
Sajida Qureshi ( Department of Surgery, Dow University of Health Sciences (DUHS), Civil Hospital Karachi. )
Shahriyar Ghazanfar ( Department of Surgery, Dow University of Health Sciences (DUHS), Civil Hospital Karachi. )
Aftab Leghari ( Department of Surgery, Dow University of Health Sciences (DUHS), Civil Hospital Karachi. )
Fahad Tariq ( Department of Surgery, Dow University of Health Sciences (DUHS), Civil Hospital Karachi. )
Saad Khalid Niaz ( Department of Gastroenterology, Dow University of Health Sciences (DUHS), Civil Hospital Karachi. )
Mohammad Saeed Quraishy ( Department of Surgery, Dow University of Health Sciences (DUHS), Civil Hospital Karachi. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objective: To evaluate the endoscopic dilatation of benign esophageal strictures and its outcome.
Methods: A prospective descriptive study was conducted at Surgical Unit 4 of Civil Hospital Karachi, over a period of 24 months, from August 2006 to July 2008. Twenty seven patients with benign esophageal strictures underwent esophageal dilatation under fluoroscopic guidance using Savary Gilliard Dilators and guide wire. Follow up was done weekly for 2 weeks and monthly for a minimum of 6 months. Treatment success was gauged according to improvement of dysphagia.
Results: A total of 27 patients were included in the study. There were 16 (59.3%) corrosive strictures, 10 (37%) were peptic strictures and one (3.7%) was due to extrinsic compression. Majority of the corrosive strictures, 11 (68.75%) were suicidal in intent p<0.001. Mean dilatation frequency for strictures longer than 5cms was 7.10±5.322 vs. 3.47±3.281 for strictures <6cms (p<0.037). Corrosive strictures were seen more commonly in the upper esophagus as compared to peptic (Mean 22.44 ± 5.240 cm vs. 30.20 ± 4.780 cm), p<0.001. Only 81.4% corrosive stricture could be adequately dilated at initial dilatation as compared to 100% in peptic strictures. Mean symptomatic recurrences per month were 0.6919 ± 0.300 in corrosives and 0.365 ± 0.293 in peptic strictures (p<0.003). There were 4 procedure related perforations, all in patients with corrosive strictures. Overall mortality was 7.4%.
Conclusion: Endoscopic dilatation is safe and effective in treating benign and corrosive esophageal strictures, which have a higher complication rate. Mean recurrence rate decreased over a period of time in both peptic and corrosive strictures (JPMA 60:656; 2010).
Introduction
Many diseases can cause esophageal stricture formation. These include acid peptic, autoimmune, infectious, caustic, congenital, iatrogenic, medication-induced, radiation-induced, malignant, and idiopathic disease processes. Gastroesophageal reflux disease accounts for approximately 70-80% of all cases of esophageal stricture.1-3 Postoperative strictures account for about 10%, and corrosive strictures account for less than 5% in western population. Ingestion of corrosives is a common cause of benign strictures in this part of world.4-6 The injuries are frequently more serious because they are usually intentional, with large volumes of ingestion. This can result in lifelong debilitating conditions and later development of esophageal cancer. Mortality rate after caustic ingestion are reported to be as high as 20%.4
The etiology of esophageal stricture can usually be identified using radiologic and endoscopic modalities and can be confirmed by endoscopic visualization and tissue biopsy.
Progressive dysphagia for solids is the most common presenting symptom. This may progress to include liquids. Atypical presentations include chronic cough and asthma secondary to aspiration of food or acid.
Conservative management of strictures is considered to be a safe and effective method for both short term and long term relief of dysphagia.2,7 The current treatment modality of choice in benign esophageal strictures is endoscopic dilatation,8 although the best technique for dilatation and type of stricture amenable to treatment is controversial. Esophageal dilatation has been used since Middle Ages when bougies made of natural materials were used to push impacted boluses in the stomach. Current dilators are the modification or evolution of these naturally made bougies. Relatively low morbidity and mortality is associated with esophageal dilatation as compared to surgery and this has encouraged its wide spread use.9
The reported experience is mostly in patients with peptic stricture and the data supporting its efficacy and safety in corrosive strictures dilatation is still scarce. We aim to describe our experience of dilatation of peptic and caustic strictures and its outcome.
Patients and Methods
A prospective descriptive study was conducted at Surgical Unit 4 of Civil Hospital Karachi from August 2006 to July 2008 (24 months). The permission for the study was taken from the hospital ethical committee. Twenty seven patients having radiological and endoscopic diagnosis of benign esophageal strictures were included in the study. The data collected was entered into specially made endoscopy database. The site and length of stricture were assessed by radiological and endoscopic examination. Patients having achalasia, post operative strictures and malignant strictures were excluded from the study. Patients who were lost to follow up were also excluded from the study. Generally lost to followup cases are regarded as being unwell and counted as morbid or dead unless proven otherwise.
Informed and written consent was taken from all the patients. Esophageal dilatation was performed as an ambulatory procedure using conscious sedation and topical pharyngeal anaesthesia. Patients were kept nil per OS six hours prior to the procedure to ensure clear view as well as to avoid aspiration. Dilatation was done under fluoroscopic guidance using Savary Gilliard Dilators over the guide wire. A standard guide wire was positioned with the help of endoscope and fluoroscopy up to the antrum. After the guide wire was positioned the scope was withdrawn and dilatation was performed using Savary Gilliard dilators of increasing size. Usually one to three increasing size were used at one session depending on the tightness of stricture and patient\'s tolerance. Post procedure endoscopy was done in all patients to reconfirm the site, length of stricture, adequacy of dilatation, assess stomach and duodenum and to look for any perforation. Patients were advised to take liquids 2 hours post procedure.
Any subsequent dilatations depended on the recurrence of dysphagia, in which case the strictures were dilated to more than 12.8mm or three sizes greater than the initial diameter. Follow up was done weekly for 2 weeks and monthly for a minimum period of 6 months and maximum of 30 months. Treatment success was gauged according to the improvement of dysphagia using dysphagia score.
Adequate initial dilatation was considered when the lumen was dilated upto 12.8mm or the patient having significant improvement in dysphagia. Patients having peptic strictures were kept on PPIs post dilatation. When complication like perforation was suspected, immediate X-ray chest and gastrograffin swallow was done. Patients were kept nil per OS and started on intravenous antibiotics and enteral/parenteral nutrition. Further management was decided according to the progress and response of the patients to conservative treatment.
The collected data was analyzed and results formulated using Statistical Programme of Social Sciences (SPSS) version 11. P value < 0.05 was considered statistically significant. T-test was used for quantitative data and Chi-square for qualitative data.
Results
A total of 27 patients were included in the study. There were 8 males (29.6%) and 19 (70.4%) females. Ages of the patients ranged from 15 to 70 years with a mean age of 33.41 ± 18.213 years. Corrosive strictures were seen in 16 (59.3%) and peptic strictures in 10 (37%) patients. Mean age of patients with peptic strictures was 42.80±19.159 years as compared to 25.88±13.720 years for corrosive strictures (p<0.015). In corrosive strictures the M: F ratio was 1:2.2 as compared to peptic strictures where the ratio was 1:2.3. The length of the stricture ranged from 2-22cms. Mean length of the corrosive strictures was 8.88±5.999cm whereas in peptic strictures it was 3.90±1.729cm (p<0.006). Patients with corrosive strictures for suicidal intent were 11/16 (68.75%) p<0.001. Length of stricture correlation with number of times dilated revealed that for strictures less than 6cms long, mean number of dilatations was 3.47±3.281, whereas for strictures longer than or equal to 6cms it was 7.10±SD 5.322 (p < 0.037). Upper esophagus was involved in 15/27 (55.55%) and lower esophagus in 12/27 (44.44%). Corrosive strictures were seen more common in the upper esophagus (Mean 22.44±5.240cm) as compared to peptic (Mean 30.20±4.780cm) p< 0.001 (Table-1).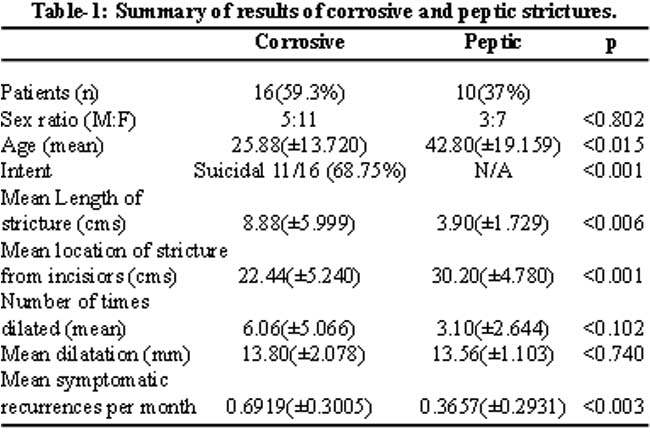
Initial adequate dilatation was done in 81.4% corrosive strictures and 100% of peptic strictures. These were the patients who had >12.8mm dilatation while 11.1% were dilated initially up to 11mm and 7.4% up to 9mm. Mean symptomatic recurrences per month in peptic strictures was 0.365±0.29 where as in corrosive stricture it was 0.691±0.30, p<0.003 (Figure). There were 4 procedure related perforations in patients with corrosive strictures (Table-2).
Overall mortality was 7.4%.
Discussion
Endoscopic dilatation is a safe and effective mode of treatment of benign esophageal strictures. It is increasingly being used as a primary treatment in place of surgery, which is associated with increased morbidity and mortality. Peptic strictures are found commonly as a result of prolonged gastro esophageal reflux disease,10,11 the resultant scarring from reflux esophagitis presenting as a stricture. It is the most common cause of stricture in the lower esophagus. Most of the published literature is on the experience of dilatation in peptic strictures as this constitutes the majority of esophageal strictures. A local study of 369 patients had 63.7% peptic strictures and 1.6% corrosive strictures.1 In the present study 59.3% were corrosive strictures and 37% peptic strictures.
Corrosive injury to the esophagus may be caused by ingestion of strong acids (hydrochloric acid) or a strong base (lye) either with suicidal intent or accidental ingestion. Resultant marked caustic oesophagitis leads to stricture formation within 1 to 2 months after the initial injury. Depending upon the degree of injury and scar formation, affected patients may develop one or more segmental strictures that have unpredictable location or diffuse esophageal stricture that reduces the entire esophagus to filliform strictures. Caustic injury is therefore associated with more extensive stricture formation. This type of esophageal injury is seen most commonly in our part of the world.4,5 Corrosive strictures were seen in 59.3% cases as compared to 37% peptic strictures, showing corrosives as the commonest etiology of strictures in India and Pakistan.5,12 The figures cited in the western literature for corrosive strictures in contrast are 1-4%.
Intent behind 68.75% strictures was suicidal whereas the rest gave a history of accidental ingestion leading to strictures. Suicidal intent strictures were seen more in females (7/11).
Broor SL5 reported a mean age of 25.5 years in a study of 47 patients with corrosive oesophageal strictures. In the present study mean age of patients with corrosives was 25.88 years as compared to 42.8 years in peptic strictures group showing significant association with age (p<0.015). This could be related to immaturity and emotional instability seen in younger age.
Most commonly upper and mid esophagus are involved in caustic ingestion depending on the amount and the substance ingested. In the present study caustic strictures were seen at a mean distance of 22.44 cms. Peptic strictures in contrast were at a mean distance of 30.2 cms, (p <0.001) which is in line with the published literature, confirming that corrosive intake causes more extensive damage starting in esophagus. A study of 58 patients from Turkey13 revealed that the most frequent location of the caustic injury was upper esophagus (36.4%).
The mean length of caustic strictures in the present study was 8.8 cms as compared to 3.9 cms in peptic induced strictures (p < 0.006).
Initial adequate dilatation was accomplished in 81.4% corrosive and 100% peptic induced dilatation, a figure although not statistically significant but indicating that corrosive induced strictures were difficult to dilate. The adequate dilation figures reported in different national and international studies are 94%.1,14 An eight years experience of endoscopic dilatation of corrosive esophageal strictures by Singhal S15 showed successful dilatation in 75.67% cases. Adequacy of dilatation or its success was gauged in terms of major improvement or relief of dysphagia. Satisfactory swallowing in the present study was achieved with dilatation upto 12.8mm.
Longer caustic strictures require more dilatations as compared to peptic strictures (6.06 v/s 3.10. p < 0.102). It was seen that the number of dilatations required for both peptic and corrosive strictures decreased significantly over the period of time (Figure-1).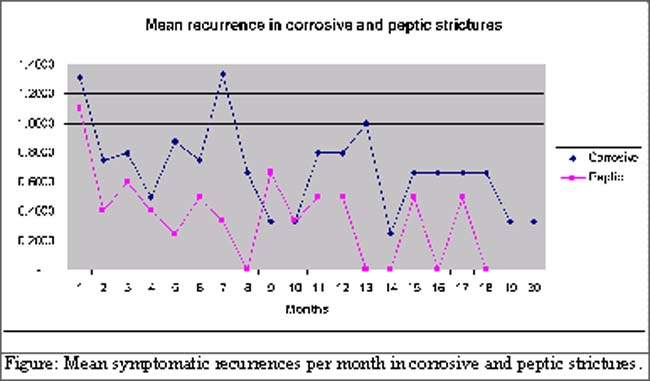
This is similar to a study from India14 which showed that number of dilatations was significantly more in corrosive than peptic induced strictures.
Despite advances in endoscopic equipment and dilators resulting in improve safety of esophageal dilatation,16 esophageal perforation remains one of the major complication of dilatation. The incidence of perforation is influenced by the underlying cause of stricture, technique of dilatation, equipment and the expertise of the endoscopist. With bougies and balloon the incidence of perforation is reported to be 12-32%.8,17-19 There were four (14.8%) procedure related perforations in our study. This higher incidence of perforation was seen exclusively in corrosive induced strictures, which were long, eccentric and tight, thus technically more difficult to dilate. This observation correlates with the work done in India where like in Pakistan, corrosive ingestion strictures are more commonly seen as compared to the west. More over being a tertiary health care center, most complex and resistant strictures are referred, while simple strictures are being increasingly dealt with by primary or secondary health care centers.
The mortality related to esophageal perforation depends on time to recognize the underlying cause. Patients in whom perforation is recognized immediately have a good prognosis whereas a delay of beyond 24 hours leads to a high mortality of 25-50%.20,21 All four patients with perforation were young, having long strictures which started from upper esophagus with involvement of stomach, due to the extensive damaged caused by corrosives. All such strictures are resistant and difficult to dilate, resulting in increased risk of perforation. In our study, the perforations in all four patients were diagnosed immediately and were managed conservatively. Out of four, two patients died because of sepsis. Amongst the remaining two, one patient had self expandable metallic stent placed and the opening became small and finally closed over a period of time. The second also responded to conservative treatment resulting in spontaneous closure after four weeks. Dilatation was resumed in both the patients. The over all mortality in this study was 7.4%. An audit conducted at UK reported an overall perforation rate of 2.6% with a mortality of 1%. Singhal S15 and Andreollo NA22 reported complication rate of 0.56% vs 1.2%. A local study of 369 patients1 with a short follow up reported no significant complications but their experience with dilatation of corrosive was limited to only 6/369 (1.6%).
Conclusion
Corrosive strictures were more frequently seen in younger age group. Endoscopic dilatations proved safe and effective in benign strictures with a low recurrence rate.
References
1.Khokar N, Gill LM, Khan MM. Endoscopic Dilatation of Esophageal Strictures. J Coll Physicians Surg Pak 2003; 13: 555-7.
2.Patterson DJ, Graham DY, Smith JL, Schwartz JT, Alpert E, Lanza FL, et al. Natural history of benign esophageal strictures treated by dilatation. Gastroenterology 1983; 85: 346-50.
3.Marks RD, Richter JE. Peptic strictures of the esophagus. Am J Gastroenterol 1993; 88: 1160-73.
4.Lahoti D, Broor SL. Corrosive injury to upper gastrointestinal tract. Indian J Gastroenterol 1993; 12: 135-41.
5.Broor SL, Kumar A, Chari ST, Singal A, Misra SP, Kumar N, et al. Corrosive esophageal strictures following acid ingestion: clinical profile and results of endoscopic dilatation. J Gastroenterol Hepatol 1989; 4: 55-61.
6.Zargar SA, Kocher R, Nagi B, Mehta S, Mehta SK. Ingestion of corrosive acids. Spectrum of injury in upper gastrointestinal tract and natural history. Gastroenterolgy 1989; 97: 702-7.
7.Cox JCG, Winter RK, Maslin SC, Jones R, Buckton GK, Hoare RC, et al. Balloon or bougie for dilatation of benign esophageal stricture? An interim report of a randomiazed controlled trial. Gut 1988; 29: 1741-7.
8.Barkun AN, Mayrand S. The treatment of peptic esophageal strictures. Can J Gastroenterol 1997; 11(Suppl B): 94-7.
9.Gerzic ZB, Knezevic JB, Milicevic MN, Jovanvic BK. Esophagocoloplasty in the management of postcorrosive stricture of the esophagus. Ann Surg 1990; 211: 329-36.
10.Hussain SZ, Thomas R, Tolia V. A review of achalasia in 33 children. Dig Dis Sci 2002; 47: 2538-43.
11.Reynold JC, Parkman HP. Achalasia. Gastroenterol Clin North Am 1989; 18: 223-55.
12.Dilawari JB, Singh S, Rao PN, Anand BS. Corrosive acid ingestion in man - a clinical and endoscopic study. Gut 1984; 25: 183-7.
13.Ilkin Naharci M, Tuzun A, Erdil A, Ates Y, Bagci S, Yamanel L, et al. Effectiveness of bougie dilation for the management of corrosive esophageal strictures. Acta Gastroenterol Belg 2006; 69: 372-6.
14.Broor SL, Raju GS, Bore PP, Lahoti D, Ramesh GN, Kumar A, et al. Long term results of endoscopic dilatation for corrosive esophageal strictures. Gut 1993; 34: 1498-501.
15.Singhal S, Kar P. Management of acid and alkali induced esophageal strictures in 79 adults by endoscopic dilation: 8 years experience in New Delhi. Dysphagia 2007; 22: 130-4.
16.Standards of Practice Committee, Egan JV, Baron JH, Adler DG, Davila R, Faigel DO, Gan SL, et al. Esophageal dilatation. Gastrointest Endosc 2006; 63: 755-60.
17.Zaninotto G, DeMeester T, Bremmer CG, Smyrk TC, Cheng SC. Esophageal function in patients with reflux induced strictures and its relevance to surgical treatment. Ann Thorac Surg 1989; 47: 362-70.
18.Bischof G, Feil W, Riegler M, Wenzl E, Schiessel R. Peptic esophageal stricture: is surgery still necessary? Wien Klin Wochers Chr 1996; 108: 267-71.
19.Khan R, Abid S, Hamid S, Abbas Z, Shah H, Jafri W. Outcome of Endoscopic therapeutic interventions: are they different among various non-malignant esophageal diseases? J Ayub Med Coll Abottabad 2005; 17: 22-5.
20.Bladergroen MR, Lowe JE, Postlehwait RW. Diagnosis and recommended management of esophageal perforation and rupture. Ann Thorac Surg 1986; 42: 235-9.
21. Shaffer HA Jr, Valenzvela G, Mittal RK. Esophageal perforation. A reassessment of the literature for choosing medical or surgical therapy. Arch Intern Med 1992; 152: 757-61.
22.Andreollo NA, Lopes LR, Inogutti R, Brandalise NA, Leonardi LS. [Conservative management of benign esophageal strictures using dilation. Analysis of 500 cases.] Rev Assoc Med Bras 2001; 47: 236-43.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: