
Shahid Ahmed ( Department of Endocrinology, Combined Military Hospital, Lahore Pakistan. )
Zahir Shah ( Department of Radiology, Combined Military Hospital, Malir, Pakistan. )
August 2010, Volume 60, Issue 8
Case Reports
Abstract
A 38 years old man presented with 2 years history of low backache and progressively increasing stiffness of the spine. Movements were restricted at lumbar spine due to stiffness especially forward flexion was markedly reduced. He was suspected to be suffering from ankylosing spondylitis. There was no tenderness over sacroiliac joints or lumbar spine. Yellowish green Ochronotic pigmentation of cartilage of ears was noted. Radiographs of lumbar and thoracic spine revealed narrowing of inter-vertebral spaces with calcification of intervertebral discs. Homogentisic acid was present in the patient\'s urine sample, suggesting him to be suffering from Alkaptonuria. Patient is being managed with non steroidal anti-inflammatory drugs and vitamin C, 1g daily.
Introduction
Alkaptonuria is one of the disorders originally defined as an inborn error of metabolism by Archibald Garrod in his Croonian Lectures of 1902.1 Alkaptonuria is an autosomal recessive disorder. It results from a deficiency of an enzyme homogentisate 1,2-dioxygenase (HGD) activity in the liver2 that normally splits the aromatic ring of homogentisic acid, a tyrosine-degradation product. This leads to accumulation of large quantities of homogentisic acid in the body. Deposition of homogentisic acid and its metabolites in tissues causes ochronosis, with darkening of cartilaginous tissues and bone, arthritis and joint destruction, and deterioration of cardiac valves.3-5 In urine, large quantities of homogentisic acid are excreted which oxidize to benzoquinones, and form melanin-like polymers, resulting in dark discoloration of urine on standing.2 Vitamin C, up to 1 g/d, is recommended for older children and adults. The mild antioxidant nature of ascorbic acid helps to retard the process of conversion of homogentisate to the polymeric material that is deposited in cartilaginous tissues. Though treatment with vitamin C to enhance homogentisic acid degradation has not proved helpful in some studies,6 however, 2-(2-nitro-4-trifluoromethylbenzoyl)-1,3- cyclohexanedione (NTBC) or nitisinone (Orfadin), has been proposed as potential therapy because it inhibits the enzyme that assists the conversion of 4-hydroxyphenylpyruvate to homogentisic acid (i.e., 4-hydroxyphenylpyruvate dioxygenase).7
Case Report
A 38 years old man, an office clerk by profession presented with 2 years history of low backache and progressively increasing stiffness in the spine causing restriction of forward and lateral bending. Stiffness was slightly more in the morning but was generally constant all the time. In the previous one year he had also developed pain in knee joints, shoulders and elbows, mild to moderate in severity and associated with mild morning stiffness. There was no history of associated fever, diarrhoeal illness, urinary tract infection or any skin lesions. There was no history of any other significant illness in the past. He was a non smoker and non alcoholic. He was married for 8 years with no children and had 3 sisters, 43, 45 and 47 years and a brother, 40 years of age. None of the siblings was having any symptoms resembling his illness. On examination he was a young man of thin built, with a pulse rate of 70 beats per minute, respiratory rate 16 per minute and 120/70 mm Hg blood pressure. Respiratory system examination revealed markedly reduced chest expansion due to reduced movement of the chest cage. Chest was normal on auscultation. Examination of abdomen and cardiovascular system was also unremarkable. Movements were restricted at lumbar spine due to stiffness especially forward flexion was markedly reduced. Schober's test was strongly positive. There was no tenderness over sacroiliac joints or lumbar spine. Movements at cervical spine were also slightly restricted. Yellowish green Ochronotic pigmentation of cartilage of the ears was present (Figure-1).
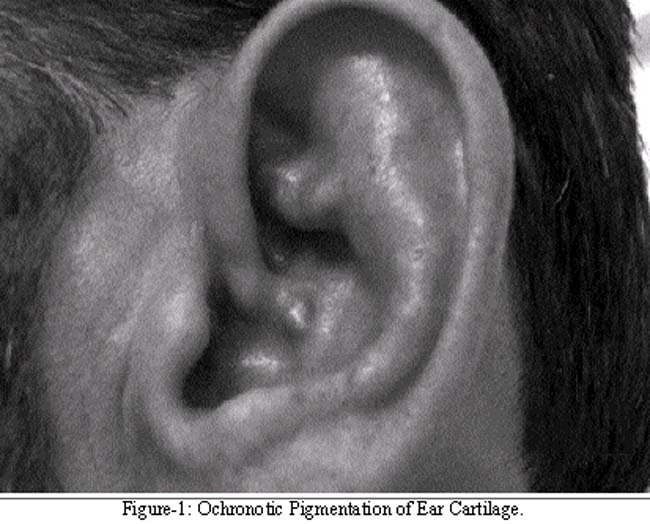
Sclerae were not involved yet. Haemoglobin was 14.2 g/dl and ESR 30 mm fall at the end of first hour. Serum urea, creatinine, sodium, potassium, calcium, phosphate and uric acid were within normal limits. Serum was negative for Rheumatoid factor. Radiographs of lumbar and thoracic spine revealed narrowing of inter-vertebral spaces with calcification of intervertebral discs (Figure-2).

Radiographs of cervical spine and knee joints did not reveal any calcification. Homogentisic acid was present in the patient's urine sample, suggesting Alkaptonuria. There was no history of passing dark urine or staining diapers in childhood, or exposure to any chemical which can cause acquired ochronosis. Echocardiography did not reveal any valvular abnormality. Ultrasonography of kidneys and urinary tract did not suggest nephrolithiasis.
Patient is being managed with non steroidal anti-inflammatory drugs and vitamin C, 1g daily because of a potential role that it might retard the process of conversion of homogentisate to the polymeric material that is deposited in cartilaginous tissues. Nitisinone is not available yet. All his siblings were tested for the presence of homogentisic acid in the urine but none of them showed a positive result.
Discussion
This young patient presented with a history of chronic low backache and gradually increasing stiffness of the lumbar spine. This history, combined with severely restricted forward flexion at lumber spine, raised the suspicion of ankylosing spondylitis. But yellowish green pigmentation of the ear cartilage and calcification of intervertebral discs on plain radiographs of lumbar spine suggested the possibility of alkaptonuria.
It is estimated that the current incidence of alkaptonuria is 1 case in 250,000 to 1 million live births.2 Clinically, alkaptonuria resembles ankylosing spondylitis5,8 in its particular damage to the spine and large joints but differs in sparing the sacroiliac joint. We also started investigating our case initially with a provisional diagnosis of ankylosing spondylitis. The spinal involvement results in kyphosis, height loss, and decreased lumbar flexion, and the joint disease decreases the range of motion and causes effusions. Ochronotic arthritis resembles a crystalline or inflammatory arthritis in its waxing and waning course. Joint symptoms typically begin in the third or fourth decade of life and progress until chronic pain prompts a knee, hip, or shoulder replacement; on average, this occurs at the age of 55 years. Tendon and ligament ruptures occur with minimal provocation, and kidney stones probably form because of the extremely high levels of urinary homogentisic acid excretion.8
Joints and connective tissue involvement like pigmentation of sclera and ear cartilage, tendons and ligaments thickening and tears, joint effusions etc. usually present after 30 years of age. Our patient, 38 years old had Ochronotic pigmentation of ear cartilage only. Nephrolithiasis and mitral and aortic valvular calcification and regurgitation usually present in late middle age.8
Because alkaptonuria is autosomal recessive, a family pedigree, in all likelihood, reveals no other affected individuals. However, because many individuals are asymptomatic, the low frequency of affected family members may be due to a lack of ascertainment.9
References
1.Garrod AE. The incidence of alkaptonuria: a study in chemical individuality. 1902 [classical article]. Yale J Biol Med 2002; 75: 221-31.
2.Watts RW, Watts RA. Alkaptonuria: a 60-yr follow-up. Rheumatology (Oxford) 2007; 46: 358-9.
3.La Du BN. Alkaptonuria. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic & molecular bases of inherited disease. 8th ed. Vol. 2. New York: McGraw-Hill, 2001; pp 2109-23.
4.Ffolkes LV, Brull D, Krywawych S, Hayward M, Hughes SE. Aortic stenosis in cardiovascular ochronosis. J Clin Pathol 2007; 60: 92-3.
5.Perry MB, Suwannarat P, Furst GP, Gahl WA, Gerber LH. Musculoskeletal findings and disability in alkaptonuria. J Rheumatol 2006; 33: 2280-5.
6.Wolff JA, Barshop B, Nyhan WL, Leslie J, Seegmiller JE, Gruber H, et al. Effects of ascorbic acid in alkaptonuria: alterations in benzoquinone acetic acid and an ontogenic effect in infancy. Pediatr Res 1989; 26: 140-4.
7.Anikster Y, Nyhan WL, Gahl WA. NTBC and alkaptonuria. Am J Hum Genet 1998; 5: 201-4.
8.Phornphutkul C, Introne WJ, Perry MB, Bernardini I, Murphey MD, Fitzpatrick DL, et al. Natural history of alkaptonuria. N Engl J Med 2002; 347: 2111-21
9.Keller JM, Macaulay W, Nercessian OA, Jaffe IA. New developments in ochronosis: review of the literature. Rheumatol Int 2005; 25: 81-5.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: