
Shaikh Samiullah ( Department of Medicine Liaquat University of Medical &Health Sciences, Jamshoro, Hyderabad. )
Rahoopoto Qasim ( Department of Medicine Liaquat University of Medical &Health Sciences, Jamshoro, Hyderabad. )
Shaikh Imran ( Department of Medicine Liaquat University of Medical &Health Sciences, Jamshoro, Hyderabad. )
Jaffery Mukhtair ( Department of Medicine Liaquat University of Medical &Health Sciences, Jamshoro, Hyderabad. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objective: To observe the frequency of admission hyperglycaemia and its influence on the outcome of patients with intracerebral haemorrhage.
Methods: This case series study included 450 consecutive patients received in medical wards at Liaquat University Hospital Jamshoro/Hyderabad with a diagnosis of Spontaneous Intracerebral Haemorrhage within 24 hours of their first stroke onset, between September 2006 to December 2008. The patients with haemorrhage secondary to brain tumours, trauma, haemorrhagic transformation of cerebral infarct, with previous history of haemorrhagic stroke, and patients with Glycosylated Haemoglobin greater than 8.5% were excluded from the study. Hyperglycaemia was defined as an admission or in-hospital fasting blood glucose level of 126 mg/dl (7 mmol/liter) or more or a random blood glucose level of 200 mg/dl (11.1 mmol/liter) or more on 2 or more determinations. The patients were divided into 2 broad groups, good outcome groups (i.e. patients who survived), and poor outcome group (patient died).
Categorical variables such as age, sex, volume of haematoma, GCS score, presence of admission hyperglycaemia, Mean arterial pressure (MAP), and site of haematoma were expressed as percentage and frequency. Chi-square test was applied for comparing categorical variables such as hyperglycaemia, GCS score, and age with the outcome of the patients. Multivariate logistical regression analysis was done. A p-value 0.05 was considered as statistically significant. All calculations were done using SPSS version 16 (Chicago, IL, USA).
Results: Of the 450 consecutive patients, 399 fulfilled the inclusion criteria. Males were 261(65.4%) and females 136 (36, 4%).Patients of over 65 years age numbered 222(55.6%) and 177(44.4%) were less than 65 years. Stress hyperglycaemia was present in 109 (27.3%) cases and 290(72.7%) patients were normoglycaemic. Of the 109 patients who died during hospitalization, 59(54.12%) had presented with admission hyperglycaemia (0.001).
Conclusion: Stress hyperglycaemia is a common finding in patients presenting with intracerebral haemorrhage. It is a marker of poor outcomes and higher mortality, more so in patients with no known history of diabetes (JPMA 60:660; 2010).
Introduction
Primary intracerebral haemorrhage (PICH) is defined as bleeding that evolves within the tissue of the brain. Primary non traumatic intracerebral haemorrhage (ICH) comprises 10-15% of all strokes.1
Stress hyperglycaemia which is the presence of hyperglycaemia without preexisting diabetes mellitus, is a common problem in stroke population. It is estimated that 20%-50% of acute stroke patients present with a concurrent diagnosis of hyperglycaemia.2 Furthermore, hyperglycaemia at the time of stroke in patients without a history of diabetes mellitus has been linked to a poor prognosis in populations of patients with cerebral haemorrhagic strokes.3 As in patients with ischaemic strokes acute hyperglycaemia is associated with increased oedema and infarct size and with reduced cerebral blood flow and cerebrovascular reserve,4 it can be postulated that hyperglycaemia can also increase ischaemic brain damage around an ICH and therefore emerge as a clinical predictor of worse prognosis in these patients. The effects of admission hyperglycaemia on the clinical course after intracerebral haemorrhage (ICH) are largely unknown, and the few relevant studies have been limited by small size, no distinction between diabetic and nondiabetic patients, or lack for controls for other important clinical factors.5,6
The aim of this study was to observe the frequency of admission hyperglycaemia and also the influence of hyperglycaemia on the outcome of the patients with intracerebral haemorrhage.
Patients and Methods
This case series study included 450 consecutive patients received in medical wards at Liaquat University Hospital Jamshoro/Hyderabad with a diagnosis of spontaneous intracerebral haemorrhage (SICH) within 24 hours of their first stroke onset, between September 2006 to December 2008. Informed consent was obtained from all patients included or their legal representatives. Patients information regarding biodata, clinical presentation and laboratory workup was documented in a proforma. SICH was defined as a neurological deficit documented by a brain computed tomography (CT) indicating the presence of an ICH in absence of trauma or surgery.7 The patients with haemorrhage secondary to brain tumours, trauma, haemorrhagic transformation of cerebral infarct, with previous history of haemorrhagic stroke, and patients with HBA1C greater than 8.5% were excluded from the study. All patients were screened according to a strict protocol consisting of a complete medical history, a full neurological examination, standardized blood tests, and a CT scan of the brain within 24 hours. The Glasgow Coma Scale (GCS) assessed initial stroke severity, and it was determined after initial evaluation and resuscitation.8 The patients were categorized in to three groups. Group 1had GCS score 3-4, group two with GCS 5-12 and group three with GCS >12. The following data were collected: age, sex, recognized risk factors for SICH (arterial hypertension, alcohol intake, smoking, diabetes mellitus, serum cholesterol levels, antiplatelet treatment), glucose levels at admission and 72 hours after stroke onset, HbA1C,systolic, diastolic, and mean arterial pressure (MAP) = [(2 x diastolic)+systolic] / 3, and CT scan findings. Patients were grouped according to age, with Group one having age < 60 and Group two age > 65 years. On the basis of MAP patients were categorized in to two with group one having MAP < 130mmHG and group two>130mmHG. Hyperglycemia was defined as an admission or in-hospital fasting blood glucose level of 126 mg/dl (7 mmol/liter) or more or a random blood glucose level of 200 mg/dl (11.1 mmol/liter) or more on 2 or more determinations.HBA1C were done in all patients and level above 8.5% were taken as abnormal.9
Neuroradiological findings were determined in the CT scan and classified according to site of SICH (basal ganglia, thalamic, lobar), volume of haematoma (according to ABC/2 method, in which A is the greatest diameter on the largest haemorrhage slice, B is the diameter perpendicular to A, and C is the approximate number of axial slices with haemorrhage multiplied by the slice thickness),10 midline shift (the displacement of the septum pellucidum across midline, using as reference a perpendicular line connecting the anterior and posterior insertions of the cerebral falx at the level of the lateral and third ventricle,11,12 intraventricular extension of haemorrhage (graded according to Graeb\'s scale).12 On the basis of volume of haematoma patients were categorized into three with group one having volume < 30 ml, group two 30-60 ml and group three>60ml. The primary end point of the study was in-hospital mortality. The patients were divided into 2 broad groups, good outcome groups (i.e. patients who survived), and poor outcome group (patient who died). All patients were given appropriate standard therapeutic care and were monitored during the stay in hospital (up to a maximum of 21 days). All standard investigations such as blood sugar, lipid profile, HBA1C were done from research laboratory of Liaquat University Hospital Hyderabad/Jamshoro and CT scan from the radiology department of the same institution.
Categorical variables as age, sex, volume of haematoma, GCS score, hyperglycaemia and site of haematoma were expressed as percentage and frequency. The chi-square test was used for comparing categorical variables such as hyperglycaemia, GCS score, age and volume of haematoma with the outcome of the patients. The multiple regression method was used to adjust the variables. A p-value 0.05 was considered as statistically significant. All calculations were done using SPSS version 16 (Chicago, IL, USA).
Results
Of the 450 consecutive patients 399 fulfilled the inclusion criteria. Males were 261(65.4%) and females 136 (36, 4%).Patients over 65 years age were 222(55.6%) and 177(44.4%) were less than 65 years. Stress hyperglycaemia was present in 109 (27.3%) cases and 290(72.7%) were normoglycaemic. Out of 109 patients, 59(54.12%) died during the follow up period as compared to 63(21.7) of the 290 patients without hyperglycaemia (p=0.001). GCS score at the time of admission was 3-4 in 120(30.1%) 5-12 in 203(50.9%) and 13-15 in 76(19%) patients. Volume of haematoma was < 30 ml in 183 (45.9%), 30-60ml in194 (48.6%) and >60 in 22 (5.5%) patients. GCS score at the time of admission was 3-4 in 120 (30.1%), 5-12 in 203 (50.9%) and 13-15 in 76 (19%) cases. Site of lesion was thalamus in 174(43.6%), putamen in 81(20.3%) and lobar in 144 (36.1%) patients. Intraventricular extension and midline shift was present in 37(9.3%) patients. A total of 122 (9.3%) patients died during hospitalization.
Table-1 shows the comparison of various variables with the outcome of the patients. All the variables studied had a significant influence on the prognosis. In multivariable analysis only hyperglycaemia (0.001) and GCS score (0.002) at the time of admission proved to be important predictors of mortality Table-2.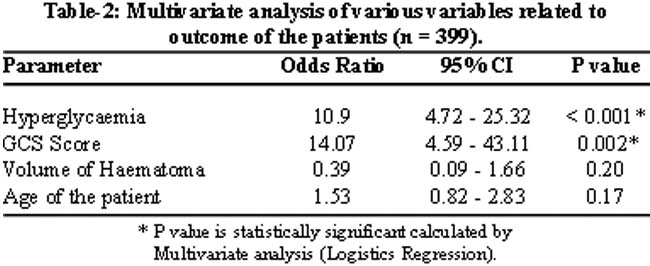
Discussion
This study has shown that hyperglycaemia is an important predictor of outcome of patients with intracerebral haemorrhage. In our study hyperglycaemia was present in 27.3% cases which were higher than 17% reported by Passero S13 who studied 1085 patients with intracerebral haemorrhage.
In our study 54.2% patients died during hospitalization .These figures are close to that observed by Ezzeddine et al14 that admission hyperglycemia is an independent predictor of mortality with 45% mortality as compared to 5% in patients without hyperglycemia and intracerebral haemorrhage. In a study of 181 patients by Odufuye et al, the mortality was 22 times more in patients with intracerebral haemorrhage who had hyperglycaemia at the time of admission without a previous history of diabetes mellitus.15 This statement was further strengthened by Demchuk et al who found hyperglycaemia without diabetes a strong predictor of poor outcome in patients with intracerebral haemorrhage.
In this study in addition to hyperglycaemia the other variables influencing the outcome of patients with intracerebral haemorrhage include haematoma volume, age and level of consciousness at the time of admission.
The GCS score is now a standard neurological assessment tool that is reproducible and reliable.16 It has been associated with ICH outcome in other prediction models.17 Levels between 3-4 correlated with a poor prognosis. Likewise, patients with GCS scores of >13 tend to have a much better outcome. According to Broderick JP, Brott T patients in whom the haematoma volume was 60 cm or greater and the GCS score was 8 or less, the predicted 30- day mortality rate was 91% compared to 19% in those with a volume less than 30 cm3 and the GCS score was 9 or more.18 Size of the haemorrhage has been reported to correlate well with acute ICH mortality.19,20 Our study found a significant correlation between size of the haematoma and ICH mortality in agreement with Drury et al21 and Kanaya et al.22 According to another study, intracerebral haemorrhage volume was consistently associated with the outcome.23 Claude Hemphill contradicts the size of volume as a strong predictor of outcome and stated that other predictors such as low GCS score, advanced age, or IVH influenced outcome to a greater degree.24
In our study more deaths were found in patients over 65 years of age. Some studies have shown age as an independent predictor of ICH whereas others did not find this association.24 The fact that age has been an inconsistent ICH outcome predictor among various models and may have its strongest influence among the group of very elderly patients suggests two possibilities. Either the very elderly sustain worse neurological injury from ICH irrespective of size or location, or overall medical care decisions in elderly patients are less aggressive even if ICH-related neurological injury is not as profound.
In this study on multivariate analysis, hyperglycaemia and GCS score at the time of admission have appeared as significant independent predictors of death. In the study by Passero et al,13 high admission blood glucose was associated with variables signifying the severity of stroke, such as initial MAP,haematoma volume, shift of cerebral midline structures, intraventricular extension, and disturbed consciousness.
Conclusion
Stress hyperglycemia is a common finding and is a marker of poor outcomes and higher mortality in patients with intracerebral haemorrhage. This is more so in patients with no history of diabetes compared to patients with normoglycaemia. Estimation of Blood glucose in patients with stroke is mandatory and if hyperglycaemia is detected, it should be treated aggressively.
Acknowledgement
We are thankful to Dr. Ghulam Hussain, incharge neurology unit for his tremendous support. We are also grateful to Dr. Iftikhar, Dr. Tooba and Dr. Haleema for their help and guidance in writing this article.
References
1.Caplan LR. Intracerebral haemorrhage. Lancet 1992; 339:656-8.
2.Alvarez-Sabín J, Molina CA, Montaner J, Arenillas JF, Huertas R, Ribo M, et al. Effects of admission hyperglycemia on stroke outcome in reperfused tissue plasminogen activator-treated patients. Stroke 2003; 34: 1235-41.
3.Kiers L, Davis SM, Larkins RL, Hopper J, Tress B, Rossiter SC, et al. Stroke topography and outcome in relation to hyperglycemia and diabetes. J Neurol Neurosurg Psychiatry 1992; 55: 263-70.
4.Weir CJ, Murray GD, Dyker AG, Lees KR. Is hyperglycemia an independent predictor of poor outcome after acute stroke? Results of a long term follow up study. BMJ 1997; 314: 1303-6.
5.Woo E, Chan YW, Yu YL, Huang CY. Admission glucose level in relation to mortality and morbidity outcome in 252 stroke patients. Stroke 1988; 19: 185-91.
6.Arboix A, Massons J, Garcia-Eroles L, Oliveres M, Targa C. Diabetes is an independent risk factor for in-hospital mortality from acute spontaneous intracerebral haemorrhage. Diabetes Care 2000; 23: 1527-32.
7.Broderick JP, Adams HP Jr, Barsan W, Feinberg W, Feldmann E, GrottaJ, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1999; 30: 905-15.
8.Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974; 2: 81-4.
9.The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2003; 26(Suppl 1): S5-20.
10.Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 1996; 27: 1304-5.
11.Broderick JP, Brott TG, Duldner JE, Tomsick T, Huster G. Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality. Stroke 1993; 24: 987-93.
12.Graeb DA, Robertson WD, Lapointe JS, Nugent RA, Harrison PB. Computed tomographic diagnosis of intraventricular hemorrhage. Etiology and prognosis. Radiology 1982; 143: 91-6.
13.Passero S, Ciacci G, Ulivelli M. The influence of diabetes and hyperglycemia on clinical course after intracerebral hemorrhage. Neurology 2003; 61: 1351-6.
14.Ezzeddine MA, Tariq N, Vazquez G, et al. Hyperglycemia may be associated with edema progression in acute intracerebral hemorrhage. [P08.141] Poster Session VIII: Stroke: Bench to Bedside, Thursday, April 30, 2009.
15.Odufuye AO, Jain AR, Bellolio FM, et al. Hyperglycemia as a predictor of early mortality in intracerebral hemorrhage. [P02.043] Poster Session II: Prognosis in Intracerebral Haemorrhage, Tuesday, April 28.
16.Juarez VJ, Lyons M. Interrater reliability of the Glasgow Coma Scale.J Neurosci Nurs 1995; 27: 283-6.
17.Lisk DR, Pasteur W, Rhoades H, Putnam RD, Grotta JC. Early presentationof hemispheric intracerebral hemorrhage: prediction of outcome and guidelines for treatment allocation. Neurology 1994; 44: 133-9.
18.Broderick JP, Brott T, Duldnee JE, Temsick T, Huster G. Volume of intracerebral haemorrhage. A paverfus and easy to use predictor of 30-day mortality. Stroke 1993; 24: 987-93.
19.Mase G, Zorzon M, Biasutti E, Tusca G, Vitrani B,Cazzato G. Immediate prognosis of primary intracerebral hemorrhage using an easy model for the prediction of survival. Acta Neurol Scand 1995; 91: 306-9.
20.Portenoy R, Lipton R, Berger A, Lesser M, Lantos G.Intracerebral hemorrhage: a model for the prediction of outcome. J Neurol Neurosurg Psychiatry 1987; 50: 976-9.
21.Drury I, Whisnant JP, Garraway WM. Primary intracerebral haemorrhage: impact of CT on incidence. Neurology 1984; 34: 653-7.
22.Kanaya H, Yukawea H, Itok Z. Grading and indications for treatment in intracerebral hematomas of the basal ganglia (cooperative study in Japan). In: Pia HW, Langmaid C, ZierskiJ (eds): Spontaneous Intracerebral Hematomas. Advances in Diagnosis and Therapy. Berlin: Springer-Verlag, 1980, pp 268-74.
23.Juvela S. Risk factors for impaired outcome after spontaneous intracerebral hemorrhage. Arch Neurol 1995; 52: 1193-200.
24.Hemphill JC 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC, et al. The ICH Score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001; 32: 891-7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: