
Rana Shoaib Hamid ( Radiology Department, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan. )
Tanveer-ul-Haq ( Radiology Department, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan. )
Ishtiaq Chishti ( Radiology Department, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan. )
Muhammad Azeemuddin ( Radiology Department, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan. )
Zafar Sajjad ( Radiology Department, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan. )
Basit Salam ( Radiology Department, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objective: To evaluate the technical success, safety and outcome of endovascular coiling procedure in intracranial aneurysms.
Methods: From April 2003 to April 2009, 43 patients (23 males and 20 females), age range 11 to 70 years, mean age 46.67 ± 11.57 years were treated for intracranial aneurysms by detachable coil deployment at Radiology Department of Aga Khan University Hospital. Aneurysm rupture with subarachnoid haemorrhage was the cause of presentation in 39 patients while 4 patients were diagnosed with un-ruptured aneurysms. At time of presentation, grading of subarachnoid haemorrhage was done according to Hunt and Hess grading system. Eleven patients presented with Grade I haemorrhage, other 11 presented with grade II haemorrhage, 8 patients had grade III haemorrhage and 9 patients had grade IV haemorrhage. Preliminary diagnostic workup was performed by cross sectional imaging, CT angiography or digital substraction angiography. Coiling procedures were performed under general anaesthesia through femoral artery approach. Detachable platinum coils were densely packed in all aneurysms by endovascular technique. Patient files and radiology reports were retrospectively reviewed. Technical success and safety of the procedure were analyzed. Modified Rankin Score was used to determine clinical outcome. Score 0-2 represented good outcome, score 3-5: dependency (Can not attend own bodily needs and carry out daily activities without assistance) and score 6: death.
Results: Aneurysm size ranged from 3mm - 22mm (mean size 8 mm ± 4). 74.4% aneurysms had narrow necks while 25.6% aneurysms were wide necked. Most common aneurysm site was anterior communicating artery. Technical success rate for endovascular intracranial aneurysm coiling was 95.3 % (n = 41). Major complication rate was 11.6 % (n = 5). Mortality rate was 2.3% (n = 1). 78 % patients showed good clinical outcome after coiling including 4 patients with un ruptured aneurysms (n = 32).
Conclusion: Results of endovascular aneurysm coiling at our center showed high technical success rate (95.3%) and good short term clinical outcome in 78% patients (JPMA 60:638; 2010).
Introduction
Intracranial aneurysm is not an uncommon entity, with a prevalence of 0.5% to 6% in adults in general population.1 They are multiple in 10 -30% of cases. Although most aneurysms are small but they can lead to substantial morbidity and mortality. Most common presentation is rupture leading to subarachnoid haemorrhage.2 Approximately 27,000 new cases of subarachnoid haemorrhage due to aneurysm rupture present each year in United States.3 In Pakistani population frequency of sub-arachnoid haemorrhage as a cause of stroke is estimated to be 8-10%.4,5
Patients with ruptured aneurysms present with severe headache, coma or with severe neurologic compromise. More than 10% patients die before reaching hospital.3 Over all 50% patients die within first month from progressive deterioration. Approximately 30 percent of survivors have moderate-to-severe disability.6 Ruptured aneurysms may bleed again within 24 hours of initial episode and risk remains high in initial 2 weeks.2 Patients with un-ruptured aneurysms can present with symptoms due to mass effect, resulting in cranial-nerve palsies or brain-stem compression. Prompt diagnosis with timely treatment of aneurysm is associated with improved prognosis.
Intracranial aneurysms are now increasingly treated by endovascular coiling. A microcatheter is positioned into the aneurysm, and detachable coils are deployed to decrease the amount of blood or to stop blood from filling the aneurysm.7 This technique is rapidly becoming primary option for the treatment of aneurysms.8
In Pakistan, the outcome of surgical clipping of aneurysms has been studied locally in the past9 but to the best of our knowledge no local data is available regarding outcome of endovascular coiling as treatment modality.
We evaluated the technical success, safety and outcome of endovascular coiling procedure in intracranial aneurysms.
Patients and Methods
This retrospective study was carried out at radiology department of Aga Khan University Hospital. Data of patients was collected from April 2003 to April 2009.We included all patients who underwent coiling procedure for intracranial aneurysm. Patients in whom coiling was technically not possible due to difficult anatomy or severe vascular spasm were excluded from the study.
Sample comprised of total 43 patients (23 males and 20 females) age range was from 11 to 70 years, mean age 46.67 ± 11.57 years. Thirtynine (90.69%) patients presented with subarachnoid haemorrhage due to ruptured aneurysms while 4 (9.3%) patients had symptoms due to unruptured intracranial aneurysms. At time of presentation subarachnoid haemorrhage in 39 patients was graded according to Hunt and Hess grading system.10 Eleven patients presented with Grade I haemorrhage, other 11 presented with grade II haemorrhage, 8 out of 39 patients had grade III haemorrhage and 9 patients had grade IV haemorrhage. Standard four vessels cerebral angiogram was performed supplemented by rotational and 3D angiography prior to the coiling procedure. Location, size, orientation, neck diameter, and shape of intracranial aneurysm. were analyzed. Narrow neck of aneurysm was defined as less than 50% neck to body ratio and wide necked aneurysms were defined as those with more than 50% neck to body ratio.
Coiling Procedure: Procedures were performed by senior interventional radiologist in angiography suite on a monoplane flat panel DSA unit (Axiom Artis angiography machine Siemen\'s corporation). All procedures were carried out under general anaesthesia via femoral artery approach. Following diagnostic angiography by 5 Fr H1 catheter (Cordis corporation), a 6 Fr guiding catheter (MPD, Cordis corporation) was placed in internal carotid artery as distally as possible and after selective catheterization of aneurysm with micro-catheter (Prowler, Cordis corporation), multiple detachable coils (GDC, Boston Scientific or TRUFIL, Cordis corporation) were deployed for embolization. Dense packing of aneurysm was the end point for procedure (Figure-1).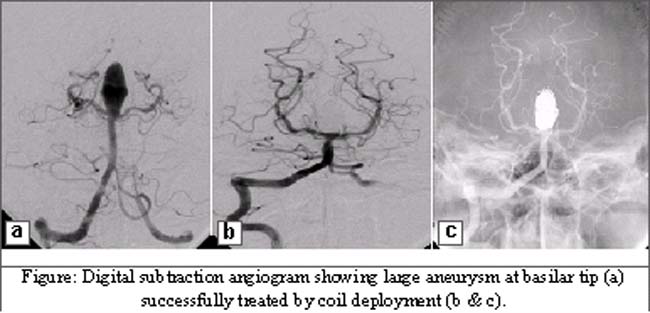
Technical failure was defined as an attempted embolisation procedure during which coils could not be successfully deployed. Any procedural or other subsequent complication was recorded. Patients were followed after procedure and Modified Rankin Score11 was used to determine clinical outcome.
Scores 0-2: Good out come
Scores 3-5: Dependency (Can not attend own bodily needs and carry out daily activities without assistance)
Score 6: Death
Data from patient\'s files and radiology reports was collected on performa and analyzed on SPSS version 16.
Results
Aneurysm size ranged from 3mm-22mm (mean size 8 ± 4 mm). 32 aneurysms had narrow necks while 11 aneurysms had wide necks. Most common aneurysm site was anterior communicating artery (30.2%). Frequency for distribution of location of aneurysm is outlined in Table.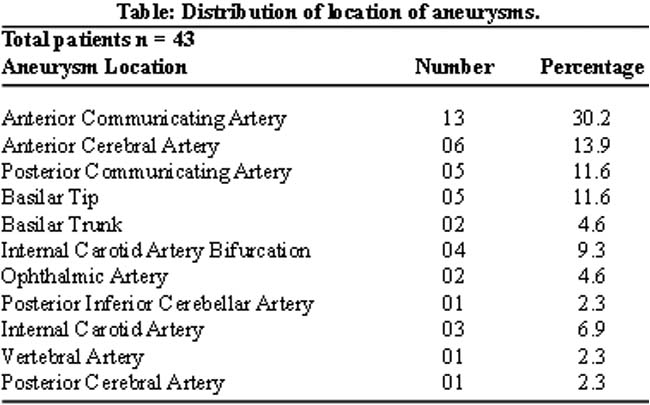
Technical success rate for endovascular intracranial aneurysm coiling was 95.3 % (41 out of 43 patients). In 2 patients the procedure was unsuccessful due to anatomically difficult catheterization of aneurysm or supplying artery. Major complication rate was 11.6 %. Aneurysm rupture occurred in 3 patients, 2 of them underwent subsequent surgical clipping. In 1 patient the ruptured aneurysm was immediately sealed by deployment of coil. In 3 patients thromboembolism occurred during attempts of cannulation of the native artery. Two of these patients developed established infarctions. In 3rd patient tiny thrombus was discovered in parent artery and was immediately treated with Nimodipine, Abciximab and Heparin infusion. No neurological deficit was observed in this patient.
One patient died after 2 days of coiling procedure due to infarct induced by intense vascular spasm. Out of 41 patients who underwent successful coiling of aneurysms, 32 (78%) showed good clinical outcome, this group includes all 4 patients with un-ruptured aneurysms. Six patients developed dependency (14.63%). Two patients were lost to follow-up after discharge from hospital.
Discussion
In the past, surgical clipping had been the mainstay of treatment of both ruptured and unruptured cerebral aneurysms. With development of newer interventional techniques and increasing experience of interventional radiologists, traditional concepts of aneurysm treatment have changed.12,13 Since the advent of Guglielmi detachable coils in 199114 the technique is being widely used as alternative treatment modality of intracranial aneurysms. It allows placement of platinum coils into lumen of the aneurysm blocking blood flow into the aneurysm and preventing rerupture. The technique is a safe and effective alternative treatment option with fewer complications, shorter hospital stay and faster recovery.15,16 Reported technical complications of coiling include parent artery occlusion, aneurysm perforation and coil migration.17
Major procedural complications in our series were 11.6%, similar to those reported by Renowden i.e. 12.4%.18 Two patients with ruptured aneurysms underwent successful surgical clipping. Surgical intervention can be a helpful second line treatment in cases of unsuccessful or complicated coiling procedure.19 One patient in our series had a tiny thrombus in native artery which was managed successfully by Abciximab, nimodipne and heparin infusion. Mortality rate related to procedural complications or technical failure is variable, ranging from 0.6-29%.20-22 In our series mortality rate was 2.3% which is comparable to published literature.
Regarding eventual patient outcome, a large multi center prospective study of 2143 patients with ruptured intracranial aneurysms, by Molyneux8 showed favourable results for endovascular therapy as compared to surgery. The relative risk of significant disability at one year for patients treated with coils was 22.6 percent lower than in surgically-treated patients. Yu23 have also demonstrated lower risk of death and significant disability in patients treated with coiling procedures as compared to surgically treated group. In our series 78% patients showed good clinical outcome after endovascular management, our results in this regard are better than Jahromi24 and quite similar to Sluzewski25 (63% and 84% respectively).
The procedural success rates, safety and eventually patient outcome is expected to improve further with increasing experience of interventional radiologists and availability of multidimensional coils allowing safer initial deployment.
Conclusion
Results of endovascular aneurysm coiling at our center showed high technical success rate and good short term clinical outcome.
References
1.Schievink WI. Intracranial aneurysms. N Engl J Med 1997; 336: 28-40.
2.Greenberg MS. SAH and aneurysms. In: Greenberg MS, ed. Handbook of neurosurgery. 5th ed. New York: Thieme Medical 2000: 754-803.
3.Wijdicks EF, Kallmes DF, Manno EM, Fulgham JR, Piepgras DG. Subarachnoid haemorrhage: neurointensive care and aneurysm repair. Mayo Clin Proc 2005; 80: 550-9.
4.Qureshi FS, Bilal A, Khan RR, Khalid G. Stroke; frequencies of intra-cerebral bleed, cerebral infarction and sub-arachnoid haemorrhage. Professional Med J 2007; 14: 580-5.
5.Siddiqui AM, Ali A, Masrur S, Monga MA, Tauqeer A, Rehman KU. Clinical Audit of Patients with CVA in Medical Unit-I, Jinnah Hospital, Lahore. Ann King Edward Med Coll 2001; 7: 79-82.
6.Johnston SC, Selvin S, Gress DR. The burden, trends, and demographics of mortality from subarachnoid haemorrhage. Neurology 1998; 50: 1413-8.
7.Debrun GM, Aletich VA, Thornton J, Alazzaz A, Charbel FT, Ausman JI, et al. Techniques of coiling cerebral aneurysms. Surg Neurol 2000; 53: 150-6.
8.Molyneux A, Kerr R; International Subarachnoid Aneurysm Trial (ISAT) Collaboration Group, Stratton I, Sandercock P, Clarke M, Shrimpton J, Holman R. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. J Stroke Cerebrovace Dis 2002; 11: 304-14.
9.Ahmed M, Vohra AH. Surgical outcome of multiple intracranial aneurysms. Ann King Edward Med Coll 2005; 11: 489-91.
10.Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg 1968; 28: 14-20.
11.Rankin J. Cerebral vascular accidents in patients over the age of 60. II. Prognosis. Scott Med J 1957; 2: 200-15.
12.Horowitz MB, Levy E, Kassam A, Purdy PD. Endovascular therapy for intracranial aneurysms: a historical and present status review. Surg Neurol 2002; 57: 147-58.
13.Wanke I, Doerfler A, Dietrich U, Egelhof T, Schoch B, Stolke D, et al. Endovascular treatment of unruptured intracranial aneurysms. AJNR Am J Neuroradiol 2002; 23: 756-61.
14.Guglielmi G, Vinuela F, Dion J, Duckwiler G. Electrothrombosis of saccular aneurysms via endovascular approach. Part 2: Preliminary clinical experience. J Neurosurg 1991; 75: 8-14.
15.Johnston SC, Dudley RA, Gress DR, Ono L. Surgical and endovascular treatment of unruptured cerebral aneurysms at university hospitals. Neurology 1999; 52: 1799-805.
16.Johnston SC, Wilson CB, Halbach W, Higashida RT, Dowd CF, McDermott MW, et al. Endovascular and surgical treatment of unruptured cerebral aneurysms: comparison of risks. Ann Neurol 2000; 48: 11-9.
17.Vinuela F, Duckwiler G, Guglielmi G. Guglielmi detachable coil embolization of intracranial aneurysms. J Stroke Cerebrovasc Dis 1997; 6: 249-52.
18.Renowden SA, Benes V, Bradley M, Molyneux AJ. Detachable coil embolisation of ruptured intracranial aneurysms: a single center study, a decade experience. Clin Neurol Neurosurg 2009; 111: 179-88.
19.Klein O, Colnat-Coulbois S, Civit T, Auque J, Bracard S, Pinelli C, Marchal JC. Aneurysm clipping after endovascular treatment with coils: a report of 13 cases. Neurosurg Rev 2008; 31: 403-10.
20.Van Rooij WJ, Sluzewski M. Procedural morbidity and mortality of elective coil treatment of unruptured intracranial aneurysms. AJNR Am J Neuroradiol 2006; 27: 1678-80.
21.Viñuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 2008; 108: 832-9.
22.Lanterna LA, Tredici G, Dimitrov BD, Biroli F. Treatment of unruptured cerebral aneurysms by embolization with guglielmi detachable coils: case-fatality, morbidity, and effectiveness in preventing bleeding--a systematic review of the literature. Neurosurgery 2004; 55: 767-75.
23.Yu SC, Wong GK, Wong JK, Poon WS. Endovascular coiling versus neurosurgical clipping for ruptured intracranial aneurysms: significant benefits in clinical outcome and reduced consumption of hospital resources in Hong Kong Chinese patients. Hong Kong Med J 2007; 13: 271-8.
24.Jahromi BS, Mocco J, Bang JA, Gologorsky Y, Siddiqui AH, Horowitz MB, et al. Clinical and angiographic outcome after endovascular management of giant intracranial aneurysms. Neurosurgery 2008; 63: 662-74.
25.Sluzewski M, van Rooij WJ, Rinkel GJ, Wijnalda D. Endovascular treatment of ruptured intracranial aneurysms with detachable coils: long-term clinical and serial angiographic results. Radiology 2003; 227: 720-4.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: