
Arshad K. Butt ( Departments of Gastroenterology and Radiology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Anwaar A. Khan ( Departments of Gastroenterology and Radiology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Altaf Alam ( Departments of Gastroenterology and Radiology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Shafiq Ahrnad ( Departments of Gastroenterology and Radiology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
S. Waqar H. Shah ( Departments of Gastroenterology and Radiology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Farzana Shafqat ( Departments of Gastroenterology and Radiology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Altaf Baqir Naqvi ( Departments of Gastroenterology and Radiology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
July 1998, Volume 48, Issue 7
Original Article
Abstract
Hepatocellular carcinoma is one of the most common malignancies world wide. We present data on 76 patients admitted to the Shaikh Zayed Hospital. Mean age was 52.2±11.3 years. Eighty six percent were males and 14% females. Eighty-six percent patients had underlying cirrhosis documeted on ultrasound examination. Seventy-five percent were positive for anti HCV, 10% for HBsAg positive, 10% for both HBsAg and anti HCV and 5% cases had negative viral serology. Main clinical features were abdominal pain, weight loss, jaundice, hepatomegaly and ascites. Forty- three percent patients were Child-Pugh class A, 30% class B and 13% class C and 14% were non cirrhotic. Mean alfa fetoprotein levels were 142±155 ng/ml (range 2.7 to 1470). Diagnosis of hepatocellular carcinoma was established in 60 patients by fine needle aspiration biopsy under ultrasound guidance.Two patients died afterbiopsydue to uncontrollable bleeding. Fifty-four percent patients had a solitary lesion and 46% had multifocal or diffuse lesions. The average size of lesion was 7.8x8,1 cm. Twenty-two patients received intralesional alcohol injection. Fifty-four percent of these with a tumor size greater than 8cm died during follow up. The major cause of death was liver failure in 8 patients and fatal bleeding occurred in 4 patients. Hepatocellular carcinoma has a high prevalence in middle a8ed males with a strong association with anti HCV positive cirrhosis. Patients with a tumoursize greaterthan 8 cm.have a poor response to intralesional alcohol Injection (JPMA 48:197, 1998).
Introduction
Hepatocellular carcinoma (HCC) is among the l() most commonmalignancies in the world1. lnPakistanprcvalcnceof HCC varies from 3.7% of all malignant tumors2to 16%3.
Epidemiological and experimental studies have demonstrated a convincing role of chronic infection with hepatitis B (HBV) and hepatitis C (HCV) on a background of cirrhosis as major risk factors for the development of hepatocellular carcinoma4,5. In Pakistan. carrier rates for HBsAg and hepatitis C are reported to be 10-16% and 2-6% respectively6-9. These figures ate alarmingly high and stress the need for epiderniological studies to. better delineate the relative roles of these two potentially carcinogenic viruses in the etiology of hepatocellular carcinoma in our population.
Hepatocellular. carcinoma is difficult to treat and has a poor prognosis. Surgery is successful in only a small number of patietns. Systemic chemotherapy has been found to be ineffective, Intra arterial chernoembolization, lipoidal infusion into hepatIc artery, intralesional alcohol injection, liver transplantation and recently gene therapy are being evaluate10,11. Since our patients have HCC developing in cirrhotic livers with compromised hepatic reserve, surgical excision is usually not possible. Similarly selective intraarterial drug delivery systems and the novel gene therapy are not available in our institutions. With these limitations, percutaneous ethanol intralesional injection therapy (PET) is considered a viable palliative option for the vast majority of our patients. This study reports clinical, epidemiological features, serology, laboratory findings and the response of tumor to percutaneous absolute ethanol injection under ultrasound guidance as a palliative procedure.
Patients and Methods
Seventy-six consecutive patients with HCC admitted to the Department of Gastroenterology and Hepatology, Shaikh Zayed Hospital, Lahore between September 1994 and November 1996 were enrolled in this study. Complete database on clinical and labratoiy parameters was obtained for all patients. Twelve of these were referred from other institutions. All patients had estimation of serum alfa-fetoprotein levels and ultrasound examination of abdomen. Histological diagnosis of HCC was established by fine needle aspiration cytology (FNAC) using 23 gauge lumbar puncture needle in 60 patients12,13. In 16 patients diagnosis was made on ultrasound appearance and elevated alpha- fetoprotein levels. FNAC could not be done in these cases because of impaired clotting profile nonresponsive to treatment. Diagnosis of cirrhosis was established on clinical features of portal hypertension and cutaneous signs of chronic liver disease when present, impaired liver function tests, low serum albumin, impaired clotting profile, irregular liver surface detected on ultrasound and ratio of transverse caudate lobe to transverse right lobe width greater than 0.6514. A liver biopsy was not considered absolutely essential for diagnosis of cirrhosis in our series.
Hepatitis B surface antigen (HBsAg) was tested with SERODIA-HBs (a Reverse Passive Hemagglutination Test kit manufactured by Fujirebio Incorporated, Japan), Anti HCV was tested with Murex anti-HCV (Version Ill) which is an ELISA based technique utilizing antigens from the putative core (C, structural), protcase/helicase (NS3, non-structural), NS4 (non-structural) and replicase (NS5, non-structural) regiona of the virus. (The kit is commercially marketed by Murex Diagnostic Limited, Dartford, England).
Twenty patients were considered ineligible for percutaneous ethanol intralesional injection therapy (PET) due either to persistent encephalopathy, multicentric tumor, grossly impaired clotting profile, massive ascites that precluded proper placement of needle in the tumor or marked debilitation. Thirty four patients refused alcohol injection while 22 patients consented for intralesional alcohol injection using 100% ethanol under ultrasound guidance. A 22 gauge fine needle was used to inject alcohol. initially pure alcohol was used but due to severe pain experienced by patients that limited volume of alcohol injected, 2% Xylocainc was mixed with ethanol in a dilution of 1:25 and injected into the tumor mass upto the limit of tolerance of each patient. Total volume of alcohol injected was calculated by the formula v 4/3xxx (radius in cm + 0.5 3)15. . The calculated volume was injected in weekly sessions till completion of therapy. All patients were then followed in out patients departemnt every 12 weeks. Informed consent was obtained from all patients.
Response to treatment was evaluated by survival rates and reduction in tumor size on ultrasound examination repeated every 3 months. The study was approved by the institutional review board.
Statistical analysis
Qualitative variables are reported as frequencies or percentages. Quantitative data are reported as mean±S.D. Logistic regression analysis was used to identify clinical and laboratory parameters predicting response to PET. A p value <0.05 was considered significant for allanalyses.
Results
A total of 76 patienls were included in this study. Their demographic and clinical data is presented in Table I.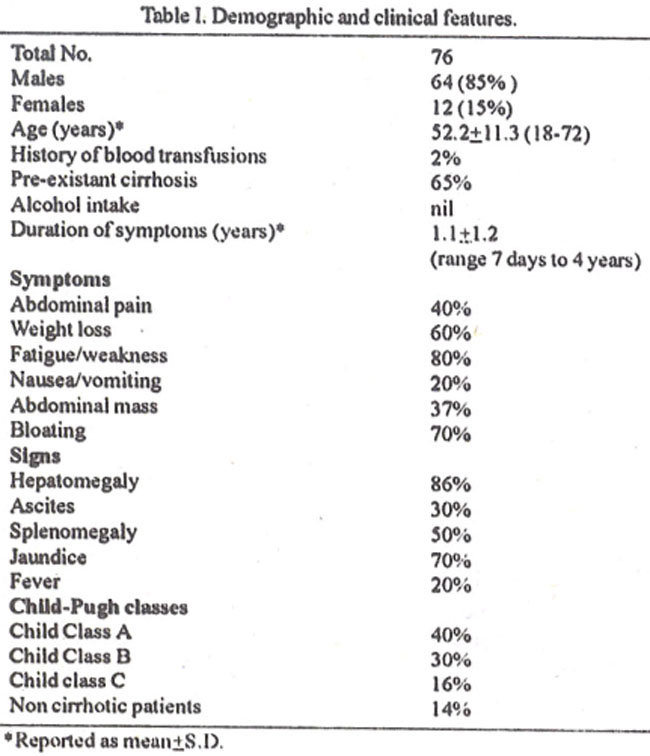
Males outnumbered females by 5.8: 1. Sixty five percent of the patients were aware of pre-existent cirrhosis. In 5 patients (6.5%) HCC was diagnosed incidentally on ultrasound examination of abdomen carried out for unrelated symptoms. lii7 cases (9.2%) ultrasound evaluation of HCC was doubtful. The true nature of altered liver echotexture was established on FNAC as hepatoccilular carcinoma.
Easy fatiguability, postprandial bloating and weight loss were the most common symptoms while jaundice and hepatomegaly were the most common signs.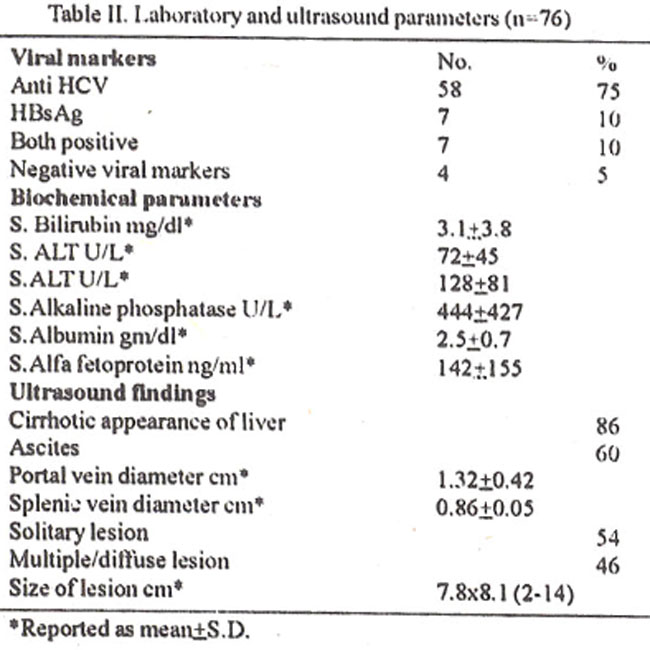
Table II presents details of laboratory parameters including viral serology and ultrasound appearance. Sixty-five percent of anti HCV positive patients had cirrhosis and 10% were non cirrhotics. In 4 patients no viral marker could be demonstrated. Mean values for alkaline phosphatase and serum alfa fetoprotein were significantly higher (p<0.05) in patients with HCC. Alfa fetoprotein levels were not uniformly distributed. 25th and 75th percentile values were 120 ng/ml and 245 ng/ml respectively. No correlation existed between the alfa fetoprotein levels and clinical, biochemical aad ultrasound features of HCC.
Eighty-six percent of patients had cirrhosis determined on clinical examination and ultrasound appearance of liver. Only 14% had normal ultrasound appearance of liver. Fifty-four percent of our patients had a solitary lesion either in the left (16%) or right lobe (38%), 20% had two simultaneous lesions and in the remaining 26% the tumor was multiple (>3 lesions) or diffuse (involving whole of the right or left lobe). In 6% portal vein invasion and thrombosis was found on ultrasound examination. Mean size of lesion reported on ultrasound examination was 7,8x8. 1 cm. Whereas in non-cirrhotic livers it was larger than 6cm.
Histopathological diagnosis of HCC was established in 60 patients. In 4 cases a repeat FNAC was required. Sixteen patients (3%) died after FNAC due to uncontrollable bleeding evidenced by rapidly increasing hemorrhagic ascites and irreversible shock. One patient became hypotensive after FNAC but responded to intravenous volume expansion with plasma and infusion of 3.5% colloidal solution of poly geline.
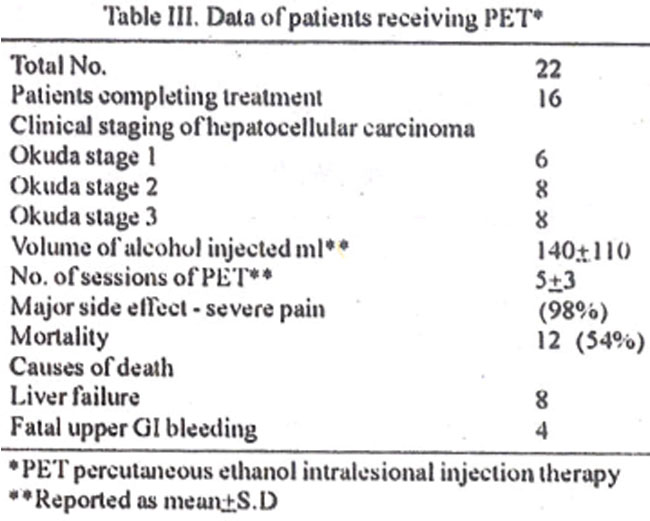
Table III presents details of 22 patients who received ETP as palliative therapy. Mqjor side effect limiting the volume alcohol injected at each session of PET to only 5-10cc was severe pain. However, after addition of 2% xylocaine the total volume per session increased to 40 cc. Mean (±S.D) number of sessions required for completing treatment were 5±3. Six patients did not complete the treatment, 3 of these refused additional injections and the remaining 3 died before treatment could be completed. During a mean follow up of 1 year (range 5 months to 1.5 years), 12(54%) patients died. The major cause of death was liver failure. One patient developed encephalopathy within 48 hours of alcohol injection and died in hepatic coma. Another developed a liver abscess that was drained successfully under ultrasound guidance. Logistic regression analysis identified tumor size greater than 8 cm, advanced liver disease with liver failure and 01 bleeding as predictors of poor response to intralesional alcohol therapy.
Discussion
Hepatocellular carcinoma is one of the most common visceral malignancies worldwide with variable incidence in different countries’. An estimated one million people die of this disease each year16. Strong epidemiologic evidence links chronic injection with hepatitis B (HBV) and C (HCV) viruses on a background of cirrhosis as major risk factors. Earlier diagnosis by estimation of serum alfa fetoprotein levels and ultrasound screening failed to prolong survival17,18 and has not altered the dismal prognosis of this dreaded disease. However. experience from Far East is at variance with that from the West20. Surgery, which is the only curative treatment, is amenable in a small number of cases due to extent of tumor and associated cirrhosis10. Amongst the alternative treatment options available, percutaneous ethanol therapy (PET) offers palliative results comparable to surgical resection in HCCs smaller than 4 cm15,19,20-23.
The present study indicates that HCC was more commonly associated with anti HCV infection than HbsAg associated liver disease; 75% of patients were anti HCV positive compared to 10% positivity rate for HbSAg. A higher prevalence of HCV associated HCC has also been reported from Shaukat Khanum Memorial Cancer Research Institute24,25.
Lahore and from Japan . Most of the HCC cases in South Africa5, Italy26, Southern Punjab27 and in one study from Northern Punjab28 were HbsAg positive. These discrepancies in the prevalence of H BV and HCV in the etiology ofcirrhosis and HCC need to be explored further.
Meanage forHCC inourseries was 52.2±11.3 vearsand was similar to data reported by Maliket al28 and Tasceret al7. Most common symptoms were easy fatigueability followed by postprandial bloating and weight loss while clinically detectable jaundice and a palpable liver were the most common signs. The presence of these clinical features in patiems w liii cirrhosis warrant thorough evaluation for possible development of HCC.
Fine needle aspiration cytology (FNAC) was carried out under ultrasound guidance in 60 patients. In 16 cases FNAC could not be done due to impaired clotting. Two patients (3%) died after FNAC due to uncontrollable bleeding although their clotting profile determined before FNAC was normal. The mortality rate in our series is thus considerably higher than the 0.1% rate reported elsewher12,13 This may be attributed to inclusion of all stages of livcrcirrhosis i.e.. Child class C in our series.
Logistic regression analysis revealed that in patients subjected to therapy cumulative size of lesions greater than 8 cm, Child- Pugh class C. liver failure and upper GI bleeding developing after initiation of PET were predictors of poor response to ethanol therapy. Of 7 patients, who completed treatment protocol, ultrasound examination follow—up was carried out every 3 months to evaluate the size of lesions and recurrence of tumor. During this period recurrence was noted in 1 patient after 9 months. lie received additional PET. However, due to large size of lesion and progressive decline of liver function, lull calculated volume could not be given. He is alive albeit, with evidence of liver failure. Three patients did not show complete resolution of lesions on ultrasound examination. Repeat FNAC revealed dysplastic cells but no malignant cv tology was reported. The remaining 3 patients are free of tumor recurrence at 5 months of follow-up.
One year survival of 45% in this series is considerably lower than reported series.15,19-23 One reason could be the size of lesions injected. All studies reported to date have evaluated response to PET with HCCs less than 5 cm in size. Perhaps selection of patients with Lumorsize less than 5cm would have improved the overall prognosis.
Hepatocellular carcinoma had a higher prevalence in middle aged males and a strong association with hepatitis C positive cirrhosis. liflralcsional ethanol therapy as a palliative procedure was associated with poor outcome in those patients with a cumulative tumor size greater than cm. Child-Pugh class C. liver failure and upper GI bleeding.
References
1. Rustgi AK Epidemioloy of hepatocellular carcinoma Gastroenterol Clin North Am., 1987;16:454-51.
2. Zaidi SHM Primary liver cancer in Pakistan J Pak Med Assoc, 1979;29:99-102.
3 Tariq NA A review of 50 cases of heoatocellular carcinoma Pak J Med Res., 1990;29:97-99.
4. Tsukuma H, Hiyama T, Tanaka S, et al Risk factors for hepatocellular carcinoma among patients with chronic liver disease N Engl J Med., 1993;328:1797-1801.
5. Kew MC, Yu MC, Kedda MA et al. The relavtive roles of hepatitis B and C viruses in the etioligy of hepatocellular carcinoma in Southern Affican blacks Gastroenterology. 1997;112;184-187.
6. Malik IA, Tariq WUZ. Viral hepatitis in Pakistan Pak J Pathol., 1993;4:1-5.
7. Malik IA, Ahmed N, Luqman M, et al Hepatitis C as a cause of chronic liver disease in Northern Pakistan J Pak Med Assoc., 1992;42:67-68.
8. Tariq WUZ and Malik IA Hepatitis C virus in Pakistan perspective. In proceeding." 10th Biennial Scientific Meeting of Asian Pacific Association for the study of liver and 12th. Congtess of Pakistan Society of Gastroenterology and GI Endoscopy". Rawalpindi, January 12-15, 1996,pp 243-58.
9. Zuberi SJ, Lodhi TZ and Samad F Prevalence of hepatitis B surface antigen and antibody in healthy subjects with liver disease. J Pak Med Assoc., 1978;28:2-3.
10. Venook AP Treatment of hepatocellular careinoma. Too many options? J Clin Oncol., 1994;12:1323-1334.
11. Cao G, Kuriyama S, Du P, et al. Complete regression of established murine hepatocellular carcinoma by in vivo tumor necrosis factor alpna gene transfer Gastroenterology, 1997;112:501-510.
12. Buscanni L, Fomari F, Bolondi L, et al. Ultrasound-guided fine-needle biopsy of focal liver lesions. Techniques, diagnostic accuracy and complications. A retrospective study on 2091 biopsies J.Hepatol., 1990;11:344-348.
13. Fornari F, Civardi G, Cavanna L, et al. Ultrasonically guidid fine needle aspiratiob biopsy. A highly diagnistic procedure for hepatic tumors Am J Gastroenterol., 1990;85:1009-1013.
14. Harbin WP. Robert NJ,. Ferrucer JF. Dragnosis of cirrhosis based on regional changes in hepatic morphology. A radiology and pathological analysis Radiology, 1980;135:273-283.
15. Shiina S, Tagawa K. Niwa Y. et al. Percutaneous ethanol injection therapy for hepatocellular cercinoma Results in 146 patients. Am J Radiol.,1993;160:1023-1028.
16. Wanebo HJ, Falkon G, Order SE. Cancer of the hepatobiliary system. In De-Vita V, Hellman S and Rosenberg SA. eds cancer Principles and practice of Oncology 3rd ed. Philadelphia. PA, Lippincott. 1989,pp 836-874.
17. Colombo M, De-Franchis R. Del N, et al. Hepatocellular carcinoma in Italin patients with cirrhosis N. Engl. J, Med., 1991;325:675-680.
18. Cottone M. Rurri M, Caltagirone M, et al. Early detection of hepatocellular carcinoma associated with cirrhosis by ultrasound and alfa fetoprotein. A prospective study. Hepatogastroentrology, 1988;35:101-103.
19. Livraghi T, Bolondi L, Lazzaront S, et al Percutancous ethanol injection in the treatment of hepatocellular carcinoma in cirrhosis. A study in 207 patients Cancer, 1992;69:925-929.
20. Ebara M, Ohto M, Sugiura N, et al. Percutaneous ethanol injection for the treatment of small hepatocellular carcinoma Study of 95 patients J. Gastroenterol Hepatol., 1990;5:616-626.
21. Franco D, Capussotti L., Smadja C, et al. Resection of hepatocellular carcinoma Results in 72. European patients with cirrhosis. Gastroenterology 1990;98:733-738.
22. Kotoh K, Sakai H, Sakamoto S. et al The effect of percutaneous ethanol injection therapy on small solitary hepatocellular carcinoma is comparable to that of hepatectomy. Am. J. Gastroenterol, 1994;89:194-198.
23. Bruix J, Cirera I, Calvet X, at al. Surgical resection and survival in Western patients with hepatocellular carcinoma, J Hepatol., 1992;15:350-355.
24. Yousaf MA, Aftab LK, Saced K, et al. Hepatocellular carcinoma in Pakistan. in proceedings’ 32nd Annual Meeting of the European Association for the study of the liver’ 9-12 April, London, 1997, (Supplement No’)), p. 290.
25. Hamasaki K, Nakata K, Tsutsumi T, et at Changes in the prevalence of hepatitis B and C infection in patients with hepatocellular carcinoma in the Nagasaki Prefecture, Japan, 3 Med. Virol., 1993;40:146-149
26. Colombo M, Kuo G,Choo QL, etal. Prevalence of antibodies to hepatitis Cvirus in italian patients with hepatocellular carcinoma. Lancet, 1 989;ii~(8670) 1006- 1008.
27. Taseer Ill, Malik IH, Mustafa 0, et al. Primary hepatocellular carcinoma with high prevalence of hepatitis B virus infection in Southern Punjab. Pakistan. JCPSP, 1996,6293-295.
28. Malik IA, Ahmad N, Butt SA et al. The role of hepatitis B and C viruses in the aetiology of hepatocellular carcinoma in Northern Pakistan, is preliminary report JCPSP, 1995;526-28.
29. Livraghi T, Salmi A, Bolondi L et at. Small hepatocellular carcinoma Percutaneous alcohol injection. Results in 23 patients Radiology, 1988,168:313-317.
30. Castells A, Bruix J, Fester J, et at Treatment of small hepatocellular carcinoma in cirrhotic patients: A cohort study comparing surgical resection and percutaneous ethanol injection Hepatology, 1993;18:1121-6.
31. isobe H, Sakat H, Imari V. et al Intratumour ethanol injection ther apy for solitary minute hepatocellular carcinoma. A study of 37 patients J Clin Gastroenterol. 1994;18:122-632. Castellano L, calandra M, Blanco CDV et at. Pdredictive factors of survival and intrahepatic recurrence of hepatocellular carcinoma in cirrhosis after percutaneous ethanol injection Analysis of 71 patients J Hepatol 1997,27:862-870.
32. Castellano L, calandra M, Blanco CDV et at. Pdredictive factors of survival and intrahepatic recurrence of hepatocellular carcinoma in cirrhosis after percutaneous ethanol injection Analysis of 71 patients J Hepatol 1997,27:862-870.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: