
Shabbir Asim ( Departments of Surgery, National University Hospital, Singapore. )
Lahiri Manjari ( Departments of Medicine, National University Hospital, Singapore. )
Mak Seck-wai Kenneth ( Departments of Surgery, National University Hospital, Singapore. )
Chang Russell Alexander ( Departments of Pathology, National University Hospital, Singapore. )
Khor Christopher ( Departments of Medicine, National University Hospital, Singapore. )
Khek-Yu Ho ( Departments of Medicine, National University Hospital, Singapore. )
June 2010, Volume 60, Issue 6
Case Reports
Abstract
Endoscopic ultrasonography guided fine needle aspiration is a useful diagnostic aid in evaluation of cystic pancreatic mass. We report our patient with pancreatic tuberculous abscess who presented with pyrexia, and was found to have cystic pancreatic mass on CT scan. Pancreatic tuberculous abscess was diagnosed with the help of endoscopic ultrasound (EUS)-guided fine needle aspiration cytology (FNAC), thereby obviating the necessity for surgery.
Introduction
Pancreatic tuberculosis was first reported in the literature in 1966.1 Being rare and often presenting with non-specific symptoms and/or an incidental abdominal mass that is detected on radiological imaging, it poses a great diagnostic challenge to clinicians. We report a case of pancreatic tuberculous abscess diagnosed with the help of endoscopic ultrasound (EUS)-guided fine needle aspiration cytology (FNAC).
Case Report
A 76-years old Chinese lady was admitted to our hospital with a four-week history of fever. She had a background history of pulmonary tuberculosis treated for 9 months thirty years ago. Upon admission, she complained of a vague epigastric pain that was non-radiating and not related to the intake of food. Apart from a fever of 38°C, physical examination was unremarkable. Investigations included a high white cell count of 18x0.5x109/L with polymorph neutrophilia, an elevated erythrocyte sedimentation rate (146mm/hr), a raised C-reactive protein (13.7mg/dl, normal 0- 1.0mg/dl), and an increased procalcitonin level (90.65 unit, normal 0-0.50). Her liver function tests and serum amylase were within normal limits. There was no pathogen detected on urine and blood cultures. Her chest X-ray showed right upper lobe apical fibrosis that was compatible with her past history of pulmonary tuberculosis. In view of the presence of persistent fever with abdominal pain and the absence of a definite source of sepsis, a CT scan of the abdomen was done. It showed a multiseptated cystic mass in the head of pancreas that encased the common hepatic artery. The porta-hepatis and left para-aortic lymph nodes were enlarged. Based on these findings, differential diagnoses of a cystic pancreatic tumour and a pancreatic abscess were made. The option of surgery was entertained. However, in view of the clinical picture favouring sepsis, and the patient\'s high operative risk, EUS with view to FNAC was performed to further define the mass and ascertain the diagnosis. EUS showed a 3cm x 2cm septated cystic mass in the head of pancreas with a normal main pancreatic duct and a normal common bile duct (Figure-1).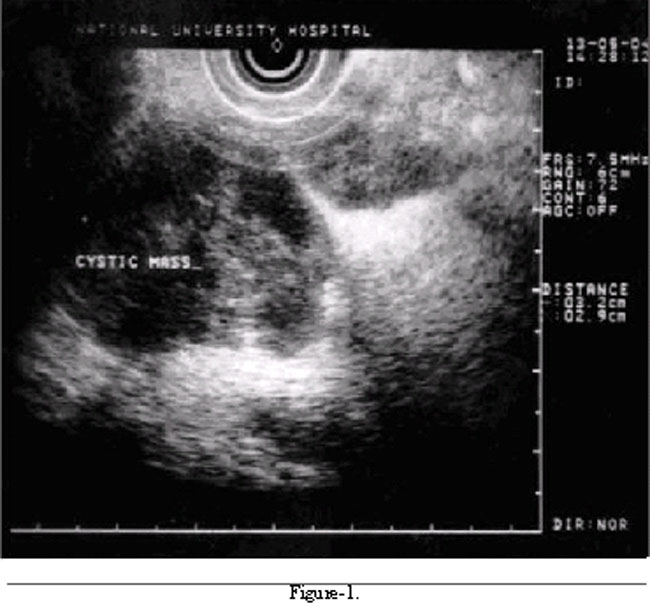
There was no distinct interface between the mass and the portal vein and superior mesenteric vein. Multiple enlarged lymph nodes were seen adjacent to the mass. Under antibiotic cover, EUS-guided FNA of the mass was done and this revealed pus, which was confirmed to be copious polymorphs on staining. Microscopic examination of the aspirated material showed abundant necrosis and groups of epithelioid cells, but Langhans\' giant cells were not present. However, occasional acid-fast bacilli were seen in the cellblock material retrieved from the needle washings (Figure-2).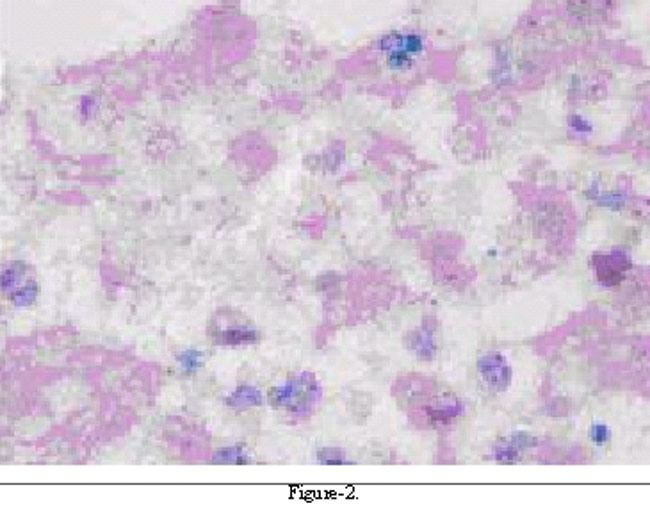
Material aspirated from a contiguous pancreatic lymph node showed a polymorph neutrophil infiltration. A diagnosis of pancreatic tuberculous abscess was made. The patient was promptly started on anti-tuberculosis therapy comprising isoniazid, rifampicin, and pyrazinamide with rapid improvement of her symptoms. On review 6 months later, she was well with no fever and was free of abdominal pain.
Discussion
Tuberculosis is most commonly diagnosed as a pulmonary disease. Pancreatic involvement is extremely rare. Pancreatic tuberculosis has been known to occur as an isolated entity or as part of a disseminated disease.2 Such reports emerge mostly from areas endemic in tuberculosis, e.g., developing countries in Asia. However, in recent years, developed countries too have reported this disease in immuno-compromised individuals due to the human immunodeficiency virus infection and other immunodeficiency states such as after liver and renal transplants.3 Pancreatic tuberculosis can present with a wide spectrum of symptoms, the most common being abdominal pain; others include gastrointestinal tract bleeding,4 diabetes mellitus,5 splenic vein thrombosis,6 and pancreatic abscess.7 In the case of pancreatic abscess, it can present as a pancreatic mass mimicking a cystic tumour of the pancreas,8 as was seen in our patient. The diagnosis of pancreatic tuberculous abscess is hard to establish. Blood investigations are not very helpful since inflammatory markers can be raised in malignancy as well. In cases with isolated pancreatic tuberculosis, chest X-ray may be normal or shows evidence of previous infection, which is a common but unhelpful finding in areas where tuberculosis is endemic. Indeed, scarring was noted in the right apical zone of one of our patient\'s chest X-ray, but this did not raise suspicion of the diagnosis since such findings are relatively common among the older population of our country. On imaging there are no distinctive features to differentiate between cystic pancreatic neoplasm and pancreatic tuberculosis. Takhtani et al reported radiological features of pancreatic tuberculosis in a series of three patients.9 Both ultrasound and computed tomography revealed a diffusely enlarged pancreas with focal hypoechoic and hypodense lesions, respectively. In addition, one patient had a large pancreatic cyst with internal echoes on ultrasonography. Associated findings included peripancreatic and mesenteric lymph nodes, bowel wall thickening at the ileocecal junction, focal hepatic or splenic lesions, splenic vein thrombosis, and ascites. They concluded pancreatic tuberculosis should be considered in the differential diagnosis of focal pancreatic lesions, especially if associated with ancillary findings such as enlarged nodes in the peripancreatic region or in the mesentery in patients presenting with longstanding fever and abdominal pain.9 In view of the non-specific and variable clinical presentation and atypical radiological signs, pancreatic tuberculosis is sometimes diagnosed in retrospect on laparotomy or after resection of suspicious pancreatic lesions. There are also case reports of diagnosis being based on finding of acid-fast bacilli after transabdominal image guided FNAC for inoperable and suspected cystic tumours.10 However, the diagnostic accuracy of the transabdominal approach is limited by the ability of these imaging modalities to clearly visualize the pancreatic lesion, and the technical difficulties associated with percutaneous aspiration of such a lesion. EUS-FNA of primary and metastatic pancreatic neoplasms have already been well described. We report here the use of EUS-FNA for the diagnosis of pancreatic tuberculous abscess. For our patients, we chose to use EUS because it gave the added advantage of being able to further characterize the mass in terms of resectability should the need arise to resect the lesion if it turned out to be a tumour. Above all EUS-FNA is a safe, quick, radiation-free, and relatively painless way of obtaining tissue for staining, cytology and culture. It may become the standard of care test in atypical cases with cystic pancreatic lesions where tissue is needed to resolve a diagnostic dilemma. In our institution a cytotechnologist is in attendance during image guided FNAC to make smears for instant examination to ascertain specimen adequacy, thus helping to restrict the number of aspiration passes to the minimum. A cytotechnologist also facilitates the harvesting of potentially useful diagnostic material that may be discarded such as blood clot and needle rinsings. This material can be used to make cellblocks, which are excellent for ancillary tests such as special stains or immunostaining. In our case the cellblock sections contained the all important acid-fast bacilli that helped clinch the diagnosis and graphically demonstrates the useful role of the cytotechnologist during FNAC. The logical approach to treating pancreatic tuberculosis is by anti-tuberculosis medications. Our patient responded very well to the anti- tuberculosis therapy and the lesion was found to have subsided on follow-up. The role of surgery in patients with pancreatic tuberculosis is very limited. However, prognosis is good even after surgical resection provided this is later followed by anti-tuberculosis therapy. The use of EUS-FNA for investigating cystic pancreatic lesions of unknown etiology that were later confirmed to be isolated pancreatic tuberculosis have recently been reported in 2 case reports.11,122 These reports also highlight the importance of high level of clinical suspicion followed by a EUS_FNAC diagnosis in order to avoid unnecessary surgical intervention. In summary, this report describes our patient with pancreatic tuberculous abscess diagnosed by EUS guided FNA, who was treated successfully with anti- tuberculosis pharmacotherapy, thus avoiding unnecessary surgery. We hope that the sharing of our experience will encourage others to consider this differential diagnosis as the threat of a resurgence of tuberculosis due to the human immunodeficiency virus infection looms ahead.
Acknowledgement
We wish to thank A/Prof Teh Meng for contributing the pathology slides.
References
1.Mann M, Stoger F. A rare case of tuberculosis of the pancreas treated by duodenopancreatectomy. Rozhl Chir 1996; 45: 96-9.
2.Ozden I, Emre A, Demir K, Balci C, Poyanli A, Ilhan R. Solitary pancreatic tuberculosis mimicking advanced pancreatic carcinoma. J Hepatobiliary Pancreat Surg 2001; 8: 279-83.
3.Coelho JC, Wiederkehr JC, Parolin MB, Balbi E, Nassif AE. Isolated tuberculosis of the pancreas after orthotopic liver transplantation. Liver Transpl Surg 1999; 5: 153-5.
4.Fan ST, Yan KW, Lau WY, Wong KK. Tuberculosis of pancreas: a rare cause of massive gastrointestinal bleeding. Br J Surg 1986; 73: 373.
5.Patankar T, Prasad S, Laxminarayan R. Diabetes mellitus: an uncommon manifestation of pancreatic tuberculosis. J Assoc Physicians India 1999; 47: 938-9.
6.Rezeig MA, Fashir BM, Al-Suhaibani H, Al-Fadda M, Amin T, Eisa H. Pancreatic tuberculosis mimicking pancreatic carcinoma: four case reports and review of literature. Dig Dis Sci 1998; 42: 329-31.
7.Jenney AW, Pickles RW, Hellard ME, Spelman DW, Fuller AJ, Spicer WJ. Tuberculous pancreatic abscess in an HIV antibody-negative patient: case report and review. Scand J Infect Dis 1998; 30: 99-104.
8.Fischer G, Spengler U, Neubrand M, Sauerbruch T. Isolated tuberculosis of the pancreas masquerading as a pancreatic mass. Am J Gastroenterol 1995; 90: 2227-30.
9.Takhtani D, Gupta S, Suman K, Kakkar N, Challa S, Wig JD, et al. Radiology of pancreatic tuberculosis: a report of three cases. Am J Gastroenterol 1996; 91: 1832-4.
10.Riaz AA, Singh A, Robshaw P, Isla AM. Tuberculosis of the pancreas diagnosed with needle aspiration. Scand J Infect Dis 2002; 34: 303-4.
11.Ahlawat SK, Pishvaian AC, Lewis JH, Haddad NG. Pancreatic tuberculosis diagnosed with endoscopic ultrasound guided fine needle aspiration. JOP 2005; 6: 598-602.
12.Cheng R, Grieco VS, Shuhart MC, Rulyak SJ. EUS-guided FNA diagnosis of pancreatic tuberculosis. Gastrointest Endosc 2006; 64: 660-3.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: