
Farzana Shafqat ( Department of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Anwaar A. Khan ( Department of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Altaf Alam ( Department of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
K. Butt ( Department of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Arshad ( Department of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
S. Waqar H. Shah ( Department of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
Altaf Baqir Naqvi ( Department of Gastroenterology, Shaikh Zayed Postgraduate Medical Institute, Lahore. )
July 1998, Volume 48, Issue 7
Original Article
Band Ligation Vs Endoscopic Scierotherapy in Esophageal Varices: A Prospective Randomized Comparison
Abstract
Objective: A prospective randomized trial was conducted to compare efficacy, safety and complications of band ligation (BL) with sclerotherapy (Sel).
Methods: Patients with esophageal variceal bleeding were randomized into two study groups. BL (group A) was done in 28 patients whereas 30 pateints (group B) had Scl. After initial treatment, follow-up sessions were repeated by the same method every two weeks till obliteration or reduction to grade 1. Subsequent sessions of endoscopy were done every three months, same procedure was repeated for recurrence of varices and for any episode of rebleeding.
Results: Initial control of bleeding by Scl was achieved in 22 of 28 patients (78%) and in 23 of 24 patients (96%) with BL. Eradication of varices was significantly better achieved in BL group, with less treatment sessions required in Group A as compared with group B 2±1.2 vs 5+2.5, P<0.001). Major complications (3% vs 16%, P < 0.05) as well as mortality (11% vs 21%, P>0.05) was higher in group B.
Conclusion: Band ligation was more effective mode of treatment and was associated with lesser early mortality and complications as compared with sclerotherapy (JPMA 48:192,1998).
Introduction
Variceal bleeding is a life threatening complication of portal hypertension, cirrhosis being the most important cause in Pakistan1. About 30% patients with liver cirrhosis get variceal bleeding with a 40% mortality following the first episode. Seventy percent of survivors get second episode of bleeding within one year2. Therapeutic endoscopy is effective in the management of upper GI bleeding3, whose primaiy goal is to control active bleeding and prevent recurrent bleeding thus reducing the morbidity and mortality. Scierothempy, over the last five decades, has been found effective in controlling active bleeding and reducing recurrent bleeding4-6. It, however, requires multiple sessions to achieve eradication with frequent selerotherapy failures and several local and systemic complications7-9. Some fatal complications, i.e., esophageal perforation and mediastinitis have been reported10,11. During sclerotherapy, the scierosant injected into the vat-ices is responsible for most of the major systemic complications.
Band ligation, a new modality of treatment was devised to reduce the possibility of these complications12. In band ligation, the obliteration of varices is due to mechanical strangulation ofvarices. As no chemical is introduced into the circulation, therefore, it is considered to be superior in efficacy and associated with fewer complications13. We conducted a prospective randomized trial to compare band ligation with scierotherapy regarding their efficacy, safety and complications.
Patients and Methods
Patients with esophageal variceal bleeding were included consecutively in this prospective, randomized study.
Inclusion criteria were: patients more than 18 years of age, with endoscopic evidence of variceal bleeding. Patients with liver cirrhosis and non-cirrhotic portal hypertension were included in the study. It also included those who had received octreotide (sandostatin), balloon tamponade therapy and beta blockers. Beta- blockers were however, not continued during the study. Exclusion criteria were: patients unfit for endoscopy, esophageal stricture, associated disease with death expected within six months, previous history ofendoscopic or surgical treatment of varices. Informed consent was obtained from all patients or their guardians. Randomization was done by sealed envelopes into Group A (BL) and group B (Sc!).
Actively bleeding patients were admitted and those with history of recent bleeding were treated as outpatients. Initial management was carried out within twelve hours of onset of bleeding alter resuscitation or apparent stoppage of bleeding. Treatment sessions were repeated every 2 weeks till the eradication of varices. Subsequent follow-up endoscopy was done every 3 months or for any episode of rebleeding. Recurrent varices or bleeding was treated with originally assigned form of endoscopic therapy. Patients were also randomized further in each group to either receive sucralfate or orneprazole. In case of treatment failure alternative procedure was done, oilier life saving measures, e.g., sengstaken blakemore tube (SB tube) placement, use of ocireotide, or shunt surgery was considered in case the bleeding was not control led.
Grading of the varices was done from 1-4 as described earlier14. In scierotherapy group, 75% alcohol was, injected either paravariccal ly or nt ravariceally. Injections were started at or near gastroesophageal (GE) junction and confined to distal 8 cm of the esophagus and proximal 1-2 cm of stomach. Aliquot of 2 ml of sclerosant was injected at each site but not more than 20ml during each session. Injection sclcrotherapy was rendered at a site distal to actively bleeding varix initially prior to finishing the session.
Band ligation was performed with an cudoscopic ligation device and overiube (Bard International Products Tewsbury, Mass.) as previously described15. Individual varices were ligated at least once per treatment, whereas, larger varices twice at separate sites, but no more than 10 ligations were performed during one session. In patients with active bleeding. ligation was performed at or around the site of bleeding to control haemorrhage, followed by ligation of rest of the varices.
Severity of cirrhosis was assessed according to Child Pugh’s classification16. Other variables noted were, stay in the hospital (in days), number of blood transfusions, use of SB. tube, use of sandostatin and of other medications, i.e., sucralfate or omeprazole. Outcome evaluation included initial control of bleedi ng, rebleeding, variceal eradication, number of sessions required for obliteration of varices, recurrence of varices, complications and mortality. Instructions were given to report immediately to the accident emergency or G.l. department, in case of bleeding or occurrence of other complications. i.e; dyspnoea. chest pain, high grade fever and drowsiness.
Statistical Analysis
Student’s t-Lest was used to compare the means of continuous variables. Nominal values were compared with comparison of proportion. e.g., hemostasis. recurrence of varices, recurrent bleeding, obliteration of varices. complications and mortality.Kaplan—Mcier analysis was used to examine the time to death and the log rank test was used to compare difference between groups.
Results
Seventy patients were enrolled in the study from January, 1996 to February, 1997, 12 were excluded. Seven of these had hepatocellular carcinoma and 5 were lost to follow up. Fifty- eight patients completed the study, 28 in group A and 30 in group B. Baseline clinical amid endoscopic characteristics were similar (Table I).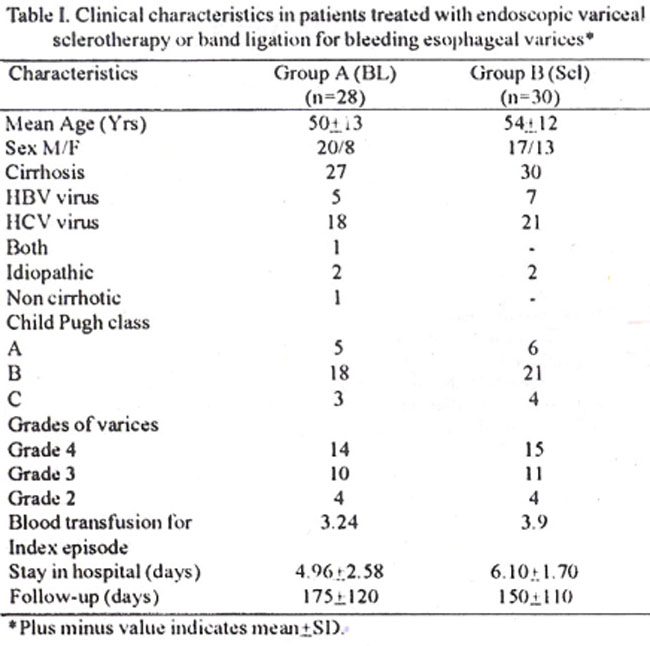
All patients were ci rrhotic except one in group A. Hepatitis C virus in 39(67%), hepatitis B in 12 (20%) and both B and C in one (2%), was associated with cirrhosis. Majority of patients in both groups belonged to child-pugh class B , (65%A, vs 70%2) and had high grade (grade 3 and 4) varices (86%A vs 87%15) Results were comparable regarding requirement of blood transfusion and hospitalization: mean duration of follow-up was 175±1 20 days in group A and 150±110 days in group B (Table I). Filleen patients of group A and 7 of group B had history of previous bleeding, whereas 24 (86%) of group A and 28(93%) of group B (Scl) were actively bleeding at presentation. Two patients had spurting varix which when ligated, immediately stopped bleeding. Hemostasis in acute bleeding, although better achieved in group A, did riot reach statistical significance (96% vs 78%. P >0.05) (Table Il).
Recurrent bleeding was seen in similar percentage of patients (29% vs 28%. P >0.05) in both groups. Esophageal varices and treatment induced ulcers were the source of rebleeding in both groups (Table II).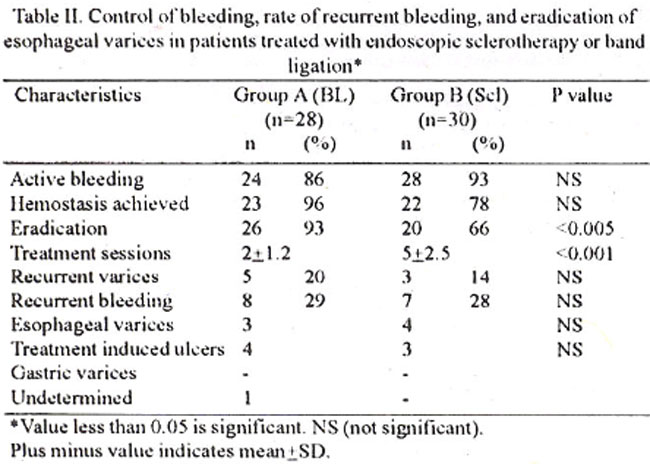
There was no definite correlation between the incidence of recurrence of bleeding and the severity of liver disease. Eradication of varices was achieved in greater number of patients belonging to group A (93% vs 67%, P<0.005) and mean treatment sessions required for obliteration of varices were less in group A as comapred with group B (2±1.2 vs 5±2.5, P<0.001) Table II).
Mirror complications of chest pain, fever and transient dysphagia were seen in both groups, chest pain and fever was significantly more in Group B. Transient odynophagia was experienced in 50% of group A and noire in group 13 patients. Sixteen patients in group A and 19 in group B had esophageal ulcers that were the cause of rebleeding in 3 patients in group A and 4 patients in group B (Table III).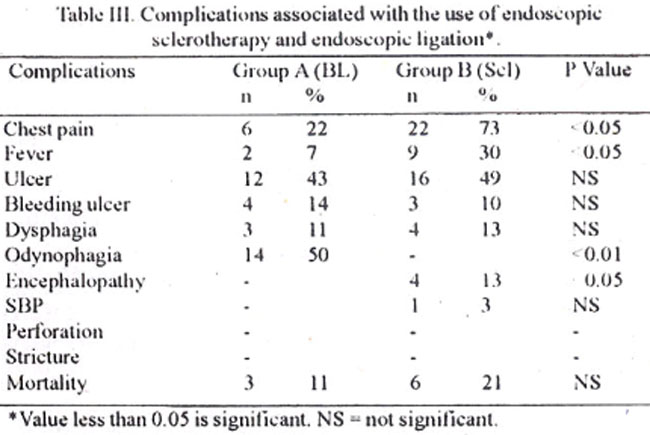
In group A major complications were, aspiralion pneumonia in 1 (3%), whereas in group B encephalopathy in 4 (13%) and bacterial peritonitis in 1 (3%) case was seen. Stricture, esophageal perforation or pleural effusion was not seen in either group (Table IV).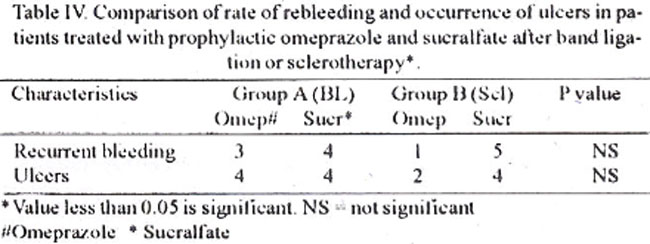
Three (1 1%) of group A and 6(21%) of group B patients died during follow-up. All patients in group A died of uncontrolled bleeding within 30 days of treatment and belonged to Child Pugh class C, 2 had bleeding ulcers and in 1 cause of bleeding could not be determined. Of six patients who died in group B. 4 belonged to Child Pugh class C and the rest to child Pugh class B. Causes of death were hepatic encephalopathy in 2, SBP in 1 and uncontrolled bleeding in 3 patients.
Discussion
Variccal band ligation has been compared with scierotherapy in large randorniLed trials17,18. Post necrotic cirrhosis due to chronic viral hepatitis was the commonest cause of variceal b1eeding inourpatieiits as had been shown by studies from China19,20 whereas commonest cause was alcoholic cirrhosis in the USA and the Europe17,18. Control of active bleeding was effectively achieved in both groups, the results were comparable to other studies15,21,22
Recurrent bleeding rate was comparable in both groups; esophageal varices and bleeding ulcers were responsible in equal proportions. Rebleeding rate in group A (BL)as seen in our study was similar to that reported by others15,18,20 but higher rebleeding rates were seen with sclerotherapy15,18,19. Jensen et al, reported rebleeding rates of 30% Vs 35% in their patients receiving band ligation and sclerotherapy respectively, these results are similar to our study21.
Rapid obliteration of varices with lesser number of sessions seen in band ligation in our study corroborates well with previous reports1,20, Recurrence of varices in band ligation and scierothempy did not have statistical difference, although increased recurrence in band ligation was seen by Hou et al20. Others have reported a variable recurrence rate of 20% - 68% after initial eradication with sclerotherapy23-25. Stiegmann et al, over a follow-up of 10 months, reported recurrence rate of 50% in Scl group and 33% in BL group15.
Frequency of treatment induced complications in band ligation were significantly lower as compared with scierotherapy, mild chest pain and transient fcver were significantly more in sclerotheray. These findings were similar as previously reported26-27. . An equal percentage of patients developed ulcers in both groups of our study. Others have found higher incidence when endoscopy was repeated earlier, e.g., 70% at 1 week and 30% at two week intervals9. Type of ulcers was different in two groups, superficial, shallow ulcers in band ligation whereas deep linear ulcers in scierotherapy group, others have reported similar findings30. Results of prophylactic use of medications, omeprazole and sucralfate, were similar regarding occurrence of ulcers and rebleeding (Table IV). Major complications were seen mostly with scierotherapy, i.e., encephalopathy, bacterial peritonitis, as compared to aspiration pneumonia in band ligation. Similar results were reported previously by other workers16,17. No patient had stricture or perforation in either group. Similar observations was made by Gimson et al, who attributed it to regular use of prophylactic sucralfate. We found no statistical difference in prophylactic use of sucralfate or omeprazole in our study. Sucralfate31 and ranitidine32 have been found to decrease the incidence of bleeding ulcers and stricture formation.
Survival, although not statistically significant, was better in band ligation (Figure).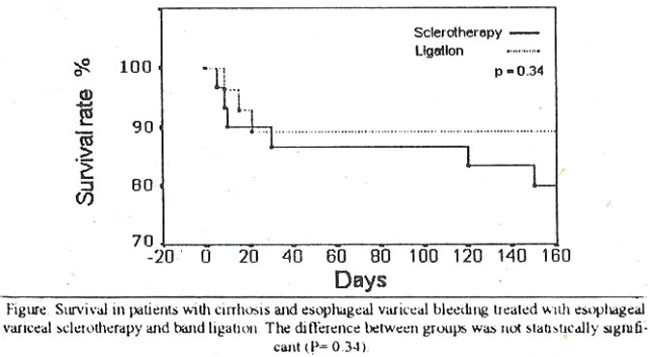
All deaths in this group occurred in child C patients due to uncontrolled bleeding and these were within 1 month of initiating treatment. None died due to procedure related compi ications, although this has been reported in some studies16,17.
This study showed that band ligation was significantly superior to sclerotherapy in esophageal variceal bleeding in terms of lower number of sessions required for obliteration and lesser complications induced by it. These observations in this short term study arc indicative of a definitive promising role of band ligation in the armamentarium for treatment of esophageal variceal bleeding.
Acknowledgments
We thank Dr. Abdul Harneed and Dr. Ashraf Chaudhary for statistical assistance and Mr. Rashid for typing the manuscript.
References
1. Hameed K, Khan I. Nazir SM, et al Injection sclerotherapy using absolute alcohol in bleeding esophageal varices JCPSP. 1996;61:296.298.
2. Graham DY. Smith JI. The course of patients alter variceal hemorrhage Gastroenterology. 1981:80;800-809.
3. Steigmann GV Endoscopic management of esophageal varices Adv Surg. 1994,27:209.31.
3. Hashizume M, Kitano S. Koyanagi N, et al Endoscopic Injection selerotherapy for 1.000 patients with esophageal varices A nine- yew prospective study Hepatology, 1992;15:69-75.
5. K itano S. Iso Y, Hashizume M, et al Selerotherapy Vs esophageal transection vs distal splenorenal shunt for the clinical management of esophageal varices in patients with child class A and B liver function, A prospective randomized trial Hepatology, 1992;15:63-68.
6. Kochhar R, Gocrika MK, Mebta SR Esophageal structures following endoscopic variceal scierotherapy Antecedents, clinical profile and management Dug. Dis, Scu, 1992;37:347-52.
7. Baillie j, Yudelman P Complications of endoscopuc selerotherapy of esophageal varices, Endoscopy, 1992;24 284-91.
8. Van.Stiegmann G and Yamamoto M Approaches to the endoscopie treatment of esophageal varices World J Surg., 1992,16.1034-41.
9. Akriviadi SE, Korula A, Gupta S. ci at Frequent endoscopic variceal sclerotherapy increases risk of complications Prospective randomized controlled study of two treatment scheduks. Dig Dus. Scu 1989,34 1068-74.
10. Sarin SR Endoscopic sclerotherapy for esophageal gastric varices A critical reappraisal Aust. N.Z J Med., 1989:19.162-72.
11. Stiegrnann GV. Cambre-Sun JH A new endoscopic elastic band ligating device. Gastrointest Endosc., 1986;32:230-33.
12. Laine L, Cook D. Endoscopic ligation compared with selerotherapy for treatment of esophageal variceal bleeding Ann lnterns. Med, 1995;123:280-87.
13. Khan AA, Nadeemullah A Treatment of esophageal varices by absolute alcohol selerotherapy. Pak.J, Med Res,, 1992;31:36-38.
14. Stiegrnann GV Goff\\\'JS. Michaletz-Onody PA, et al Endoscopic scierotherapy as compared with endoscopre ligation for bleeding esophageal varices N EngI J. Med, 1992;326:1527-52
15. lugh RNH, Murray-Lyon IM, Daw son JL, et al Transection of the esophagus for bleeding esophageal varices. Bri. Surg., 1973,60:646-49.
16. Lame L, El-Newthi HM. Migikovsky 13, et al Endoscopic ligation compared with selerotherapy for the treatment of bleeding esophageal varices Ann Intern lvted, 1993,119-17.
17. Gimson AES, kamage JR. Panos MZ et al. Randomized trial of variceal band ligation versus Injection selerotherapy for bleeding esophageal varices Lancet, 1993;342:391-94.
18. Lo (HI, Lai K, Chang CE et al A prospective, randomized trial of injection sclerotherapy Vs banding ligation in the management of bleeding esophageal varices. Hepatology, 1995;22:466-71.
19. Uou MC, Lin HC, Kuo BIT, et al Comparison of endoscopic variceal injection selerotherapy and ligation for the treatment of esophageal variceal hemorrhage. A prospective randomized trial Hepatology, 1995;21:1517-22.
20. Jensen DM, Koyacs TO, Randall GM, et al Initial results of a randomized study of emergency bleeding Vs sclerotherapy for bleeding gastric or esophageal varices (Abstract) Gastrointest Endose 1993;39 279-280.
21 Munido F, Mitrarn C, Rodriguez G, et al Endoscopic variceal treatment, is hand ligation taking over aclerotherapy? (Abstract) Am. J Gastroentrol. 1993;88. 1493
22. Westaby D, Williams K Follow-up study after sclerotherapy Seand Gastroenterol, 1984;19(Suppl 102) 71-75.
23. Sarin SK, Sachdcv G, Nanda R. Follow-up of patients after varuceal etadication Ann Surg 1986;204:78-82.
24. Takasc Y, Shibuya S, Chikamori F, et al Recurrence factors studied by percutaneous transhepatuc portography before and after endoscopic sclerotherapy for esophageal varices Hepatology, 1990;11:318-52.
25. Terblanche J, Bomman I’C. Kahn D, et at Failure of repeated injection sclerotherapy to improve long term survival after esophageal variceal bleeding A live-year prospective controlled clinical trial Lancei, 1983,ii 328-32.
26. The Copenhagen Esophageal variccs sclerotherapy Project Sclerotherapy after first variceal haemorrhage in cirrhosis. randomized multucentre trial N. EngI. J. Med.. l984;31:1594-1600.
27. Infante.Rivard C. Esnola S and Villeneuve JP Role of endoscopic variceal aclerotherapy in the long-term management of vanceal bleeding A mets-analysis. Gastroenterology, 1989,96:1087-92.
28. Sarin SK, Mishra SP, Sachdev GK, et at Ethanolamine oleate versus absolute alcohol as a variceal scierosant: A prospective, randomized, controlled trial. Am. J. Gastroenterol., 1988,83:526. 30.
29. Young MF, Sanowaki RA and Rascho R. Comparison and characterization of ulcertions induced by endoscopic ligation of esophageal varices versus endoscopic scierotherapy (see comments) Gastrointest Endosc., 1993;39:119-22.
30. Gaudy H, Rosman A and Krossen M. Prevention of stricture formation after endoscopic aclerotherapy of esophageal varices. Gastrointest Endosc., 1989;35:3 77-80.
31. Kumar A, Matha SR. ioshi V. ut al. Ranitidine for the prevention of complications following endoscopic sclerothcrapy for esophageal varices. J. Assoc., Physicians india, 1993;41:584-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: