
Abdurrahman Mohammad Alqurashi ( Department of Microbiology, College of Medicine, King Faisal Uniersity, Dammam, Saudi Arabia. )
Manal Abu Twibah ( King Fahd Hospital of the University Al-Khobar, Saudi Arabia. )
August 2010, Volume 60, Issue 8
Original Article
Abstract
Objective: To evaluate the trends of ciprofloxacin resistance pattern in commonly isolated gram-negative bacteria over time in a Saudi Arabian teaching hospital.
Methods: A retrospective analysis was carried out for ciprofloxacin resistance patterns of 10089 isolates of gram-negative bacteria isolated from various clinical specimens submitted to microbiology laboratories at King Fahd Hospital of the University (KFHU), Alkhobar, Saudi Arabia during the period January 2002 to August 2005.
Results: Increase in ciprofloxacin resistance rates in these isolates during the years 2002 and 2005 were as follows: Escherichia coli, 23.85 to 33.1%; Klebsiella pneumoniae, 15.93 to 27.55%; Enterobacter cloacae, 12.32 to 18.05%; Enterobacter aerogenes, 4.16 to 25.64%; Pseudomonas aeruginosa 17.05 to 39.53%, Pseudomonas spp., 20.58 to 58.77%; H. influenzae, 00.00% to 11.11% and H. aegyptius, 00.00% to 1.73%.
Conclusion: There was a gradual increase in resistance from year 2002 to 2005 in most of the gram negative isolates i.e. E. coli, K. pneumoniae, E. cloacae, E. aerogenes, P. aeruginosa and Pseudomonas spp showing that ciprofloxacin is no more a drug of choice for gram negative infections by these microbes (JPMA 60:625; 2010).
Introduction
Over the last few decades the ever-increasing level of bacterial resistance to antimicrobials has been a cause of worldwide concern. This situation is aggravated by over the counter availability, and indiscriminate and inappropriate use of antimicrobial agents.1 It is well recognized that the increased use of ciprofloxacin has led to a progressive loss of its susceptibility,2,3 since its introduction for the treatment of a broad range of clinical conditions such as urinary tract infections, upper respiratory tract infections, as a prophylaxis in neutropenic patients and in poultry, resistant strains are on the increase.4,5 This is particularly seen among gram-negative bacteria.6 A major aspect of medical concern is the increasing ciprofloxacin resistance among E. coli and other Enterobacteriaceae.7-10
Surveillance studies are one of the main tools for resolving the problem of antimicrobial resistance, as they enable resistance patterns to be monitored and allow early detection of any potential resistance trends.1 In this study we aimed to highlight trends of resistance to ciprofloxacin among common gram negative organisms isolated in KFHU during the years January 2002 to August 2005.
Materials and Methods
A retrospective analysis was carried out for ciprofloxacin susceptibility patterns of gram-negative bacteria isolated from various clinical specimens submitted to microbiology laboratories at KFHU, Alkhobar, Saudi Arabia during the period from January 2002 to August 2005. Data of total of 10089 gram negative organisms [Escherichia coli (n=3953), Klebsiella pneumoniae (n=1962), Enterobacter cloacae (n=501), Enterobacter aerogenes (n=167), Pseudomonas aeruginosa (n=2561), Pseudomonas spp. (n=319), Haemophilus influenzae (n=258), and Haemophilus aegyptius (n=368)] was accessed from the hospital\'s computer system during the period January 2002 to August 2005. The bacterial isolates obtained on routine culture media were identified and their susceptibility testing was carried out by using the MicroScan Walk Away 96 system (Dade Behring Inc., West Sacramento, CA95691, USA). Intermediately susceptible strains were considered resistant.
Results
Ciprofloxacin resistance of gram negative isolates recovered from specimens at KFHU during the period January 2002 to August 2005 is given in the Table.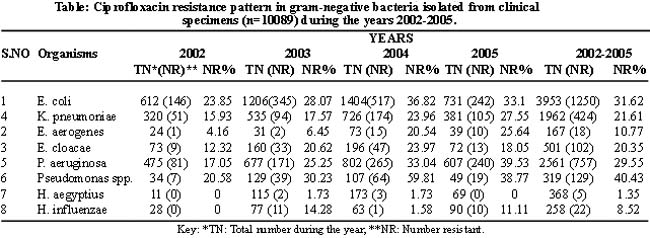
There was a gradual increase in resistance from year 2002 to 2005 in most of the gram negative isolates. For E. coli, resistance rates were 23.85, 28.07, 36.82 and 33.1% during the years 2002, 2003, 2004 and 2005 respectively. Resistance rates in other isolates during the same years respectively were as follows: K. pneumoniae, 15.93, 17.57, 23.96 & 27.55%; E. cloacae, 12.32, 20.62, 23.97 & 18.05%; E. aerogenes, 4.16, 6.45, 20.54 & 25.64%; P. aeruginosa, 17.05, 25.25, 33.04 & 39.53% and Pseudomonas spp., 20.58, 30.23, 59.81 & 38.77%. None of the isolates of H. aegyptius and H. influenzae was resistant during the year 2002. However, there was slight increase (1.73%) in resistance of the former and fluctuation in the later (14.28, 1.58 & 11.11%) during the years 2003-2005.
Discussion
There was a gradual increase in resistance from year 2002 to 2005 in most of the gram negative isolates i.e. E. coli, K. pneumoniae, E. cloacae, E. aerogenes, P. aeruginosa and Pseudomonas spp. This could be due to the increasing use of fluoroquinolones particularly ciprofloxacin in gram negative infections.3,7,8 Similar trend was reported in another study from Saudi Arabia carried out between years 2001 and 2005.11 However in our study, the rate of resistance was relatively higher but is comparable to a recent report from Saudi Arabian isolates from urinary tract infections.12 This could be due to difference in trend of ciprofloxacin prescription in different healthcare settings. These results are comparable with studies from United States, France, Germany, Italy, Spain, Canada, China and Taiwan.9,13-16
Pseudomonas spp. and P. aeruginosa showed high resistance rates (59.81% and 39.53%) like other studies.17 Very high resistance in E. coli (36.82%) and K. pneumoniae (27.55%) like other reports.18,19 could be due to the reason that ciprofloxacin being mostly used as oral agent may lead to resistance in local faecal flora and patients acquire infection with these resistant strains. Ciprofloxacin resistance in E. cloacae and E. aerogenes has increased more in our isolates (>23% & >25% respectively) than in another study (<10%)20 during the same time period which again can be attributed to variable prescription practices. Emergence of ciprofloxacin resistance in H. aegyptius and H. influenzae is also of concern. In 2002 none of these isolates was resistant like another study from Saudi Arabia,21 however fluoroquinolone non-susceptible H. influenzae isolates are reported.22 A high resistance (14.28%) in H. influenzae during the year 2004 is of particular concern.
During the time period lapsed after this study, ciprofloxacin resistance must have increased further as has been reported in a recent study where more than 80% of multidrug resistant gram negative rods were resistant to ciprofloxacin.10 Our study shows that ciprofloxacin can no more be used as empirical therapy in infections due to E. coli, K. pneumoniae, E. cloacae, E. aerogenes, P. aeruginosa and Pseudomonas spp. It is essential that those concerned be alerted to the possibility of a trend towards further increased resistance to ciprofloxacin, so that the judicious use of ciprofloxacin and its alternatives can be considered particularly in areas of high fluoroquinolone resistance rates like ours amongst gram-negative bacteria.23
References
1.Felmingham D, Washington J. Trends in the antimicrobial susceptibility of bacterial respiratory tract pathogens - findings of the Alexander Project 1992-1996. J Chemother 1999; Suppl 1: 5-21.
2.Sahm DF, Critchley IA, Kelly LJ, Karlowsky JA, Mayfield DC, Thornsberry C. et al. Evaluation of current activities of fluoroquinolones against gram-negative bacilli using centralized in vitro testing and electronic surveillance. Antimicrob Agents Chemother 2001; 45: 267-74.
3.Neuhauser MM, Weinstein RA, Rydman R, Danziger LH, Karam G, Quinn JP. Antibiotic resistance among gram-negative bacilli in US intensive care units: implications for fluoroquinolone use. JAMA 2003; 289: 885-8.
4.Barry AL, Fuchs PC, Pfaller MA, Allen SD, Gerlach EH. Prevalence of fluoroqinolone-resistant bacterial isolates in four medical centers during the first quarter of 1990. Eur J Clin Microbiol Infect Dis 1990; 9: 906-8.
5.Bazile- Pham- Khac S, Truong QC, Lafont JP, Gutmann L, Zhou XY, Osman M, et al. Resistance to fluoroquinolones in Escherichia coli isolated from poultry. Antimicrob Agents Chemother 1996; 40: 1504-7.
6.Thompson CJ. The global epidemiology of resistance to ciprofloxacin and the changing nature of antibiotic resistance: a 10-year perspective. J Antimicrob Chemother 1999; Suppl A: 31-40.
7.Livermore DM, James D, Reacher M, Graham C, Nichols T, Stephens P, et al. Trends in fluoroquinolone (ciprofloxacin) resistance in Enterobacteriaceae from bacteremias, England and Wales 1990-1999. Emerg Infect Dis 2002; 8: 473-8.
8.Al- Lawati AM, Crouch ND, Elhag KM. Antibiotic consumption and development of resistance among gram- negative bacilli in intensive care units in Oman. Ann Saudi Med 2000; 20: 324-7.
9.Ling TK, Xiong J, Yu Y, Lee CC, Ye H, Hawkey PM. Multicenter antimicrobial susceptibility survey of gram-negative bacteria isolated from patients with community-acquired infections in the people\'s republic of China. Antimicrob Agents Chemother 2006; 50: 374-8.
10.O\'Fallon E, Pop-Vicas A, D\'Agata E. The emerging threat of multidrug-resistant gram-negative organisms in long term care facilities. J Gerontol A Biol Sci Med Sci 2009; 64: 138-41.
11.Babay HAH (2007). Ciprofloxacin resistance among bacterial isolates in a teaching hospital in Riyadh, Saudi Arabia 2001-2005. Pak J Med Sc 2007; 23: 39-42.
12.Al-Tawfiq JA, Anani AA. Antimicrobial susceptibility pattern of bacterial pathogens causing urinary tract infections in Saudi Arabian Hospital. Chemotherapy 2009; 55: 127-31.
13.Jean SS, Teng LJ, Hsueh PR, Ho SW, Luh KT. Antimicrobial susceptibilities among clinical isolates of extended- spectrum cephalosporin-resistant gram-negative bacteria in a Taiwanese University Hospital. J Antimicrob Chemother 2002; 49: 69-76.
14.Karlowsky JA, Draghi DC, Jones ME, Thornsberry C, Friedland IR, Sahm DF. Surveillance for antimicrobial susceptibility among clinical isolates of Pseudomonas aeruginosa and Acinetobacter baunannii from hospitalized patients in the United States, 1998 to 2001. Antimocrob Agents Chemother 2003; 47: 1681-8.
15.Jones ME, Draghi DC, Thornsberry C, Karlowsky JA, Sahm DF, Wenzel RP. Emerging resistance among bacterial pathogens in the intensive care unit- a European and North American Surveillance study (2000-2002). Ann Clin Microbiol Antimicrob 2004; 3: 14.
16.de la Campa AG, Balsalobre L, Ardanuy C, Fenoll A, Perez-Trallero E, Linares J. Spanish Pneumococcal Infection Study Network G03/103. Fluoroquinolone resistance in penicillin-resistant Streptococcus pneumoniae clones, Spain. Emerg Infect Dis 2004; 10: 1751-9.
17.Hadadi A, Rasoulinejad M, Maleki Z, Yonesian M, Shinani Al, Kourorian Z. Antimicrobial resistance pattern of gram-negative bacilli of nosocomial origin at two university hospitals in Iran. Diagn Microbiol Infect Dis 2007; 60: 301-5.
18.Kader AA, Kumar A, Dass SM. Antimicrobial resistance patterns of gram-negative bacteria isolated from urine cultures at a general hospital. Saudi J Kidney Dis Transplant 2004; 15: 135-9.
19.Xiao Y, Wang J, Li Y; MOH National Antimicrobial Resistance Investigation Net. Bacterial resistance surveillance in China: a report from Mohnarin 2004-2005. Eur J Clin Microbiol Infect Dis 2008; 27: 697-708.
20.Al-Tawfiq JA Antony A, Abed MS. Antimicrobial resistance rates of Enterobacter spp.: a seven-year surveillance study. Med Princ Pract 2009; 18: 100-4.
21.Balkhy HH, Memish ZA, Shibl A, Elbashier A, Osoba A. In vitro activity of quinolones against S. pneumonia, H. influenza and M. catarrhalis in Saudi Arabia. East Mediterr Health J 2005; 11: 36-44.
22.Ohkoshi Y, Yokota S, Sato K, Hayashi T, Matsuda K, Kuwahara O, Akizawa H, Fujii N. Antibiotic susceptibility of Haemophilus influenzae strains isolated from various clinical sources in Hokkaido Prefecture, Japan. J Infect Chemother 2008; 14: 93-8.
23.Masterton RG. Ciprofloxacin resistance - \'early-warning\' signs from the MYSTIC surveillance programme? J Antimicrob Chemother 2002; 49: 218-20.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: