
M.A. Rahim Khan ( Departments of Radiology, Shaikh Zayed Postgraduate Medical Institute, Lalsore. )
Anwaar A. Khan ( Departments of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Farzarta Shafqat ( Departments of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
September 1996, Volume 46, Issue 9
Original Article
Abstract
Diagnostic accuracy of ultrasonography and cholangiography (ERCP/PTC) was compared in determining the site and nature of obstruction in Obstructive jaundice. Ultrasound was performed in 50 patients with clinical diagnosis of obstructive jaundice. All patients subsequently underwent ERCPIPTC and/or surgery. ERCP was performed in 38 and FTC in 15 patients. The positive predictive value for the site and etiology of obstruction by ultrasonography was 94% and 86% respectively. In comparison, the cholangiography (ERCPIPTC) had positive predictive value of 100% in site and 98% in etiology. High degree of accuracy and non-invasiveness makes ultrasound as the primary radiological tool in the differential diagnosis of obstructive jaundice. ERCP is the gold standard for determining the precise level and cause of obstruction. FTC adds further to ultrasound based diagnosis of obstructive jaundice particularly in proximal obstruction and in ERCP failure (JPMA 46: 188, 1996).
Introduction
Ultrasound is an established component of myriad of techniques used in the differential diagnosis of obstructive jaundice (03). It is simple, cost effective and non-invasive procedure that can be repeated as desired. Coupled with clinical and biochemical information, it is possible to predict the site and cause of obstruction with high degree of precision1-4. Percutaneous transhepatic cholangiography (PTC) is a time tested procedure employed in the investigation ofobstructivejaundice despite its significant morbidity. Since the early 1980s, FTC is gradually replaced by Endoscopic retrograde cholangiopancreatography (ERCP) because it has potential therapeutic use. A definite role of PTC however, still exists in patients who have contraindications to ERCP, have difficult cannulation by ERCP or there is proximal biliary obstruction. ERCP has achieved credence in the recent years both as a diagnostic and therapeutic procedure in the management of obstmctive6jaundice and is the gold standard for investigation of OJ5,6. The advantages of ERCP are its ability to visualize and biopsy ampullary lesions, demonstration of biliaiy and pancreatic ducts and a therapeutic potential. The present study compares the diagnostic accuracy ofultrasonography and cholangiography (ERCP/PTC) in ascertaining the site and nature of obstruction.
Patients and Methods
The study is based on 50 patients treated from April, 1994 to October, 1995 with the clinical diagnosis of obstructive jaundice at the Shaikh Zayed Postgraduate Medical Institute, Lahore, a tertiary referral centerf orbiliary problems. Ultrasound was performed by a consultant radiologist in all patients using a real time GE scanner RTX 200 model equippedwith 3.5 MHzconvex transducer. Liver, gallbladder, intraliepatic ducts, common bile duct and pancreas were evaluated. The criteria used for the diagnosis of biliarv obstruction by ultrasonography were dilated intrahepatic bile ducts or common bile duct diameter of>8 mm. A diameter of 10 mm was considered upper limit of normal in postcholecystectomy patients7. PTC was performed by a radiologist using percutaneous transhepatic approach by chiba needle (22G). ERCP was performed by one of the gastroenterologists (AAK). Olympus endoscope TJF10 or Olympus video endoscopc TJF130 was used by a routine method. Cannulation of CBD was done in all cases with elucidation of obstructive lesion. Thirty eight patients had ERCP and 15 had PTC (3 patients had both ERCP and PTC).
The diagnosis was classified as: the site of obstruction was defined as proximal (in the porta hepatis orsuprapancreatic part of CBD) or distal (in the intrapancreatic orintraduodenal part of CBD) by ultrasonic evaluation and the cause of obstruction was reported neoplastic or non-ncoplastic calculi/strictures (benign or postoperative).
The ultrasound diagnosis was recorded before the establishment of final diagnosis by another investigation, i.e.,
ERCP, PTC, FNA and/or operative biopsy (24 patients). The ultrasound and cholangiographic diagnoses were compared with the final diagnoses and results were calculated to determine the diagnostic accuracy of ultrasonography and cholangiography.
Results
The etiological diagnoses of these patients are given in Table.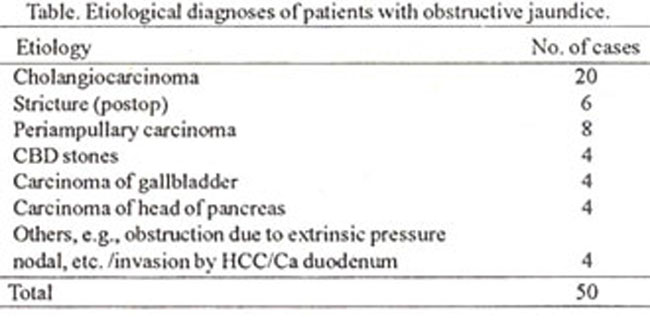
Ultrasonogram provided a correct diagnosis of proximal obstruction in 23 of 26 cases and distal obstruction in all 24 cases. The overall positive predictive value for the site of obstruction was 94%. Ultrasonograrn reports were wrong in locating the site of obstruction in three patients (6.0%). These included patients with a nodal mass, periampullary carcinoma and cholangiocarcinoma causing lower end obstruction. Sonographic evaluation of the cause of obstruction gave a positive predictive value of 100% in calculus disease and 85 % (39/46) non-calculus disease. Overall positive predictive value for the cause of obstruction was 86%. Forty-six patients had a non-calculus lesion that included tumors and strictures (benign and postop). The etiology was correctly determined by ultrasound in 39 patients. Ultrasound provided correct diagnosis of carcinoma of the gall bladder in 4 cases with a positive predictive value of 80% and wrong diagnosis of carcinoma of the gallbladder causing proximal obstruction in a patient who had cholangiocarcinoma. Ultrasound diagnosis of carcinoma of the head of pancreas was correct in four patients with positive predictive value of 67% and wrong in two cases who had periampullary carcinoma and cholangiocarcinoma.
Periampullary carcinoma was confirmed in 8 patients by operation and/or ERCP/biopsy. The ultrasound diagnosis was correct in five of them with positive predictive value of 83%. Twenty patients had a confirmed diagnosis ofcholangiocarcinoma by operation and/or ERCP. The ultrasound provided correct diagnosis in 17 with a positive predictive value of 89%. The diagnosis of benign strictures which included postoperative (iatrogenic) was made in 6 cases with a positive predictive value of 100% as confirmed by ERCPfPTC and laparotomy. Of four cases, 2 had obstruction due to extrinsic pressure by nodal mass and inflamed, distended gall bladder. The other 2 showed invasion of CBD by hepatocellular carcinoma (HCC) and carcinoma of the duodenum. Ultrasound provided correct diagnosis in three cases with positive predictive value of 75%.
Three cases needed PTC besides ERCP to demonstrate the biliary tree proximal to the site of obstruction. There were 22 proximal and 28 distal obstructions. Cholangiograms (ERCP/PTC) ascertained correctly the site of obstruction in all 50 cases with positive predictive value of 100%. ERCP/PTC provided correct diagnosis in 49 cases (45 non-calculus, 4 calculus) with a positive predictive value of 98% and made wrong diagnosis of calculus lesion (2%) in a patient who had cholangiocarcinoma.
Discussion
Ultrasonography, ERCP and PTC are common armamentarium for the detection of site and cause of obstruction in OJ. All 50 cases of obstructive jaundice reported here showed valying degree of dilatation of intrahepatic biliaty ducts or CBD diameter of>8 mm. It is prudent for surgical planning to establish the level and etiology of obstruction in the biliazy system. Overall positive predictive value of ultrasound for the level of obstruction in this series was 94%and forthe cause of obstruction 86%. Positive predictive values for the site and nature of the obstruction were as 94.3% and 89.9% by Tandon et al, 90.9% and 95.2 by Dwivedi et al and in 72% and 41% of cases by Khandelwal et al9 respectively. Rigautset al correctly defined the cause of obstruction in71%ofductat stones and in 90% of tumoral bile duct obstruction10.
In this series, the accuracy of cholangiography in delineating the site and cause of obstruction was 100% and 98% respectively. Similar results were reported by other11,12. Dwivedi etal showed that ERCPIPTC could correctly change the site and nature of obstructionin 5 (17.9%) patients and in remaining 23 patients it did not add any additional information over ultrasound findings6. Dixit et al demonstrated that US, PTC and ERCP correctly ascertained the cause of obstruction in 55%, 63% and 67% of cases respectively13, while Huang et al. demonstrated accuracy of US and ERCP in 85% and 95% of cases respectively14. In the present series cholangiography (ERCPIPTC) correctly changed the site of obstruction in 3 cases (6%) and cause of obstruction in 7 cases (14%). It did not add any additional information over ultrasound findings in the remaining 43 cases (86%).
Acknowledgements
We are thankful to Miss Yaamina Rahim for helping in the preparation of the manuscript and Mr. Asghar Ali Anjum for formatting.
References
1. Malini, S. and Sabel, J. Ultrasonography in obstructive jaundice. Radiology, 1977,123:429-33.
2. Lee, T.G., Henderson. S.C. and Ehrlich, R Ultrasound diagnosis of a common bile duct dilatation. Radiology, 1977;124:793-7.
3. Honickman, S.P., Mueller, P.R., Wittenburg. J. et al Ultrasound in obstructive jaundice: Prospective evaluation of site and cause. Radiology, 1983; 147:511-5.
4. May, OR., James. EM, Bender, CE Diagnosis and treatment of jaundice. Radiographics, 1986,6:847-90.
5. Dwivedi, M, Acharya. S.K., Nundy, S et al Accuracy of abdominal ultrasonography and the role of a second investigation in surgical obstructive jaundice. Gastroenterol Jpn., 1989,24:573-9.
6. Salazar S., Usechc. E. and Vetencourt, R Ultrasonography in the differential diagnosis of obstructive jaundice: Comparison with endoscopic retrograde cholangiopancreatography. GEN, 1993,47:73- 7.
7. Steven, MC. and Alfred, BK. Biliary sonography. Radiol. Clin. North Am., 1991;29:1171-98.
8. Tandon, B.N., Rana, S., Acharya, S.K. et al Bedside ultrasonography. A low-cost definitive diagnostic procedure in obstructive jaundice. J. Clin. Gastroenterol., 1987,9:353-6.
9. Khandelwal, N., Sun, S., Katariya, S. et al, Ultrasound in obstructive jaundice. Indian J. Gastroentcrol., 1990;9:51-3.
10. Rigauts, H., Marchal, G,, Van-Steenbergen, W. er al. Companson of ultrasound and ERCP in the detection of the cause of obstructive biliary diserse. Rofo-Fortscher. Geb Rontgenstr. Neuen. Bildgeb. Verfahr., 1992;156:252-7.
11. Gold, R.P., Casarella, W.J., Stern, 0. et al Transhepatic cholangiography: The radiological method of choice in suspected obstructive jaundice. Radiology, 1979;133:39-44.
12. Koenigsberg, M., Wiener, SN. and Walzer. A. The accuracy of sonography in the differential diagnosis of obstructive jaundice: A comparison with cho. langiography. Radiology, 1979;133:157-65.
13. Dixit, V.K., Jam, A.K,, Agrawal, AK. et al Obstructive jaundice- A diagnostic appraisal. 2. Assoc. Physician India, 1993;41:200-220.
14. Huang, JQ., Bao, X. J. and Lu, XH. The common causes and differential diagnosis of malignant jaundice Chung Hua, Nei. Ko Tsa. Chih.. 1993;32:400-4.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: