
Rana Shoaib Hamid ( Department of Radiology, Aga Khan University Hospital, Karachi, Pakistan. )
Tanveer ul Haq ( Department of Radiology, Aga Khan University Hospital, Karachi, Pakistan. )
Ishtiaq Chishti ( Department of Radiology, Aga Khan University Hospital, Karachi, Pakistan. )
Muhammad Azeemuddin ( Department of Radiology, Aga Khan University Hospital, Karachi, Pakistan. )
June 2010, Volume 60, Issue 6
Case Reports
Abstract
Lumbar arterial injury after trauma is a rare cause of significant retroperitoneal haemorrhage. Early diagnosis followed by endovascular transcatheter embolization is a very effective treatment to control bleeding in patients who do not respond to conservative management. We present a case of post traumatic avulsion of left fourth lumbar artery which was successfully treated with percutaneous transcatheter arterial embolization with glue.
Introduction
Pelvic and spinal fractures caused by blunt abdominal trauma are associated with significant mortality and morbidity.1 Pelvic retropenitoneal haemorrhage remains a major cause of death despite improvements in prehospital care resuscitation and increased therapeutic options.2 Upto 60% of such patients die due to significant haemorrhage secondary to vascular injury.1 Early CT scan followed by arteriography with selective embolization is recommended for the management. Embolization is a safe and effective method for immediate control of active extravasation, as well as to prevent future haemorrhage.3
Lumbar artery rupture is a rare and often overlooked cause of haemorrhage after pelvic and spinal trauma. We present a case of retroperitoneal haemorrhage due to rupture of lumbar artery successfully treated by endovascular embolization.
Case Report
A 31 year old patient was brought to the emergency department after sustaining abdominal trauma from a heavy steel door which fell on him. He was conscious but irritable, unable to sit or stand and had haemodynamic instability due to shock. His blood pressure was 90/60 mm Hg with a pulse rate of 110/min. Lower abdomen was soft but distended. His left leg was rotated and shortened. His Haemoglobin level was 5.3 G/dl. An ultrasound (FAST) was positive for minimal free fluid in peritoneal cavity. 3-D CT scan of pelvis showed diastasis of pubis with fractured pubic rami on right side. Fractures were also involving left sacral ala, bilateral transverse processes of lower lumbar vertebrae and neck of left femur. Contrast enhanced helical CT scan of abdomen and pelvis revealed a large retroperitoneal haematoma on left side extending from lumbar region into pelvis and also involving left psoas and ileus muscles.
Patient was resuscitated with blood transfusions, intravenous fluids, plasma expanders and fresh frozen plasma but his lower abdominal distension continued to increase and haemodynamic status worsened despite conservative management. Digital substraction angiography was planned to look for and embolize site of retroperitoneal haemorrhage. The angiogram of aorta (performed on Seimens Axiom Artis machine, through right femoral artery approach by 5Fr RDC catheter) was positive for active extravasation from ruptured left 4th lumbar artery from its origin (Figure-1).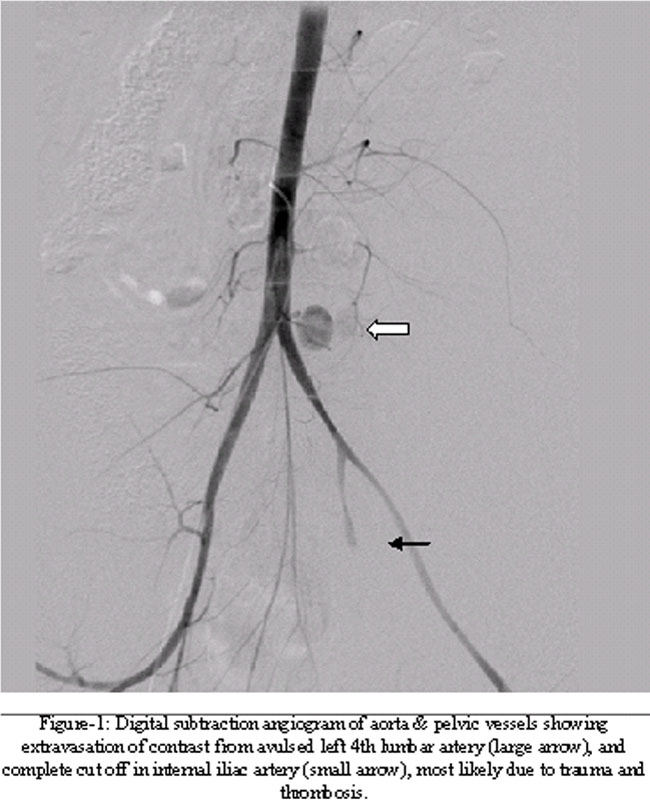
Complete embolization was performed with histoacryl (n-butyl-2-cyanoacrylate) glue (Figure-2).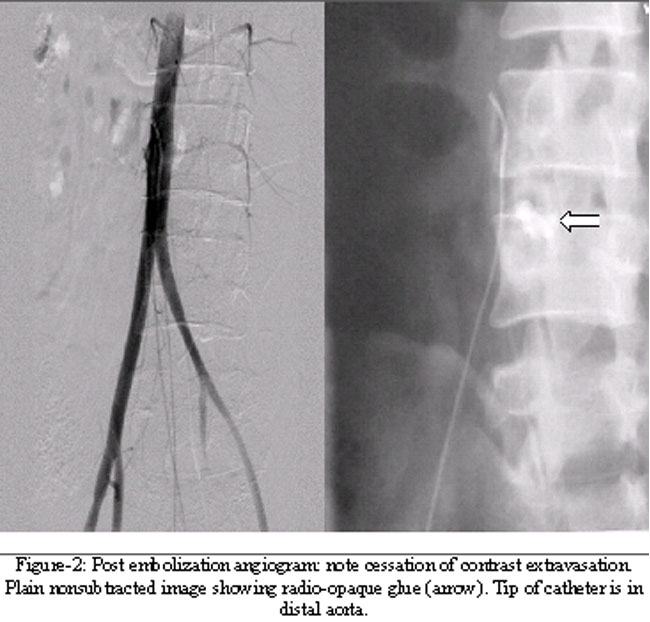
After the procedure, patient was closely monitored and managed in intensive and special care units. His haemodynamic status and clinical condition gradually improved over couple of days. The retroperitoneal haematoma was drained percutaneously by catheter placement. The patient then underwent internal fixation for his femoral fracture and was later discharged from hospital.
Discussion
Continuous retroperitoneal bleeding from the injured pelvic or paraspinal arteries particularly lumbar arteries could be a major source of haemorrhage in patients with pelvic fractures.4 Sheering forces from sudden rotation or violent flexion extension injuries may be the cause of such vascular injuries. Fracture of a transverse process may be responsible for direct laceration and avulsion of a lumbar artery or rarely formation of a pseudo-aneurysm may be the cause.5
Prompt diagnosis and urgent intervention is the cornerstone of haemostasis in haemodynamically unstable patients. Computed tomography is imperative in diagnosis and management. It should be used to determine presence and extent of retroperitoneal haematoma, to localize the pelvic bleeding site and any associated extrapelvic visceral or arterial injury.6
Since mid 1950s angiography is being frequently used as diagnostic modality for evaluation of visceral or vascular trauma. Overall, angiography confirms posttraumatic arterial bleeding in approximately 80-90% of cases.7 After having localized one or several sources of retroperitoneal haemorrhage, haemostasis is achieved by catheter embolization.
The aim of embolization is to achieve immediate vascular occlusion (often temporarily) by decreasing pressure upstream from the leak; this facilitates physiological haemostasis, thrombus formation and healing of the dissected vessels.6 This technique is proving to be the treatment of choice for securing haemostasis. When compared to surgery, it is a relatively simple, safe, prompt and effective method of controlling the haemorrhage.8,9
Various authors have reported high technical success rates for selective transcatheter embolization of lumbar arterial injury.3-5,10 Embolic agents described in literature for lumbar artery embolization include coils and microparticles, gelfoam and rarely glue.3,10 We used glue instead of other embolization material since the artery was avulsed from its origin and no segment was found to place the coil or particles.
Possible complications of the procedure include retroperitoneal infarction and abscess formation. Another important concern in embolizing lumbar arteries is that the arteria radicularis magna (also called the artery of Adamkievicz) should be identified in order to avoid potential embolization, which can result in severe neurological damage.
Conclusion
Our case illustrates the potential value of early imaging particularly arteriography and transcatheter embolization in cases of pelvic and spinal trauma leading to retroperitoneal haemorrhage with particular reference to lumbar arterial injury as the cause.
References
1.Brown JJ, Greene FL, McMillin RD.Vascular injuries associated with pelvic fractures. Am Surg 1984; 50: 150-4.
2.Sclafani SJ, Florence LO, Phillips TF, Scalea TM, Glanz S, Goldstein AS, et al. Lumbar arterial injury: radiologic diagnosis and management. Radiology 1987; 165: 709-14.
3.Sofocleous CT, Hinrichs CR, Hubbi B, Doddakashi S, Bahramipour P, Schubert J. Embolization of isolated lumbar artery injuries in trauma patients. Cardiovasc Intervent Radiol 2005; 28: 730-5.
4.Hori A, Nagata Y, Hanashiro Y, Ohshiro K, Shimabukuro K, Mekaru T, et al. Embolization of the lumbar artery for pelvic fracture. Rinsho Hoshasen 1989; 34: 1047-50.
5.Domenicucci M, Ramieri A, Lenzi J, Fontana E, Martini S. Pseudo-aneurysm of a lumbar artery after flexion-distraction injury of the thoraco-lumbar spine and surgical realignment: rupture treated by endovascular embolization. Spine (Phila Pa 1976) 2008; 33: E81-4.
6.Geeraerts T, Chhor V, Cheisson G, Martin L, Bessoud B, Ozanne A, et al. Clinical review: initial management of blunt pelvic trauma patients with haemodynamic instability. Crit Care 2007; 11: 204.
7.Dondelinger RF, Trotteur G, Ghaye B, Szapiro D. Traumatic injuries: radiological hemostatic intervention at admission. Eur Radiol 2002; 12: 979-93.
8.Gordon RL, Fast A, Aner H, Shifrin E, Siew FP, Floman Y. Control of massive retroperitoneal bleeding associated with pelvic fractures by angiographic embolization. Isr J Med Sci 1983; 19: 185-8.
9.Akpinar E, Peynircioglu B, Turkbey B, Cil BE, Balkanci F. Endovascular management of life-threatening retroperitoneal bleeding. ANZ J Surg 2008; 78: 683-7.
10.Geldof K, Maleux G, Heye S, Van Cleynenbreugel B, Oyen R. Transcatheter embolization of an isolated lumbar arterial bleeding complicating radical nephrectomy for renal infarction with infected perirenal haematoma. JBR-BTR 2008; 91: 203-5.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: