
K.M.I. Pal ( Department of Surgery, Aga Khan University Hospital, Karachi. )
A. Khan ( Department of Surgery, Aga Khan University Hospital, Karachi. )
July 1998, Volume 48, Issue 7
Original Article
Abstract
Acute appendicitis is a common surgical emergency in urban setting, of a developing country. The computerised hospital patient database at Aga Khan University Hospital, Karachi, was utilised to obtain records of all adults with a histologically proven diagnosis of acute appendicitis. A review of patients treated over a 18 month period was undertaken. One hundred and three append icectomies were performed for acute appendicitis during this period. The diagnosis was clinical in all cases. Investigations like leucocyte count and lower abdominal ultrasound scan were used to improve diagnostic accuracy without a clear advantage. A number of routine investigations like, haemoglobin estimation and urea, creatinine, electrolyte measurements, did not provide additional information. The duration of antibiotic treatment in acute simple appendicitis was empiric and could be reduced to a single preoperative dose. Peritoneal fluid culture studies had a poor yield (26%) and results were not found to effect management in acute simple appendicitis. The routine use of Ampicillin in all cases of bacterial peritonitis needs re-evaluation, as a high incidence (73%) of resistance was seen. Studies to define the role and duration of treatment, with a single antibiotic, in acute simple appendicitis should be undertaken. Acute appendicitis is probably the most frequently considered surgical differential diagnosis at any hospital dealing with acute surgical conditions. The established treatment continues to be surgical removal of the inflamed organ. The diagnosis and decision to operate both are accepted to be based on clinical judgement, though a number of investigative manoeuvres have been described to reduce the negative append icectomy rate1. Other areas of debate are the number and length of antibiotic treatment and use of bacterial culture studies in cases of simple acute appendicitis2,3. To analyse present practice and identify areas for study and change, a retrospective study was undertaken at Aga Khan Unviersity Hospital (AKUH), Karachi (JPMA 48:189, 1998).
Patients and Methods
Records of patients with a final diagnosis of acute appendicitis from 1st July, 1994 to 31st December. 1995 were reviewed. Hospital computerised patient database was queried to extract all adult discharges with a principal (histologically proven) diagnosis of acute appendicitis. Negative appendicectoniics were variables were looked at:
undertaken in emergency thus excluded. The following demographic data, investigations room, length of stay in hospital before operation, operative findings, peritoneal culture results wound management, antibiotic therapy, type and duration, postoperative hospital stay, complications arising during hospital stay and first post operative cli nic visit.
Results
A total of 103 cases with a Final diagnosis of acute appendicitis were treated during the study period. There were 70 (68%) males and 33 (32%) females with a male to female ratio of 2:1. The mean age was 30 years (range 18-70).
Investigations performed as part of the work up of patients are shown in Figure 1.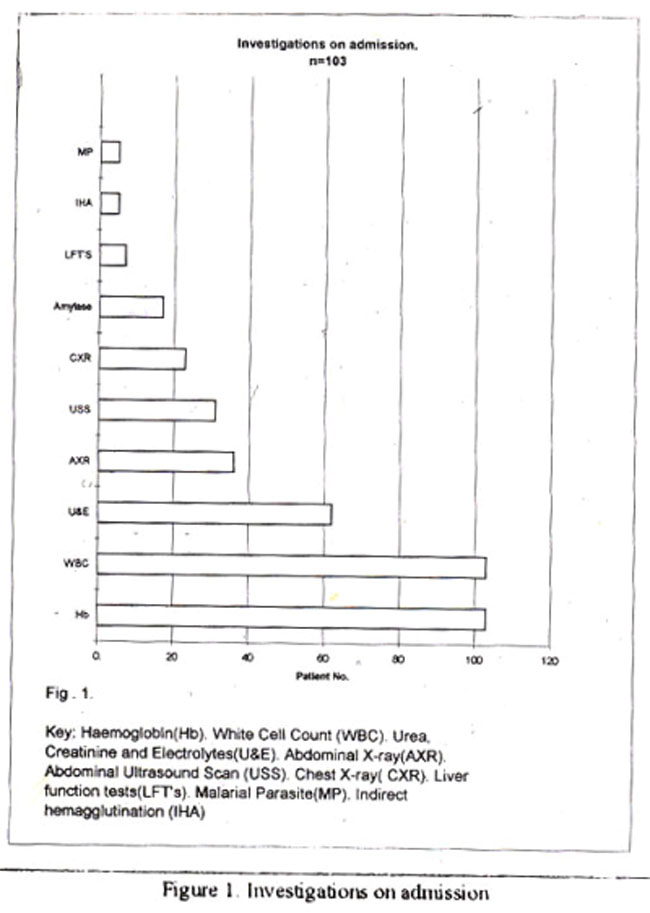
Haemoglobin (Hb) was checked in 101 patients, white cell count (WBC) estimation was done in all patients. Serum creatinine, urea, electrolyies were estimated in 60 patients. Chest x-rays were performed for patients above 50 years. An abdominal ultrasound scan (USS) was undertaken in all female patients to help exclude gyanecologic pelvic pathology.
Two female patients had a Hb below 10 gms/dL, the rest were within normal range. A raised WBC was seen in 70% of patients. Urea, creatinine and electrolyte (U&E) estimations were all within normal range. An abdominal Ultrasound was helpful in arriving at the correct diagnosis by idemifying an enlarged appendix, in three patients. Once a decision for appcndicectomy was made, it was routine to give a combination of Ampicillin, Gentamicin and Metronidazole, intravenously. The subsequent length of antibiotic therapy depended upon the operative findings and was empiric. With no free pus in the peritoneal cavity the treatment was either discontinued or two further doses were given (Figure 2).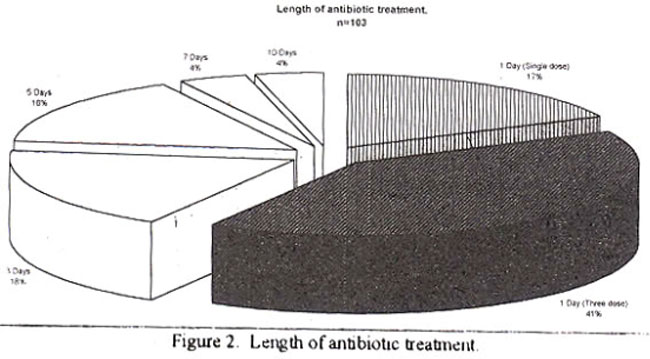
If pus or a gangrenous/perforated appendix was found, treatment was continued for 3 to 5 days, or longer.
The mean duration of hospital stay before surgery was 7 hours (range 2—26). All 103 patients were taken to theatre with a suspected diagnosis of acute appendicitis. The majority were explored through a transverse right iliac fossa incision (Lanz type) ora classic Gridiron incision. Three patients had a formal laparotomy through a midline incision, for generalized peritonitis. Seventy-three (7 1%) were found to have simple acute appendicitis with local peritoneal inflammation and no free pus in the peritoneal cavity. Thin) (29%) patients were found to have a gangrenous and/or perforated appendix with free pus. A standard appendicectomy was performed in all cases with burial of stump.
A culture swab was meant to be routinely takefl on opening the peritoneum, in all cases of bacterial peritoneal inflammation. On review, a total of 80 culture swabs could be traced. It could not be ascertained if the missing 23 were not taken or were lost in processing. All the missing swabs were from cases of acute simple appendicitis. On a verbal questionnaire to residents and Chief Residents it was noted that 98% routinely took peritoneal swabs on entering the peritoneal cavity in all cases of acute appendicitis irrespective of presence of fluid or pus. Of the 80 swabs plated. 30 (37.5%) showed pathogen growth. Of these, 17 swabs ere taken from cases with frank pus and a perforated or gangrenous appendix (n=30), while 13 swabs were from patients with simple acute appendicitis (n=50). The spectrum of bacterial growth is shown in Figure 3.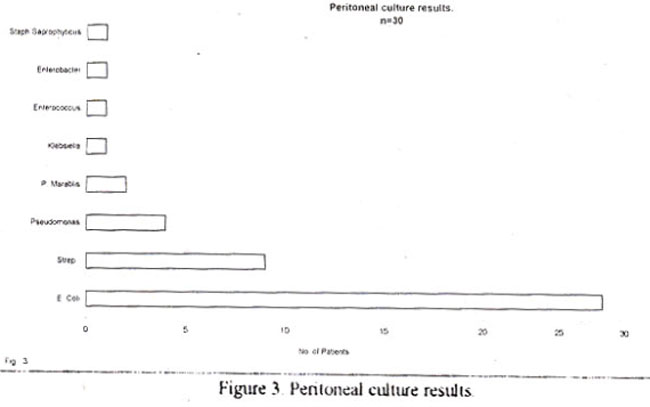
As has been welt reported, E. coli were the most common of the aerobic organisms4. No anaerobic organisms were isolated.
The skin and subcutaneous tissue was left open in 26 (25%) cases with pus in the peritoncum. Of the 77 patients with closure of skin. 3 developed a wound infection, giving a wound infection rate of 3.9%. There were no other complications noted in this subgmup. The patients with intraperitoneal pus had the skin and subcutnaeous tissues left open postoperatively and were allowed to heal by seconthuy intention or delayed primazy suture. In this group there were no complications, which required further intervention or change in therapy. No patient required a change in antibiotics during course of treatment.
The mean hospital stay was 3 days (range 2-14). All patients were seen in the post operative clinic atleast once before final discharge.
Discussion
Appendicectomy continues to be the emergency counterpart of inguinal hemia repair, for surgeons in training. Careful review of practice is continuously needed to avoid complacency and deteriorating patient care.
The wide and easy availability of multiple investigations has led to a tendency to ask for multiple tests, sometimes without a clear indication. In elective surgical settings it has been shown repeatedly that routine laboratory testing as a screening procedure, is non-rewarding and uneconomical5-9. This could be extended to certain acute clinical illnesses of short duration, in otherwise healthy and asymptomatic individuals. The routine testing of Hb and U&E’s in otherwise healthy individuals does not contribute to clinical management.
The diagnosis of acute appendicitis continues to be a clinical decision. A ziumber of investigations have been studied to enhance the diagnostic accuracy. A raised WBC is a sensitive indicatorbut lacks specificity1. Real time Ultrasound examination in expert hands has been reported to have a sensitivity in the range of 75-94% and a specificity of 86-100%10,11. The operator dependency of this investigation is a limiting factor. In our case, most of the US examinations were performed out of working hours, usually by radiology residents. The procedure was useful in excluding gynaecological causes of right lower quadrant pain, rather than making a firm diagnosis of acute appendicitis.
Use of antibiotics has reduced the postoperative infectious complications, like intraperitoneal abscesses and wound infection, in acute appendicitis12. During the period of study, 61(60%) patients were given treatment which could be classified as prophy lactic i.e., 1 to 3 doses. All these patients had their wound primarily closed. A wound infection incidence of 3.9% was noted in this group, but there were no intra-abdoniinal complications. Prophylactic use of antibiotics has been extensively studied and at present there is no evidence to suggest that three doses perioperatively are superior to a single dose preoperatively.
A number of studies has shown that for simple acute appendicitis. use of a single antibiotic gives equivalent results to triple therapy with Ampicillin, Gentamicin and
Metronidazole2,13-15. An important factor with the use of single antibiotic therapy is the saving in physician, nursing and pharmacy time as well as manpower resources. Both the above mentioned factors could be combined to reduce the cost of treatment, while maintaining the quality of care.
A look at the bacterial spectrum in the current series (Figure 3), shows that E. coli arc the dominant species, followed by Streptococcus and Pseudomonas. Antibiotic sensitivity testing revealed that about 73% of E. coil were resistant to Ampicillin. Considering these to be otherwise healthy adults, with pathogens derived from their own gut organisms, this is a worrying indicator. This also raises the question about continuing the use of Ampicillin as a component of blind triple therapy for bacterial peritonitis developing in the comniunity setting.
A further question raised is the usefulness of routine peritoneal culture swabs in all cases of acute appendicitis irrespective of the presence of pus. There was a poor yield from culture swabs taken in the absence of gross peritoneal contamination. In cases of simple acute appendicitis with positive peritoneal cultures, management was not influenced by culture results. It seems that dispensing with the use of culture swabs in simple acute appendicitis would not adversely affect patient outcome. On the other hand it would reduce the cost of treatment.
Another area of concern is the total absence of anaerobic growth in peritoneal cultures during the study period. A number of factors have been identified as contributory. Firstly, anaerobes because of their sensitivity to Oxygen require special precautions in sample collection. The swabs (Transwab; Medical Wire and Equipment Co. Ltd., Corsham. Wilts, England) used are appmved for anaerobic culture growth, but their yield has been poor for this variety of organisms. Any delays in transportation and plating have a negative effect on the yield. The use of preoperative antibiotics is also thought to contribute to poor culture results.
In conclusion, complete patient record keeping and computerisation of data is essential if rapid and effective reviews of practice are to be undertaken. This can be achieved in a developing country set-up, as is shown by this study. The decision to operate in acute appendicitis is usually made on history and physical examination. Other investigations have a supporting role in difficult cases. A variety of “routine” investigations do not provide any added useful information. The continuing use of Ampicillin as a component of triple therapy for bacterial peritonitis needs re-evaluation. The length of antibiotic treatment in cases of acute appendicitis without gross peritoneal contamination is variable and seems to be empiric. There is evidence to suggest that shortening the duration to single dose, will not adversely affect outcome in this subgroup of patients. The routine use of peritoneal swabs for culture and sensitivity in cases without frank pus at operation is of questionable value1. A further area of study could be the definition of local resistance patterns to a single antibiotic for use in acute simple appendicitis. A suitable combi nation would be amoxycil Iine and clavulanic acid (Augmentin). If peritoneal cultures show a high level of sensitivity to this antibiotic, a controlled study could be undertaken to establish its place. Steps have been taken to impmve the anaerobe yield by provision of special anaerobic culture medium in theatres. The process of specimen delivery is being streamlined to reduce delays before final inoculation.
References
1.Hoffmann J, Rasmussen 0. Aids in the diagnosis of acute appendicitis. Br. J. Surg., 1989;76:774.779.
2.DiPiro JT, Cue JT. Single.agent versus combination antibiotic therapy in the management of intraabdominal infections. Pharmacotherapy, 1994.14:266-72.
3. McNarnara MJ, Pasquale MD, Evans SR. Acute appendicitis and the use of intraperitoneal cultures. Surg Gynecol. Obstet., 1993;177:393-7.
4. Gorbach SL. Antimicrobial prophylaxis for appendectomy and colorectal surgery. Rev, infect. Dis., 1991; 13 (Suppl 10):S8 15- S820.
5. Macpherson DS. Preoperative laboratory testing: Should any tests be ‘routine’ before surgery? Med. Clin. North Am., 1993;77:289.307.
6. Nary BJ, Hansen TR. Warner MA. Preoperative labratory screening in healthy Mayo patients Cost-effective elimination of tests and unchanged outcomes. MayoCtin. Proc., 1991;66:155-159.
7. Turnbull, J, Buck, C. The value of preoperative screening investigations in otherwise healthy individuals: Arch. Intern. Med., 1987,147:1101-1105.
8. Musket AD, McGreevy JM. Rational preoperative evaluation. Postgrad. Med. J., 1986;62:925-928.
9. Kaplan EB, Sheiner LB, Boeckmann Al et at. The usefulnesa of preoperative laboratory screening. JAMA, 1985;253 :3576-3581.
10. Wade DS, Morrow SE, Balsara ZN et al. Accuracy of ultrasound in the diagnosis of acute appendicitis compared with the surgeons clinical impression, Arch Surg, 1993,128:1039-44 Discussion 1044-6.
11. Baithazar, EL Birnbaum BA Yee J et al. Acute appendicitis. CT and US correlation in 100 patients. Radiology, 1994,190:31-35
12. Bohnen JMA. Solomkin iS, Dellinger EP et at. Guidelines for clinical care: Anti-infective agents for intra-abdominal infections Arch Surg., 1992; 127:83-89.
13. Salam IM, Abu-Galala KI, el-Ashaal Yl. A randomized prospective study of cefbxitin versus piperacillin in appendicectomy J. Hosp. Infect., 1994;26 133-136.
14. A1-Dhohayan A, al-Sebayl NI, Shibl A et at. Comparative study of augmentin versus metronidazole/gentamicin in the prevention of infections after appendicectomy. Eur. Surg. Res., 1993;25.60-64.
15. Bennion RS. Thompson lB. Baron El et al Gangrenous and perforated appendicins with pertonitis Treatment and bacteriology (‘tin. Ther., 1990;12(Suppl C): 31-44.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: