
Afshan Wasti ( Department of Biochemistry, Jinnah University for Women, Karachi. )
Nikhat Ahmed Siddiqui ( Neurochemistry Research Unit, Department of Biochemistry, University of Karachi, College of Medicine, Qassim University, Qassim, Saudi Arabia. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objective: To investigate the alterations in different neurotransmitters particularly dopamine and serotonin in various regions of rat brain.
Methods: By using HPLC-ECD, the concentration of dopamine, their metabolites (DOPAC, HVA), serotonin, their precursor (tryptophan), and metabolites (5-HIAA) were determined in different regions such as hypothalamus, cortex, midbrain and striatum. In addition, tryptophan pyrrolase enzyme activity and the concentration of tryptophan were also determined in liver samples, following chronic (21 days I/M) treatment of haloperidol and clozapine (of both commercially available and purified form) in an animal model.
Results: Significant alterations were observed in the level of neurotransmitters in different regions of rat brain. In response to haloperidol treatment, the level of dopamine was observed to be significantly increased in hypothalamus, cortex and striatum but in midbrain the concentration was slightly decreased, While a significant increase (p<0.05) in the level of serotonin was observed in midbrain, hypothalamus and striatum. However, treatment with clozapine resulted in significant decrease in the level of dopamine in all the regions except cortex; with concurrent decrease observed in serotonin level in all brain regions except cortex where its concentration was slightly increased.
Liver demonstrated a significant increase (p<0.05) in the concentration of tryptophan, however, a slight increase was found in the concentration of brain tryptophan following haloperidol treatment. A marked decrease was observed in the concentration of liver tryptophan, whereas, the brain tryptophan concentration is significantly increased (p<0.05) in response to clozapine treatment. Marked increase was observed in the tryptophan pyrrolase enzyme activity, plotted against time at the time interval of 15 minutes in response to both haloperidol and clozapine treatment.
Conclusion: We suggest that the varying effect of these drugs on neurotransmitter may account for the difference in the consequence profile in response to chronic treatment (JPMA 60:628; 2010).
Introduction
An association between certain psychotic illnesses (including migraine, depression and schizophrenia), disturbance in amine metabolism in the brain and an abnormality in the methylation of biogenic amines (particularly serotonin/dopamine) in schizophrenia has long been considered.1,2 There is also evidence that excessive release of the putative neurotransmitter dopamine (DA) and deficiency in serotonin (5-HT) function is associated with schizophrenia.3
Some areas of the brain such as cortex, mid-brain, striatum, hippocampus, are thought to be important, as they provide a specific site for the action of antipsychotic drugs depending on the presence of the different neurotransmitter receptors like 5-HT2A and DRD2. Moreover, the effect of atypical antipsychotic, as predicted by multi receptor hypothesis, is either by appropriate modulation of the D2 receptor alone, or by blockade of other receptors. It is noteworthy that the atypical antipsychotic effect, previously reported by neuroimaging data, is mediated by optimal D2 receptor occupancy while the atypicality is lost in the presence of high 5-HT2 occupancy. The antipsychotic effect becomes more accommodating depending upon the fast dissociation from the D2 receptor regulating the physiological transmission of dopamine.4
Balancing efficacy and the side effect profile via transient D2 antagonism seems to be crucial to obtain antipsychotic effects by the optimal occupancy of D2 receptor, as the permanent D2 receptor antagonism by typical antipsychotic like haloperidol enhances the risk of adverse effect such as EPS. However, the balance between pre and post synaptic D2 receptor is known to exert by an inhibitory effect of serotonergic afferent neurons by synapsing with dopaminergic neurons.5
The proposed general mechanism of atypical antipsychotic drugs is the serotonin receptor antagonism contributing to the low extrapyramidal side effect profile6,7 however; the classical antipsychotic drugs have the potential to induce extrapyramidal side effects by dopaminergic receptor blockade.8,9 Serotonergic modulation has been associated with the increased release of striatal dopamine, as dopamine release in the prefrontal cortex can affect the negative and cognitive symptoms of schizophrenia and can be modulated either by the combined 5-HT2A/D2 receptor antagonism or the preferential blockade of inhibitory dopamine auto receptors or D2 receptor antagonism.5 All these contradictory observations lead to the postulation of "Serotonin Hypothesis of Schizophrenia" that aims to explain the hyperactivity syndrome (schizophrenia) on the basis of increased serotonin and tryptophan level.10 The hypo functioning of dopaminergic neurotransmission in medial prefrontal cortex alleviated by clozapine and other antipsychotic drugs were associated with the symptoms of schizophrenia.11
Noradrenaline has been shown to control dopamine turnover and release in rat brain. The extra-cellular noradrenaline was increased in the medial prefrontal cortex after administration of antipsychotics and was explained by inhibition of 5-HT2 receptor and not dopamine D2 receptors.12
Tryptophan and serotonin were considered as natural alternatives to traditional antidepressants, which can be used to resolve unipolar depression.13 The central role of multifold behavioural regulation played by serotonin and tryptophan peripheral concentration was also important for normal functioning of serotonin neurotransmission, which was in turn adjusted by hepatic and non-hepatic tryptophan pyrrolase and release of tryptophan from albumin and its passage across the blood-brain barrier. Increase in the free pool of tryptophan has been reported to increase the brain serotonin level moreover following diet-induced increase in tryptophan could increase the brain serotonergic activity.14
Liver tryptophan pyrrolase was considered as one of the principal factor that affects brain serotonin synthesis by altering the availability of tryptophan to the brain, an inverse relation was observed.15 An impairment of brain kyneurenine pathway in schizophrenia has also been reported resulting in elevated kyneurenine levels. The increase kynurenate was a consequence of increased tryptophan turnover, which results in low brain tryptophan, and hence serotonin levels in schizophrenics.16
This study depicts the neurobiological basis for the interaction between serotonin and dopamine system underlying the unique clinical profiles of haloperidol and clozapine, to illustrate its clinical relevance in the schizophrenic patients, parallel to the regional differences in the level of neurotransmitters in an animal model.
Materials and Methods
This study was conducted during January 2006 to May-2007 at the Neurochemistry Research Unit, Department of Biochemistry, University of Karachi and the Aga Khan University Hospital Karachi.
HPLC- ECD (Antec-leyden liquid chromatograph system) was used to determine the concentration of biogenic amines, nor epinephrine (NE), dopamine (DA) and 5-hydroxytryptamine (5-HT) and their metabolites, dihydroxyphenyl acetic acid (DOPAC), homovallenic acid (HVA) and 5-hydroxyindoleaceticacid (5-HIAA) in cortex, striatum, mid brain, hypothalamus and hippocampus of rat brain after appropriate treatment with haloperidol and clozapine.17 The brain tissues were excised and dissected into desired regions immediately after decapitation on an ice chilled glass plate and were stored at -70ºC until further analysis. The tissue samples were weighed and homogenized in ice-cold extraction medium and were placed in ice for at least 15 minutes to achieve complete precipitation. Samples were then centrifuged at 4ºC for 20 minutes at 12000 rpm. The clear supernatant was collected and the concentration of bioamines was determined by HPLC equipped with electrochemical detector.
Antec-leyden liquid chromatograph was equipped with a 5µm Hypersil ODS column (150mm x4.6mm). The flow rate was maintained at 1.5ml/minute. Retention times (in parentheses) for the compounds were as follows: NE (2.5 minutes), DOPAC (4.25minutes), DA (5.5 minutes), 5-HIAA (12.25 minutes), HVA (19.5 minutes) and 5-HT (18.0 minutes). The biogenic amines and their metabolites were quantified using peak height in comparison with the standards. Data are expressed as ng/mg or pg/mg tissue (wet weight) and were analyzed by student\'s t-test.
Bloxam &Warren (1974) Spectrofluorometric (JASCO fluorometer) method was used for the estimation of tryptophan in brain and liver samples by measuring fluorescence at emission and excitation wavelength (l) 480/ 365nm respectively.
The activity of tryptophan pyrrolase in liver tissue homogenates was determined by UV Spectrophotometer, by measuring the formation of L-kyneurenine from L-tryptophan, at wave length (l max) 365nm (Feigelson & Greengard method 1961). Kyneurenine concentrations were calculated, plotted against time and enzyme activity was calculated as mmol of kyneurenine /hr/g of tissue from the slope. In addition the modification made in the method is the preparation of liver homogenate. 6g of fresh liver tissue were homogenized in 40ml of homogenate solution at 0ºC for 1 minute. Preparation of reaction mixture: 15ml of liver homogenate solution was incubated with 45 ml of substrate solution at 37ºC with constant shaking (180 oscillations/minute). The enzyme activity was measured at the time interval of 15 minutes ranging from 0 to 120 minutes. For this 3ml of reaction mixture was taken out and 2ml of metaphosphoric acid was added, shaken for 5 minutes and filtered. 1.5ml of NaOH was added to 2.5ml of filtrate and read at l max 365nm using Bousch and Lomb spectrometer 21.
Results
The assessment was carried out by using High performance liquid chromatography (HPLC-ECD), in rat brain regions such as cortex, midbrain, hypothalamus and striatum, after chronic administration of haloperidol (0.2mg/Kg; I/M) and clozapine (20mg/Kg; I/M). Moreover, double comparison between the commercially available and purified form of these drugs are also incorporated in the present study.
The chronic treatment with haloperidol (both commercially available injection form and purified powder) increased the concentration of extracellular dopamine in all regions (hypothalamus, cortex and striatum) except mid-brain (Figure 1 a - b).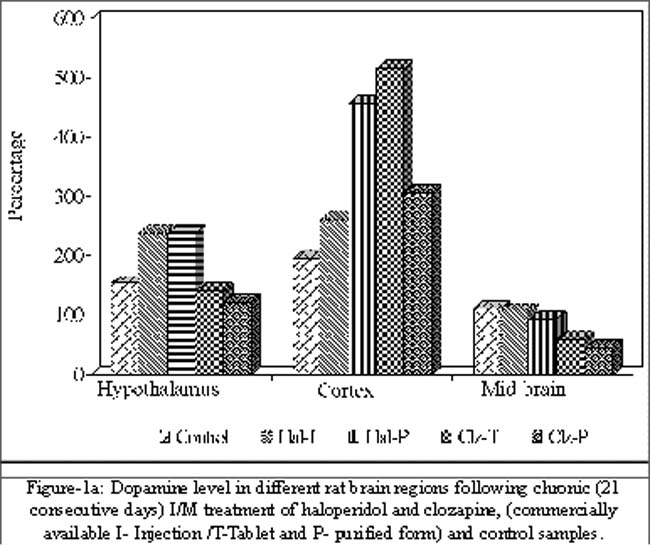
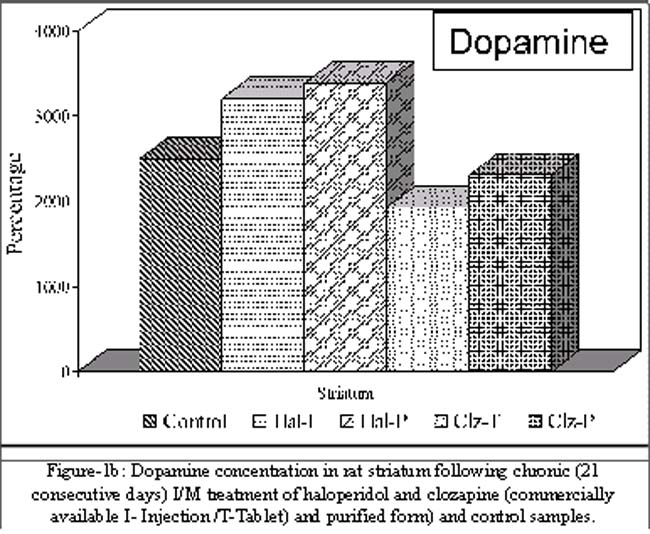
In contrast, treatment with clozapine resulted in marked decrease in dopamine concentration in all the regions except cortex in which the commercially available form of drug show marked increase (164.56%±82.7) in dopamine concentration. Furthermore, mid brain region showed significantly (p<0.05) the marked decrease (48.02%±5.09 and 61.4%±2.93) in both the experimental groups of clozapine treatment respectively (Figure-1 a-b).
The level of serotonin observed to be significantly (p<0.05) increased in midbrain, hypothalamus and striatum but slight decrease was observed in cortex (1.78% ± 26.9 and 6.99% ± 21.6) followed by the chronic treatment of commercially available tablet and purified powder of haloperidol respectively, as compared to control rats. The maximum increase in the serotonin concentration was observed in the experimental group treated with purified form of haloperidol in all three regions; midbrain (74.0% ± 23.3), hypothalamus (254.8% ± 21.4) and in striatum (227.8% ± 39.7) (Figure-2).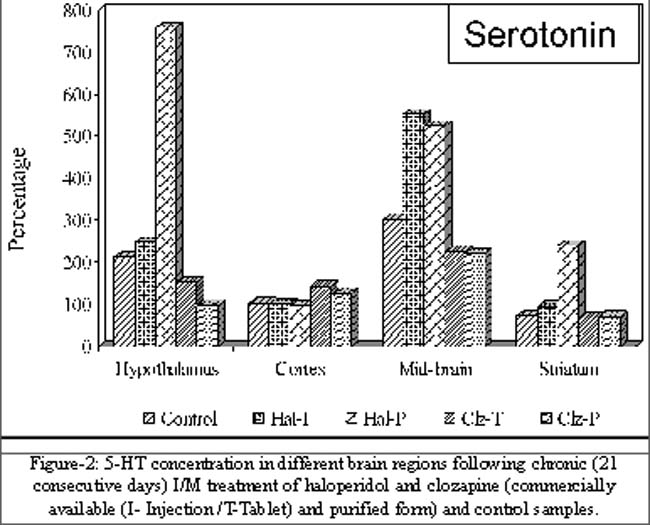
Concurrent decrease was observed in all regions after chronic treatment of clozapine except in cortex where serotonin concentration was markedly increased (39.32% ± 2.01 and 23.0% ± 4.2) in both the experiment groups. Additionally in hypothalamus, significant decrease (54.65% ± 9.5) was observed in the experimental group treated with the purified form of clozapine (Figure-2).
Liver demonstrated a significant increase (p<0.05) in the concentration of tryptophan (39.4% ± 0.09 and 65.28% ± 0.23) following haloperidol treatment in both the experimental groups. Whereas, a marked decrease was observed in the concentration of liver tryptophan (13.46% ± 0.05) in both the experimental groups treated with clozapine as compared to their respective controls. Moreover, slight increase was found in the concentration of brain tryptophan after the treatment of haloperidol in both the experimental groups. A significant increase (p<0.05) was observed in the brain tryptophan (16.6% ± 0.05) following treatment with purified form of clozapine. However slight increase (7.38% ± 0.04) was observed in the experimental group treated with commercially available form of clozapine as compared to their respective controls.
The assessment of liver tryptophan pyrrolase enzyme activity ( g/g/hr) in rats was carried out by using standard method. Kyneurenine levels ( g/g) were monitored in the liver tissues at a time interval ranged from 15 minutes to 120 minutes (Figure-3).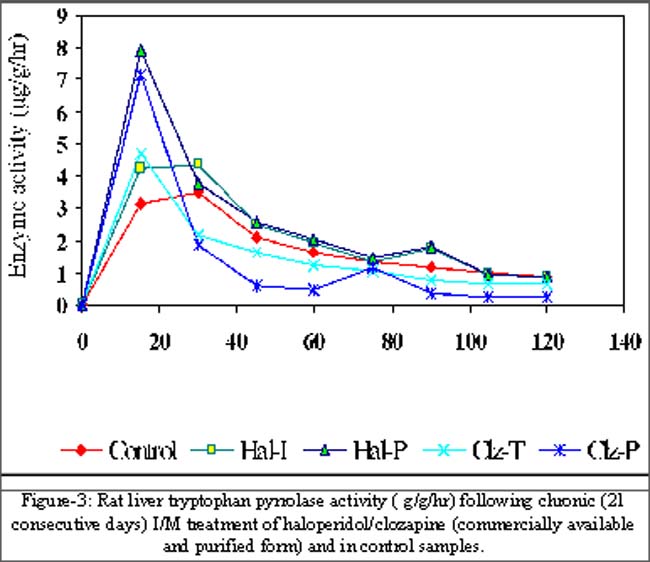
In addition, the enzyme activity was calculated from the slope as x/y * 60. Marked increase was observed in the enzyme activity, plotted against time at the time interval of 15minutes in response to both haloperidol and clozapine treatment in all the experimental groups of commercially available and purified form of treatment, as compared to their respective controls (Figure-3). For instance the increase in the tryptophan pyrrolase enzyme activity was significant (p<0.0001) in case of purified form of both haloperidol and clozapine as compared to their respective controls (Figure-3).
Discussion
In line with the key role of different brain regions and the clinical relevance of antipsychotic drugs, in psychiatric illnesses, the present study will review the evidences that pertain to the alterations in the level of monoamine particularly dopamine and serotonin after chronic treatment of antipsychotic drugs. The disparate side effects profile of haloperidol and clozapine underlies, in part, may be due to their differential affinity toward dopamine D2 receptors, since the therapeutic role of atypical antipsychotic drugs is related to the modulatory function of serotonergic (5-HT) system on dopamine transmission.1,2
Previous studies2 provide tentative evidence regarding the discrepancies related to the role of these neurotransmitters and their association both for and against in schizophrenia. However, the contribution of serotonin in the psychopathology of disease either directly or via alterations in the dopaminergic system remains elusive.3,7,18 An increase in sub cortical serotonin function is hypothesized to be associated with positive symptoms while the decrease in prefrontal serotonin function is linked to the negative symptoms.19 The hyper-dopaminergic function in the prefrontal cortex is associated with the negative or cognitive symptoms and can be modulated by combined D2 and 5-HT2 antagonisms.5 Additionally, the antipsychotic action is enhanced by an indirect effect in decreasing EPS, with concurrent activation leading to decrease symptoms of depression, as they all are associated with secondary negative symptoms.20
Haloperidol, a typical antipsychotic drug attenuate positive symptoms of schizophrenia by antagonism of D2 receptor in the mesolimbic while the concomitant blockade in striatal region is associated with the motor side effects such as EPS. In contrast, the distinctive functional profile of clozapine in controlling mood, cognition and motor behaviour is modulated by dopaminergic transmission.21
Significant increase was observed in the concentration of dopamine particularly in hypothalamus, cortex and striatum in response to the chronic treatment of haloperidol, but in midbrain the concentration is slightly decreased in both the experimental groups. However, treatment with clozapine resulted in significant decrease in all the regions except cortex in which the commercially available form of the drug showed marked increase in the concentration of dopamine. This is concurrent with the hypothesis suggesting inhibition of dopaminergic function via serotonergic system in the mid brain and forebrain, where most of the dopamine terminals are present, result in the release of dopamine by a serotonergic antagonists leading to the alleviation of antipsychotic-induced EPS through disinhibition of dopamine system in the striatum while in cortex it may lead to ameliorate negative symptoms provided superior efficacy to clozapine, in the treatment of schizophrenia.22
A significant increase in the level of serotonin was observed in midbrain, hypothalamus and striatum followed by the chronic treatment of haloperidol in both experimental groups as compared to control rats, however, in contrast with the findings of Ruch et al,23 1976, concurrent decrease was observed in all regions after chronic treatment of clozapine except in cortex where serotonin concentration were slightly increased.
To elevate brain tryptophan, peripheral tryptophan must also be increased as observed for liver tryptophan in the present study. Kozell et al, 198724 also reported increased serotonin levels in the brain after chronic antipsychotic drugs treatment, which was correlated significantly with the behavioural responses. Data shows a significant increase in tryptophan pyrrolase activity as well. Increased tryptophan in liver may account for this increased activity of tryptophan pyrrolase involving substrate -type enhancement.25 In brain the rate of serotonin synthesis is strongly influenced by the availability of plasma tryptophan and reduced levels of plasma tryptophan and CSF-5-HIAA have been reported in schizophrenia.14 The level of tryptophan, as it influences Kyneurenine (end product of tryptophan catabolism and 5-HT turnover in both brain and liver, could reflect the availability of the precursor tryptophan, in response to measure the differential effect of haloperidol and clozapine.
Conclusion
Given the concerns regarding the dysregulation in the level of neurotransmitters particularly dopamine and serotonin, in the context of treatment with typical or atypical medications, we observed significant alterations in the level of these neurotransmitters in different regions of rat brain. Furthermore, the regional analysis of these neurotransmitters are thought to be important, as they provide specific site for the action of antipsychotic drugs depending on the presence of the different neurotransmitter receptors like 5-HT2A, DRD2 etc. This study was carried out only in an animal model because it was not impossible to get the human schizophrenic brain samples in Pakistan. The CSF sample of these patients was also not available, however; the concentration of these bioamines in the serum or plasma samples was negligible.
Acknowledgment
The authors acknowledge the support of Prof. Dr. Anwar Ali Siddiqui, Associate Dean Research, Juma Research Lab, Aga Khan University Hospital Karachi, for providing the facility of HPLC used in the present study.
References
1.Meltzer HY. Role of serotonin in the action of atypical antipsychotic drugs. Clin Neurosci 1995; 3: 64-75.
2.Abi-Dargham A. Alterations of serotonin transmission in schizophrenia. Int Rev Neurobiol 2007; 78: 133-64.
3.Laruelle M, Abi-Dargham A, van Dyck C, Gil R, D\'Souza DC, Krystal J, et al. Dopamine and serotonin transporters in patients with schizophrenia: an imaging study with [(123)I]beta-CIT. Biol Psychiatry 2000; 47: 371-9.
4.Kapur S, Seeman P. Does fast dissociation from the dopamine d (2) receptor explain the action of atypical antipsychotics? A new hypothesis. Am J Psychiatry 2001; 158: 360-9.
5.Horacek J, Bubenikova-Valesova V, Kopecek M, Palenicek T, Dockery C, Mohr P, et al. Mechanism of action of atypical antipsychotic drugs and the neurobiology of schizophrenia. CNS Drugs 2006; 20: 389-409.
6.Segman RH, Goltser T., Heresco-Levy U, Finkel B, Shalem R, Schlafman M, et al. Association of dopaminergic and serotonergic genes with tardive dyskinesia in patients with chronic schizophrenia. Pharmacogenomics J 2003; 3: 277-83.
7.Mortimer AM. Novel antipsychotics in schizophrenia. Expert Opin Investig Drugs 2004; 13: 315-29.
8.WU SN, Gao R, Xing QH, Li HF, Shen YF, Gu NF, et al. Association of DRD2 polymorphisms and chlorpromazine-induced extrapyramidal syndrome in Chinese schizophrenic patients. Acta Pharmacologica Sinica 2006; 27: 966-70.
9.Gunes A, Scordo MG, Jaanson P, Dahl ML. Serotonin and dopamine receptor gene polymorphisms and the risk of extrapyramidal side effects in perphenazine-treated schizophrenic patients. Psychopharmacology (Berl) 2007; 190: 479-84.
10.Sharma RP, Shapiro LE, Kamath SK, Soll EA, Watanabe MD, Davis JM. Acute dietary tryptophan depletion: effects on schizophrenic positive and negative symptoms. Neuropsychobiology 1997; 35: 5-10.
11.Heidbreder CA, Foxton R, Cilia J, Hughes ZA, Shah AJ, Atkins A, et al.,. Increased responsiveness of dopamine to atypical, but not typical antipsychotics in the medial prefrontal cortex of rats reared in isolation. Psychopharmacology (Berl) 2001; 156: 338-51.
12.Westerink BH, Kawahara Y, De Boer P, Geels C, De Vries JB, Wikstrom HV, et al. Antipsychotic drugs classified by their effects on the release of dopamine and noradrenaline in the prefrontal cortex and striatum. Eur J Pharmacol 2001; 412: 127-38.
13.Shaw K, Turner J, Del Mar C. Tryptophan and 5-hydroxytryptophan for depression. Cochrane Database Syst Rev 2002; 1: CD003198.
14.Markus CR, Olivier B, de Haan EH. Whey protein rich in alpha-lactalbumin increases the ratio of plasma tryptophan to the sum of the other large neutral amino acids and improves cognitive performance in stress-vulnerable subjects. Am J Clin Nutr 2002; 75: 1051-6.
15.Allegri G. Ragazzi E, Bertazzo A, Costa CV, Rocchi R. Tryptophan metabolism along the kynurenin pathway in rats. Adv Exp Med Biol 2003; 527: 481-96.
16.Moller SE. Tryptophan to competing aminoacid ratio in depressive disorder: relation to efficacy of antidepressive treatments. Acta Psychiatr Scand Suppl 1985; 325: 3-31.
17.Wasti A, Ghani R, Manji MA. Haloperidol induced variations in hematological indices. Pak J Med Sci 2004; 20: 197-200.
18.Reynolds G. Receptor mechanisms in the treatment of schizophrenia. J Psychopharmacol 2004; 18: 340-5.
19.Breier A. Serotonin, schizophrenia and antipsychotic drug action. Schizophr Res 1995; 14: 187-202.
20.Carpenter WT Jr. Serotonin-dopamine antagonists and treatment of negative symptoms. J Clin Psychopharmacol 1995; 15: 30S-5S.
21.Quintin P, Thomas P. Efficacy of atypical antipsychotics in depressive syndromes. Encephale 2004; 30: 583-9.
22.Kapur S, Remington G, Jones C, Wilson A, DaSilva J, Houle S, et al. High levels of dopamine D2 receptor occupancy with low-dose haloperidol treatment: a PET study. Am J Psychiatry 1996; 153: 948-50.
23.Ruch W, Asper H, Burki HR. Effect of clozapine on the metabolism of serotonin in rat brain. Psychopharmacologia 1976; 46: 103-9.
24.Kozell L, Sandyk R, Wagner GC, Fisher H. The effects of L-tryptophan on haloperidol-induced movement disorder in the rat. Life Sci 1987; 41: 1739-44.
25.Cihak A, Lamar C Jr, Pitot HC. L-tryptophan inhibition of tyrosine aminotransferase degradation in rat liver in vivo. Arch Biochem Biophys 1973; 156: 188-94.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: