, K. Airway management and intubation. In’ Jesse B Ilall, Gregory, A Schmidt. Lawrence, D.H.. Wood cds. Principles of critical care, New York. McGraw Hill, 1992, pp. 123.134.
6. Little, L.A., Koening. J.C. and Ncwth, C.J.L. Factors affecting accidental extubation in neonatal and paediatnic intensive care patients. Cot Care Med,, 1990;18:163-165
7. Conrardy, PA.. Goodman, L.R., Laingc, F ct al Alteration ofcndotrachcal tube position. Cnit Care Mcd , 1976;4:5-12
8. Barson, SB. and Kohlmoos, H W. Laryngeal scquelae of endotracheal anaesthesia. Ann. Otol. Rhinol. Laryngol., 1951 ,60:767-792.
9. Harisell, C.J. and Stephen. C. R. Incidence of sore throat following endotracheal intubation. Can. J. Anaesth,. 1994; 11:307 312.
10. Loeser, E.A., Kaminaky. A., Diaz, A. et al. The influence ofendotnacheal tube cuffdesign and cuff lubrication on post. operative sore throat. Anaesthcsiologv. 1983;58:376-379.
11. Stock, MC. and Downs, 3 B. Lubrication of tracheal tubes to prevent sore throat from intubation. Anacsthesiology, 1982;57(5):41 8.420.
12. Dixon. T.C., Sando, M.J.\\\\V, Botton, 3M et at. A report of 342 cases of prolonged endotracheal intubation. Mcd. 3. Aust., 1968;2: 529-533
13. Bishop. M.J.. Weymuller, E.A. and Fink, BR. Laryngeal effects of prolonged intubation. Anesth. Analg., 1984;63:33 5-342.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: