
Vikram Mehraj ( Department of Pathology & Microbiology, Aga Khan University, Stadium Road. Karachi, Pakistan. )
Mohammad Asim Beg ( Department of Pathology & Microbiology, Aga Khan University, Stadium Road. Karachi, Pakistan. )
Taimur Saleem ( Department of Pathology Medical Students Aga Khan University, Stadium Road. Karachi, Pakistan. )
Saima Lalani ( Department of Pathology Medical Students Aga Khan University, Stadium Road. Karachi, Pakistan. )
Nadia Sani ( Department of Pathology Medical Students Aga Khan University, Stadium Road. Karachi, Pakistan. )
Imran Khan ( Department of Pathology Medical Students Aga Khan University, Stadium Road. Karachi, Pakistan. )
Fatima Afridi ( Department of Pathology & Medical Students, Karachi Medical & Dental College,Aga Khan University, Stadium Road. Karachi, Pakistan. )
Hina Irfan ( Department of Pathology & Medical Students, Karachi Medical & Dental College,Aga Khan University, Stadium Road. Karachi, Pakistan. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objective: Parasitic diseases are a major public health problem in the tropical and sub tropical countries including the subcontinent region. We aimed to assess methods of Parasitology education in medical schools of Karachi Pakistan.
Methods: Ten medical schools in Karachi, Pakistan were sent a structured questionnaire collecting information on different aspects of Parasitology education. The collected data was analyzed using SPSS version 14.0.
Results: The response rate of this study was 90%. Majority of the schools in Karachi, Pakistan (78%) taught Parasitology concurrently with Microbiology, Pathology, Pharmacology and Forensic medicine in third and fourth year of undergraduate training. More than 20 hours were spent on teaching through didactic lectures (56%), interactive lectures (22%), problem based learning (PBL) (22%), clinical cases (11%) and small group discussions (89%). A Clinical Microbiologist or Parasitologist taught Parasitology by using transparencies, handouts and/or computer aids. Variation in education methods existed mainly in the private medical schools.
Conclusion: Medical curricula were meeting the European standards for teaching of Parasitology. However, there is a need for revision and modification in the curricula owing to the high burden of parasitic diseases in the subcontinent region (JPMA 60:613; 2010).
Introduction
Parasitic diseases cause tremendous mortality and morbidity worldwide. Of the 300 million people affected globally, at least 50% are school-age children living in developing countries of the world.1 According to recent WHO estimates, one person in every four harbours parasitic worms.2 The common yet neglected parasitic diseases include Malaria, Schistosomiasis, Hook worm infestation, Leishmaniasis, Giardiasis and Ameobiasis.3 Malaria, the eighth leading contributor to global diseases burden measured in disability adjusted life years (DALYs), poses a risk to 50% of the world\'s population in 107 countries.4,5
Pakistan is an endemic country for parasitic diseases owing to a multitude of factors such as the sub-tropical climate, high level of illiteracy, rapidly mushrooming population, unbridled urbanization, overcrowding, poor hygiene, lack of awareness and lack of access to basic health facilities.6,7 Malaria is a major health problem in Pakistan with an estimated number of annual episodes of about 1.6 million; 33% of these cases are caused by Plasmodium falciparum.8 However, this proportion is now increasing.9 Intestinal parasitic infections are also quite frequent in our population.6 In a study of 350 children aged 1-5 years from an urban slum of Karachi, Pakistan, it was seen that 52.8% of the children had intestinal parasitic infections. More than 40% children had infection with a single parasite while 10% with multiple parasites.10 G. lamblia is an important cause of recurrent abdominal pain in children in Pakistan.11 Similarly, Giardiasis occurs significantly (44%) in young people (mean age 28 ± 17 years) with abdominal pain.12 Cutaneous leishmaniasis affects 1 to 1.5 million people globally; 90% of the disease burden is concentrated in Afghanistan, Pakistan, Syria, Saudi Arabia, Algeria, Iran, Brazil and Peru. After the migration of millions of refugees from the neighbouring country of Afghanistan, the incidence of this disease has increased in Pakistan.13
In view of the magnitude of the problem in the region, it is essential to formulate an indigenous medical curriculum which produces a competent medical graduate who can serve societal needs and is adequately prepared to deal with the common parasitic diseases. Parasitology teaching should be tailored in such a way that factual information is juxtaposed with razor-sharp clinical acumen. It is also important to have an assessment system in place that adequately addresses all subject areas of Parasitology that are globally and locally pertinent. Pakistan Medical and Dental Council (PMDC) develops and revises the curricula of graduate and post-graduate medical education in Pakistan as deemed appropriate. The council also considers the comments and suggestions from senior teachers of medical schools (medical colleges and universities) throughout the country.14 Traditionally, Parasitology has been taught in medical schools as a part of Pathology/Microbiology. This approach of teaching of Parasitology in the wider context of Pathology and Microbiology has its merits and demerits. In the broader picture, teaching Parasitology in parallel with Pathology and Microbiology may help undergraduate medical students\' link different entities together, improving the coherence of the subject matter studied. However, this approach may be detrimental in decreasing its significance in comparison to Virology and Bacteriology. It also reduces the proportion of questions put to the candidates exclusively, from the domain of Parasitology.
A European community education programme "Tempus" made recommendations that basic Parasitology be given at least 20 hours of teaching, be integrated with other medical disciplines to strengthen it and modern teaching/learning methods, such as CD-ROM programs, clinical slides, be incorporated.15
The teaching practices of Parasitology in Pakistan across different medical schools across the country have not been documented. We didn\'t come across any such study in other South Asian countries either. Therefore, the effectiveness of Parasitology teaching in these areas can\'t be gauged. As a first step, we aimed to conduct a study to determine the methods currently used to teach Parasitology in undergraudate medical schools of Pakistan.
Methods
This was a descriptive cross-sectional study. There are 32 medical schools recognized by PMDC in Pakistan14 and currently there are 10 medical schools in the metropolitan city of Karachi. Karachi is the most populated city of Pakistan with an estimated current population of about 16 million. All of these ten medical schools in Karachi were sent a structured questionnaire especially prepared for this purpose. The self administered questionnaires were addressed to the concerned teaching faculty at each of these medical colleges. The questionnaire was formulated on the basis of literature review and extensive discussion with colleagues on the subject. It collected information including methods used to impart Parasitology education, qualification of teaching faculty and methods of student assessment. The study was approved by the Ethics Review Committee (ERC) at The Aga Khan University, Karachi. The information on identification of medical schools was not collected in order to guarantee the confidentiality to the respondents as well as their institutions. The completed questionnaires were coded and the data was entered twice in Epi info version 6.04. It was then transferred to Windows Statistical Package for Social Sciences (SPSS) version 14.0 using DBMS version 2.0 for analysis. The descriptive analysis was conducted reporting proportions of the categorical variables. The data was further analyzed by stratifying on type of medical school into private and government medical schools. Strength of the associations was assessed using Fisher\'s exact test where appropriate. Tables and figures were used for an all-inclusive viewing of the results.
Results
Nine out of ten medical schools participated in this questionnaire based study. The response rate was therefore 90%. Four medical schools (44.4%) belonged to the government sector while the remaining five (55.6%) belonged to the private sector. Formal teaching of parasitology was being undertaken at all the nine medical schools in Karachi, Pakistan.
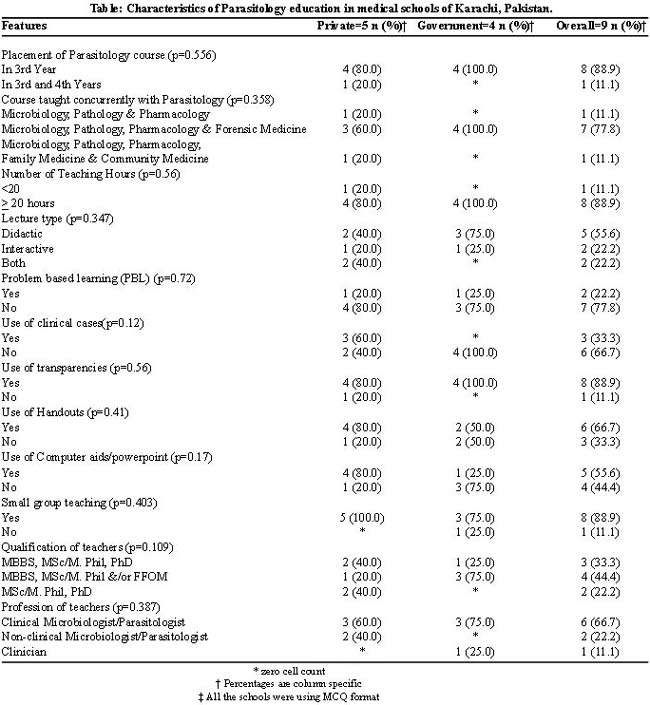
Table describes features of Parasitology teaching in medical schools. In the majority of the medical schools (88.9%), the Department of Pathology was responsible for Parasitology teaching and the discipline was taught in third year of undergraduate medical training. Microbiology, Pathology, Pharmacology and Forensic medicine were the common disciplines being taught concurrently with Parasitology in seven (78.0%) of the medical schools.
Didactic lectures were a common method of teaching (55.6%). Except for three of the medical schools (33.3%), most schools did not use clinical cases. Small group discussion was also popular (88.9%) and problem based learning (PBL) was used by only two schools (22.2%).
In five (55.6%) of the medical schools, the teaching faculty was qualified up to PhD level and most (66.7%) were clinical microbiologists spending more than three hours on teaching Parasitology. The teaching aids used included transparencies (88.9%), handouts (66.7%) and computer aids/Microsoft PowerPoint presentations (55.6%) (Table).
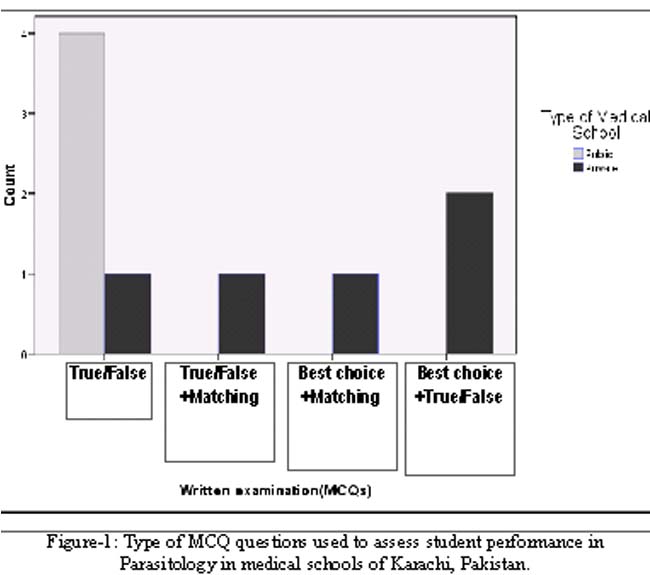
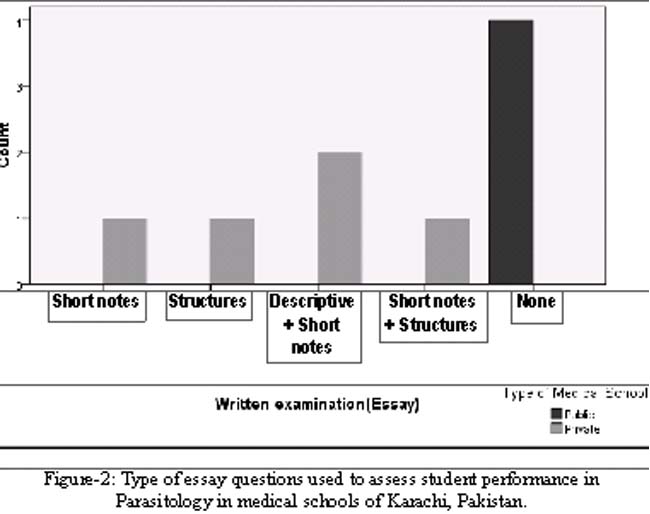
In examinations, essay questions were used by five (55.6%) of the medical schools. Multiple choice questions (MCQs) were being used by all schools with True/False type being most common (55.6%) as far as the details of the assessment were concerned (Figures 1 and 2).
Comparison of Government and private medical schools:
The discipline was taught in third year with only one private school (11.1%) extending the teaching to fourth year. Except for one private school (11.1%), more than 20 hours were spent for teaching Parasitology. Didactic lectures were common (55.6%) with two schools (one private and one government) using interactive lectures and two private schools using both types of lectures. Problem based learning (PBL) teaching method was used by one private and one government medical school. None of the government schools utilized clinical cases for teaching as compared to three private schools. Except for one government school all reported use of small group discussions for teaching. Teaching aids such as transparencies, handouts and computer aids were utilized by all except one private school. Whereas in government schools the use of transparencies, handouts and teaching aids was reported in the order of decreasing frequency as 100%, 50% and 25% respectively. All of private schools reported essay type examination for the student assessment as compared to none of the government schools. Variety of multiple choice questions (MCQ) were used in private schools as compared to only True/False in government schools (Table).
Discussion
Parasitic diseases have been a neglected area of medicine in developing countries. Lack of funding for research, shortage of trained personnel and virtual non-existence of these entities in the developed world in comparison to the developing countries are the reasons for neglect. The knowledge of common parasitic infections is essential for doctors in a country like Pakistan with a high burden of both parasitic infections and factors which lead to their increased prevalence.
Our study reveals that the curricula for undergraduate Parasitology education in most medical schools in Karachi, Pakistan are meeting the Tempus recommendations.16 However, since these recommendations focused on European medical faculties and the parasitic diseases are almost absent from the developed world; there is a need for revision of the curricula and the way it is taught in developing countries such as Pakistan. Our burden of disease is different from the region where these recommendations were formulated; therefore they should be followed with caution.
As seen in our study, the teaching methods are not uniform across the board and there is more diversity in private medical schools in comparison to government medical schools. This certainly will have a variable impact on the knowledge and training of the medical students graduating from these institutions. This also shows that the government medical schools follow more or less the same pattern as compared to the private medical schools. The use of novel modern methods like PBL needs to be considered universally after its evaluation and proven success. Small group learning has also been generally favourably perceived by students in literature17 and this method is being popularly employed at most of the institutions surveyed in our study.
Though only two schools are using PBL system to deliver their curriculum, other medical schools are also exploring this option. It has been shown that in PBL system, the facilitator\'s expertise, responsible for a particular group, does not influence the students\' knowledge in that discipline.18 Therefore, the new system may still be able to meet the requirements of students without finding experts in Parasitology. This becomes an extremely important consideration for developing countries where appropriately trained and qualified clinical faculty may be difficult to find for some clinical disciplines such as Parasitology. Inception of PBL would therefore maximize and capitalize on available resources in the developing countries for Parasitology teaching.
Parasitology education needs to be accorded more attention in a disease endemic country like Pakistan where parasitic diseases are rampant. The medical curricula may not afford adequate clinical exposure to medical students such that they are able to diagnose and treat parasitic diseases competently in a high disease burden area as Pakistan. Indigenous recommendations should be formulated. Future research should focus on prospective assessment of medical graduates\' knowledge on the discipline after application of innovative interventions which will enable to find out the specific target areas requiring improvement. We recommend that the curriculum planners keep the burden of parasitic infections in mind when planning medical curricula and provide adequate representation to this neglected discipline. With the advent of HIV and the subsequent increase in the number of HIV infected cases in this region19,20 opportunistic parasitic diseases will increase and pose an additional burden on the already limited health resources.
Conclusion
This study showed that medical curricula were meeting the European standards for teaching of Parasitology. More variation in education methods exists in the private medical schools of the country.
References
1.WHO. The world health report 1999: Making a difference. Geneva: World Health Organization.
2.WHO. Parasitic Diseases. Initiative for Vaccine Research. (Online) 2007 (Cited 2009, May 27); Available from URL: http://www.who.int/vaccine_research/diseases/soa_parasitic/en/index.html.
3.Renslo AR, McKerrow JH. Drug discovery and development for neglected parasitic diseases. Nat Chem Biol 2006; 2: 701-10.
4.Guinovart C, Navia MM, Tanner M, Alonso PL. Malaria: burden of disease. Curr Mol Med 2006; 6: 137-40.
5.WHO. World Malaria Report 2005. Geneva: WHO and UNICEF, 2005.
6.Siddiqui MI, Bilqees FM, Iliyas M, Perveen S. Prevalence of parasitic infections in a rural area of Karachi, Pakistan. J Pak Med Assoc 2002; 52: 315-20.
7.Bhutta ZA, Gupta I, de\'Silva H, Manandhar D, Awasthi S, Hossain SM. Maternal and child health: is South Asia ready for change? BMJ 2004; 328: 816-9.
8.WHO-EMRO. Epidemiological situation. (Online) 2005. (Cited 2008 Sep 1). Available from URL: http://www.emro.who.int/rbm/countryprofiles-pak.htm.
9.Yasinzai MI, Kakarsulemankhel JK. Prevalence of human malaria infection in bordering areas of East Balochistan, adjoining with Punjab: Loralai and Musakhel. J Pak Med Assoc 2009; 59: 132-5.
10.Mehraj V, Hatcher J, Akhtar S, Rafique G, Beg MA. Prevalence and factors associated with intestinal parasitic infection among children in an urban slum of Karachi. PLoS One 2008; 3: e3680.
11.Younas M, Shah S, Talaat A. Frequency of Giardia lamblia infection in children with recurrent abdominal pain. J Pak Med Assoc 2008; 58: 171-4.
12.Yakoob J, Jafri W, Abid S, Jafri N, Hamid S, Shah HA, et al. Giardiasis in patients with dyspeptic symptoms. World J Gastroenterol 2005; 11: 6667-70.
13.Kassi M, Kassi M, Afghan AK, Rehman R, Kasi PM. Marring leishmaniasis: the stigmatization and the impact of cutaneous leishmaniasis in Pakistan and Afghanistan. PLoS Negl Trop Dis 2008; 2: e259.
14.Pakistan Medical Dental Council: The Statutory Regulatory & Registeration Authority for Medical & Dental Eduation and Practitioners for Pakistan. (Online) 2001. (Cited 2009, May 12). Available from URL: http://www.pmdc.org.pk/about_us.htm.
15.Pawlowski ZS, Goullier-Fleuret A, Bruschi F. Undergraduate teaching of medical parasitology. Parasitol Today 1998; 14: 127-8.
16.Khan AJ. Scope of medical colleges in private sector. J Ayub Med Coll Abbottabad 2004; 16: 1-3.
17.Singaram VS, Dolmans DH, Lachman N, van der Vleuten CP. Perceptions of problem-based learning (PBL) group effectiveness in a socially-culturally diverse medical student population. Educ Health 2008; 21: 116.
18.Kwizera EN, Dambisya YM, Aguirre JH. Does tutor subject-matter expertise influence student achievement in the problem-based learning curriculum at UNITRA Medical School? S Afr Med J 2001; 91: 514-6.
19.Rai MA, Warraich HJ, Ali SH, Nerurkar VR. HIV/AIDS in Pakistan: the battle begins. Retrovirology 2007; 4: 22.
20.Altaf A, Saleem N, Abbas S, Muzaffar R. High prevalence of HIV infection among injection drug users (IDUs) in Hyderabad and Sukkur, Pakistan. J Pak Med Assoc 2009; 59: 136-40.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: