
Haruko Akatsu ( Brown University Medical Center, Providence, RI, USA. )
Asif Aslam ( 24, Old Clifton Road, Karachi. )
September 1996, Volume 46, Issue 9
Original Article
Abstract
The prevalence of hypertension and overweight/obesity was studied among 151 women overage 25 in an underprivileged area in Karachi. Two blood pressure measurements were recorded and elevated readings were repeated after 2 days. Body Mass Index (BMI) was used to define overweight and obese. Waist hip ratio (WHR) was calculated to distinguish between the upper and lower body type obesity. The prevalence of hypertension was 17 percent (25 women), including 15 out of 21 subjects on anti-hypertensive medication who were still hypertensive. Forty-two percent were overweight and 8 percent were obese. Most of these overweight/obese women had an upper body type obesity, which is associated with increased cardiovascular risk. Possible suggested interventions include diet education and weight monitoting by the community health workers (CHWs) using an individualized weight card. These interventions can be added on to the already established primary health care (PHC) system addressing mother and child health (MCH) problems (JPMA 46:191,1996).
Introduction
Different regions of the world are cunently undergoing a change from a pre-dominance of the acute infection and deficiency affecting children, to a predominance of the chronic diseasesOf adults. This is termed the “epidemiological transition”1-5. The care of patients with chronic diseases can be life-long and expensive and overwhelm the health care system in developing countries.
The present study documents the extent of one such chronic problem ma low income squatter settlement or “katchi abadi” in Karachi. For this purpose, hypertension and overweight/obesity were used as easily measurable indicators of chronic health problems of adults.
Subjects and Methods
(A) Subjects
It is estimated that close to 40 percent of Karachi’s rapidly expanding population is living in the under-privileged conditions of Katchi abadis6. The Aga Khan University’s Department of Community Health Sciences (AKU-CHS), Karachi. has been involved in the development of a prototype of primary health care (PHC) in five such katchi abadis out of which Chanesar Goth war chosen for the study site as it ranks middle in terms of infant mortality mte(IMR) and income.
According to base-line information as of 1991, average population in the selected part of Chanesar Goth was 10,840 and the IMR was 66.7, which has shown decline subsequent to the development of a Primary Health Care (PHC) programme in the area. The population is predominantly Muslim, with sizeable number of Christians and Hindus, representing the three major religious groups in Pakistan. Majority of the population has Sindhi as its mother tongue, with some Puajabi and Urdu speaking people. The average family has 7.2 members and an average monthly income of Rs.l5657.
The project area in Chanesar Goth is divided in 12 sectors, each consisting of about 120 households. Of these 12 sectors, sector 8 was chosen as the study community because it ranked middle among the sectors in terms of an average monthly income. The total population in sector 8 was 1307 of which 201 (15.4 percent) were children aged under 5. The population to be studied consisted of all the 202 females over age 25 living in sector 8 at the time of the study.
(B) Method Protocol
All the potential subjects were visited at their homes accompanied by female CHWs working with this study community. The CHW explained the nature of the study to the subjects and informed consent was obtained verabally.
The investigators recorded the height, weight and blood pressure of the subject. Two blood pressure measurements were recorded, once, while the subject was sitting and the second time while the subject was lying down. After the first blood pressure measurement, the subject was instructed to raise her arm above the shoulder level for at least 2 minutes to avoid any venous congestion and erroneous elevated reading. In the interval between the two readings, the community health worker(CHW) asked the following five questions from the subject: (a) Current pregnancy status, (b) use of any hypertensive drugs, (c) use of birth control pills, (d) use of tobacco and(e) regutaruse of pan. Afterthis, the waist and hip circumferences were measured for those who fell into the overweight/obese category’ as defined below.
If one or both of the two blood pressure readings were in the mild, moderate, severe, or isolated systolic hypertension range and if that individual was not on any anti-hypertensive medication, the investigator returned for a second home visit to repeat blood pressure measurements. At least two days were kept between the initial visit and the re-visit. If the subject still manifested a high pressure reading, she was referred for further evaluation.
Calculation
Body mass index (BMI) was calculated as weight/height2 (kg/m2). Waist hip ratio (WHR) was calculated as waist circumference/hip circumference x 100%. Average of systole was caLculated as average of the two systolic pressure readings (sitting and lying down) and that of diasytole as an average of the two diastolic pressure readings (sitting and lying down). Readings obtained during the initial visit were used foranalysis.
Definitions
Overweight/obesity were defined using the BMI8: BMI 23-29 Overweight; BMI >29 obese. Hypertension was defined as9: diastoLic pressure, <85 : Normal blood pressure. 85-89: high normal blood pressure, 90-104: mild lwpcrtension, 105-114: .moderate hypertension, >1= 115: severe hypertension.
Systolic pressure (when diastolic pressure is <90):
<140: normal blood pressure,140-159: borderline isolates systolic hypertension and >/= 160: isolated systolic hypertension.
The average of two blood pressure readings (sitting and lying) during the first visit was used to categorize the subject’s blood pressure status into hypertension (including mild. moderate, severe, borderline isolated systolic and isolated systolic hypertension and normal blood pressure.
Statistical Procedures
The Chi-Square was caLculated by the Statistical Package for Social Sciences (SPPS). The p values of less than 0.05 were considered to be statistically significant.
Results
Of 202 potential subjects, measurements were taken for 151 women. Data on 5 1 potential subjects could not be collected due to these subjects working outside the house during the day and refusal to participate in the study. Thirteen women were pregnant at the time of this study and were therefore excluded. Of 151 women, 78% were normotensive. 11% had mild and 6% borderLine isolated systolic hypertension. Five percent subjects had high normal blood pressure. Data collection rate was higher among youngerwomcn (tinder age 45) than that of older women (over age 45) (Table I). Nearly 50 percent of the subjects were aged between 26 and 35 years (Table I).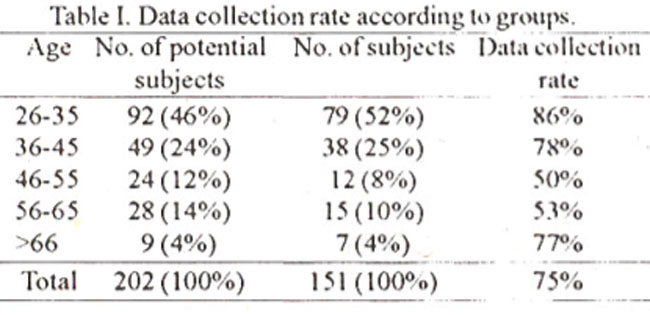
The mean age of the subjects was 40 years. The height (Mean±SD) was 153.5+6 cm. (range 126 cm to 169cm). The weight (rnean±SD) was 54.3+12.6 kg. (range was 26 kg to 105 kg). The minimum BM I was 12 and the maximum was 44 (mean BMI 23 and standard deviation 5.1). Forty-two percent women were over- weight and 8 percent were obese.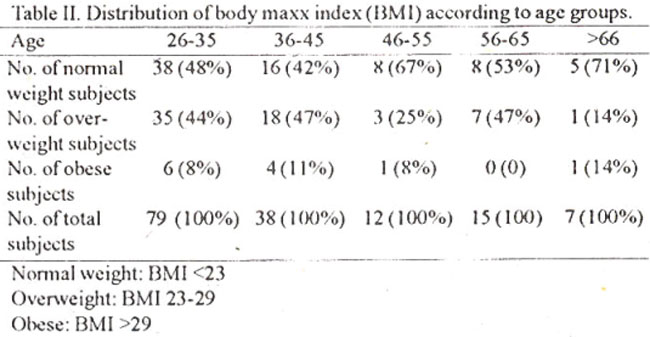
Table II shows the distribution of BMI category according to age. The prevalence of overweight/obesity was higherarnong youngerwomen: prevalence of54 percent in the age group under 45 and that of38 percent in the age group over 45. Almost all the subjects revealed upper body type obesity which is characterized by the WHR of greater than 80: one person had WHR between 71-80, 23 between 81-90, 19 between 91-100 and 2 persons above 100. The WHR range was from 72 to 161.
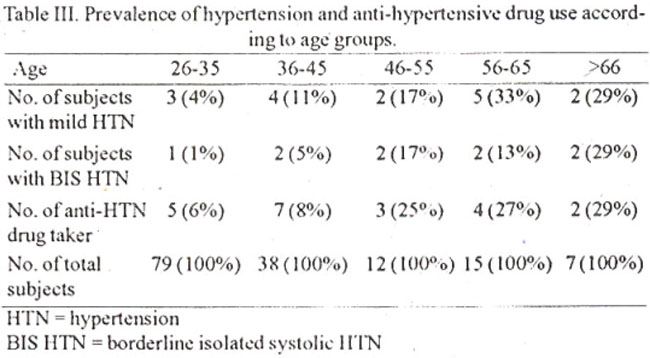
Table III shows the prevalence of hypertension and anti hypertensive drug use in various age groups. Both hypertension and use of anti hypertensive drugs was higher in women above the age of 45 years.
Discussion
The prevalence of hypertension among the study subjects was 17 percent (25 people), which included 15 out of 2 1 subjects already on anti-hypertension medication (TabLe III). If one includes the 6 women whose blood pressure were within the normaL range at the time of this study but were taking anti-hypertensive drugs, the prevalence of hypertension will be 21 percent.
The prevalence of hypertension increased significantly according to increase in age: from 5 percent among those aged 26 and 35 to 43 percent for those aged 46 to 55 and to 57 percent for those over 65. About 50 percent of the present study sample was aged between 26 and 35 (Table III).
National data on the prevalence of hypertension in Pakistan for comparison to this current finding are not available. A study done in 1974 among 322 shopkeepers and clerks in Lahore revealed that 24 percent of the sample population was found to be hypertensive. Another study in Karimabad, Karachi, a middle class urban field site of the AKU-CHS, revealed that the prevalence of hypertension among women over age 35 in 1990 was 25 percent10.
The findings of this study indicate that chronic conditions such as hypertension arc no longer negligible in the study community. A report of a WHO Scientific Group states that:
“It had taken several decades to realize that arterial hypertension is a frequent and almost ubiquitous health disorder, prevalent in both developed and developing countries11. Even if hypertension is usually asymptomatic and does not in itself interfere with daily activities, itis a significant risk factor for chronic disabling condition such as coronary heart disease and cerebrovascular disease. Thus the control of the blood pressure will be an important health issue in the study community.
A significant number of the study subjects were above the normal weight and were categorized either overweight or obese. Since mortality and morbidity increase with increasing weight, weight control seems to be one of the major problems in the study community;
In this study, 44 out of 45 women had a WHR greater than 80. which is characteristic of upper body type obesity. Usually upper body type obesity with the accumulation of fat in the abdominal region is seen among men than women. On the other hand, lowerbody type obesity with fat accumulation in the hips, gluteal regions and extremities is more typical of women. Studies have shown that upper body’ obesity is associated with increased cardiovascular risk12-14. A 12 year study of 1462 women found the WHR to be a better predictor of inyocardial infarction, angina pectoris, stroke and death than any other anthropometric measurement obtained15. In these studies, the cardiovascular risk increased significantly when the WHR was greater than 80. In this community study one not only finds a high prevalence of overweight/obesity. but one sees the kind of overweightJobesity which carries more significant health risks.
There needs to be an investigation into the etiology for such distended abdomen nor the reasons for observing male-type or upper body type obesity among women. A computed tomography study indicates that a high WHR is associated with a high proportion of intra-abdorninal fat1 Whether or not that is the case with the present study subjects needs to be further investigated.
The association between hypertension and 3 variable (the use of tobacco, regular use of pan and the use of birth control pills), which were suspected to, increase the blood pressure, was additionally studied. In the present stud, no statistically significant association was detected for an of these variables, however, the association cannot be eliminated because of limitations in the sample size of this study. In fact. increased prevalence of hypertension was observed among tobacco users, regular pan users, birth control pill users and overweigh/obese individuals.
Acknowledgement
This study was carried out during the author’s affiliation with the Department of Community Health Sciences, Aga Khan University, Karachi where the first author was a visiting international student and the second author a faculty member. We wish to acknowledge the support of Professor J. Bryant. Dr. Lubna Baig and the Staff and Community Health Workers of the Chanesar Goth Primary Health Care Center.
References
1. Beevers, D.G. and Prince, J.S. Some recent advances in non- communicable diseases in the tropics. Hypertension: An emerging problem in tropical countries. Trans. R. Soc. Trop. Med. Hyg., 1991;85:324-326
2. Bicknell, W.J. and Parks, CL. As children survive: Dilemmas of aging in the developing world. Soc. Sci. Med., 1989;28:59.67.
3. Caldwell, J.C. Health transition: The cultural, social and behavioral determi. nants of health in the third world. Soc. Sci. Med., 1993; 136, pp. 125-135.
4. Manton, KG. Theglobal impact of non-communicable diseases; estimates and projections. World Health Stat. Q.. 1988;41 :255. 266.
5. Nissinen, A., Bothing, S., Granroth. H. ct al. Hypertension in developing countries. World Health Sci. Q., 1988;41 :141-154.
6. Kool, MG., Verboom, D. and Linden, J.J. Squatter settlements in PakistanLabore, Vanguard Books Ltd., 1988. pp. 23.24.
7. Department of the Community Health Sciences, The Aga Khan University. US-AID Matching grant for Urban PHC Program (Phase II). Report for the period July 1, 1990.June,30, 1991, 1991.
8. U.S. Department of Health and Human Services. The Surgeon General’s report on Nutrition and Health, US Government Printing Office, 1988;p. 284
9. Andreoli, TE., Bennett, J.C., Carpenter. CC. et al Ed. Cecil Essentials of Medicine. 3rd edition, Philadelphia, W.B. Saunders Co., 1993, p 230.
10. Ahmad, I. Hypertension among shopkeepers and clerks. J. Pak. Med. Assoc.. 1976;26:180-185.
11. Department of the Community Health Sciences, The Aga Khan University. (1992) Urban Primary Health Care Program Report for the Period July 1. 1991-June 30, 1992. Karachi, Aga khan University, 1992.
12. Report of a WHO Scientific group (1983). Primary prevention of essential hypertension. WHO technical report series 1983, p 5.. 686.
13. Folsom, AR.. Kaye, S.A., Sellers, TA. et al. Body fat distribution and 5-year risk ofdeath in older women. JAMA., 1993;269:483-4$ 7.
14. Krotkiewsk, M., Bjorntorp, P., Sjostrom, L. et al Impact of obesity on metabolism in men and women: importance of regional adipose tissue distribution. J. Clin.Invest.. 1983,72:1150-1162.
15. Larsson, B.. Svardsudd, K., Welin, L. et al. Abdominal adipose tissue distribution, obesity and risk of cardiovascular disease and death; A 13 years follow up of participants in the study of men born in 1913 Br.Med J. 1984;288: 1401-1404.
16. Lapidus, L.. Bengtsson, C., Larsson, B. et al. Distribution of adipose tissue and risk of cardiovascular disease and death: 1-12 year follow-up of participants in the population study of women in Gothenburg. Sweden. Br. Med J., 1984;288. 1957-61.
17. Ashwell, NI., Cole, T.J. and Dixon, AK. Obesity New insight into the anthropometric classification of fat distribution by computed tomography Br Med. J., 1985,290:1692-169.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: