
Muhammad Shakeel ( Department of Otolaryngology Head & Neck Surgery, University of Aberdeen, Aberdeen Royal Infirmary, Aberdeen, Scotland, UK. )
Neil McCluney ( Department of Otolaryngology Head & Neck Surgery, University of Aberdeen, Aberdeen Royal Infirmary, Aberdeen, Scotland, UK. )
Lawrence Li ( Department of Otolaryngology Head & Neck Surgery, University of Aberdeen, Aberdeen Royal Infirmary, Aberdeen, Scotland, UK. )
Jonathan Ray Newton ( Department of Otolaryngology Head & Neck Surgery, University of Aberdeen, Aberdeen Royal Infirmary, Aberdeen, Scotland, UK. )
June 2010, Volume 60, Issue 6
Case Reports
Abstract
Lemierre\'s syndrome is caused by acute oropharyngeal infection with septic secondary thrombophlebitis of the internal jugular vein and metastatic infection. Fusobacterium necrophorum is the most commonly implicated aetiological agent.
The authors present the case of a healthy young man presenting with a history of general malaise and sore throat who developed septic metastatic complications in the left upper limb. He made a complete recovery after treatment with a combination of parenteral antibiotics and a multidisciplinary approach.
Early ultrasound scanning of the neck and blood cultures are advocated to diagnose this potentially fatal condition.
Management involves a high degree of clinical suspicion for this often \'forgotten\' condition and treatment is further discussed in the article.
Introduction
Tonsillopharyngitis is one of the most common conditions seen by general practitioners. This usually settles with simple analgesia and oral antibiotics with penicillin V being the treatment of choice. Suppurative complications of throat infections may include peritonsillar, parapharyngeal and retropharyngeal cellulitis or abscesses.1
An extremely uncommon complication of oropharyngeal infection is internal jugular vein (IJV) thrombosis with metastatic abscesses in other parts of body. This was first described in 1936 by the French microbiologist Dr. Lemierre.2 This condition causes significant morbidity leading to mortality in some cases. The advent of antibiotic therapy has dramatically decreased the incidence of Lemierre\'s disease and it has been referred to as "Forgotten disease."
The number of infections caused by Fusobacterium necrophorum, the most commonly implicated organism, has been rising possibly because of restricted antibiotic prescribing for sore throat in the community.3 There is a need to raise awareness among clinicians about this potentially life threatening clinical entity so that early and appropriate antibiotic therapy can be instituted.
We report the case of a fit and healthy young man who developed soft tissue infection of the left thenar eminence with spreading cellulitis following tonsillopharyngitis.
Case Report
A 43 year old gentleman was admitted to the medical assessment unit of a teaching hospital in the north east of Scotland with a two weeks history of general malaise and flu-like symptoms with aching joints and rigors, and marked odynophagia for 48 hours. Over the previous day, he had developed swelling over his left hand associated with erythema tracking up his forearm. His general practitioner had started oral penicillin V the previous day. No significant past medical history was noted. On examination, the patient had pyrexia of 38.3°C. His cervical lymph nodes were enlarged bilaterally. There was a soft systolic murmur on cardiovascular examination and his abdomen was mildly tender over the right iliac fossa. Respiratory and neurological examination was otherwise unremarkable.
Examination of his left (dominant) arm revealed diffuse swelling over the hand muscles, worse over the thenar eminence with swollen and tender interphalangeal joints. His range of movement was markedly reduced because of swelling and pain. There was evidence of ascending lymphangitis on his forearm (Figure-1).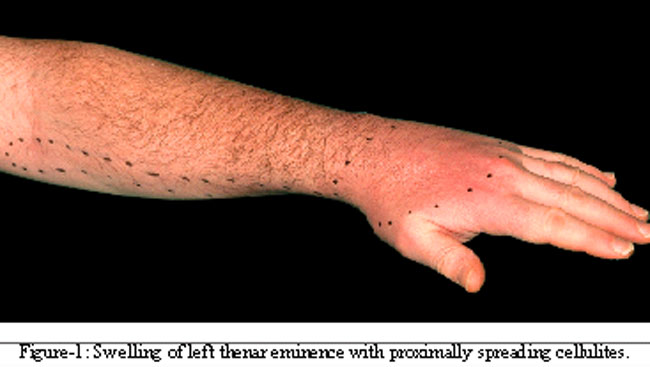
His blood results showed an increased white cells count of 15.5 x 109/L with a neutrophilia of 14.4 x 109/L. C-reactive protein was also raised at 128 mg/L. Blood cultures were taken on admission. The chest x-ray was normal as was the electrocardiogram.
The initial diagnosis was septic arthritis and high dose intravenous (IV) benzyl penicillin and flucloxacillin were commenced. The erythema continued to spread up the patient\'s arm despite antibiotics and his inflammatory markers remained elevated. He was seen by the Rheumatology team and a diagnosis of soft tissue infection was made. Continuation of the same IV antibiotics regime was advised.
The patient was reviewed by an orthopaedic surgeon, who advised that the arm be elevated in a Bradford sling along with increasing the dose of antibiotics. A diagnosis of web space infection with proximally spreading cellulitis was made. Formal incision and drainage was thought unnecessary at that time and a subsequent ultrasound scan of his hand failed to show any evidence of pus collection (Figure-2).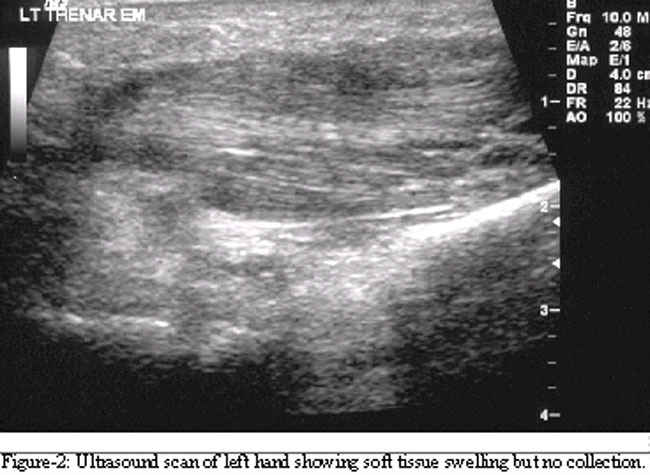
Given the history of severe sore throat, the patient was also reviewed by an otolaryngologist. Examination of his throat revealed generalised oropharyngitis with tender cervical lymphadenopathy. At this stage, the suspicion of Lemierre\'s syndrome was raised. Intravenous metronidazole was added to the patient\'s treatment regimen. An ultrasound scan of the neck was performed but did not show any evidence of internal jugular vein thrombosis (Figure-3),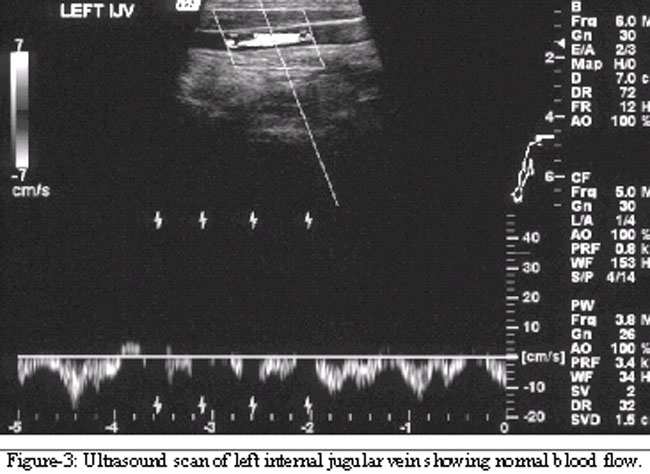
and there was good blood flow in the internal jugular, subclavian, brachiocephalic and axillary veins. The blood cultures failed to grow any organisms. A subsequent echocardiogram was normal.
His symptoms improved gradually and the patient was eventually discharged home 8 days after admission on oral antibiotics.
Discussion
In the original description of this syndrome, Lemierre described oropharyngeal infection resulting in internal jugular vein thrombophlebitis, bacteraemia and septic embolization.2 More recently stricter criteria4 have been used to diagnose Lemierre\'s syndrome:
1-Primary infection in the oropharynx, 2- Septicaemia documented by at least one positive blood culture, 3- Clinical or radiographic evidence of internal jugular vein thrombophlebitis, 4- At least one metastatic focus.
The anaerobic bacteria Fusobacterium necrophorum is a commensal in the oropharynx and is the most commonly implicated organism in Lemierre\'s syndrome.4 Other members of the genus fusobacterium (F. nucleatum, F. mortiferum and F. varium) have been implicated less commonly, as have bacteroides and anaerobic streptococcus species.4
The disease usually begins with an acute oropharyngeal infection but Lemierre noted that the syndrome could also occur as a complication of otitis media, mastoiditis, or even dental infection.2 Bacteria from the original source penetrate the adjacent internal jugular vein and cause an infected thrombosis. Septic emboli most commonly occur in the lungs. However, almost any system in the body can be involved. This can include joint inflammation, soft tissue abscess formation, renal complications, and central nervous system involvement in the form of meningitis, cerebral infarcts and cerebral abscess formation.3
Lemierre\'s syndrome most commonly occurs in young, healthy adults but other age groups can also be affected.4
The diagnosis of Lemierre\'s syndrome can be made only if the clinician is aware of the condition.3 A diagnosis can be made solely on clinical grounds.2 Throat swab is usually negative in patients with Lemierre\'s syndrome.3 Confirmation of Lemierre\'s syndrome is provided by positive blood culture for Fusobacterium necrophorum, and patients with blood cultures growing F. necrophorum should be assumed to have Lemierre\'s syndrome until proven otherwise.3 It is important to note that, if the classical features of Lemierre\'s syndrome are present, negative cultures do not rule out the diagnosis.3
If the condition is suspected, an ultrasound (US) scan of the neck and internal jugular veins is recommended as the first line radiological investigation. It is easily available, sensitive, inexpensive and does not involve radiation exposure. It can confirm internal jugular vein thrombosis and show localized echogenic regions within a dilated vessel.5 Its limitations are that it can miss a fresh thrombus with low echogenicity,5 and it is known to provide poor imaging beneath the clavicle and mandible.6 In addition, the findings may be influenced by the skill of the ultrasonographer.6
CT scanning is considered a better option by some practitioners because of its increased sensitivity than US scanning, but it involves radiation exposure, intravenous contrast administration and is more expensive. A positive scan shows a dilated internal jugular vein with low attenuation of the intraluminal contents and enhancement of the vessel wall and surrounding tissue.3
MRI scanning provides excellent soft tissue delineation, multiplanar views and has an accuracy of 97% compared with contrast venography (the gold standard) and involves no radiation exposure.7
Fusobacterium necrophorum is highly sensitive to beta-lactam antibiotics, clindamycin and metronidazole but treatment failures with penicillin have been documented.5 The addition of metronidazole is therefore recommended for broad spectrum coverage.8 The duration of antimicrobial treatment remains controversial but most regimes last for of 3-6 weeks.4
Surgical ligation of the internal jugular vein is usually reserved for patients with persistent septic embolization despite maximal appropriate antibiotic therapy.4 Anticoagulation with heparin is recommended by some authors,9 whilst others would limit this to patients with evidence of retrograde progression to the cavernous sinus and brain.10
Conclusion
The authors have presented a case that clinically resembles Lemierre\'s syndrome. Although there was no organism isolated in blood cultures, this may be explained by the initiation of high dose oral antibiotics in the community. The ultrasound scan also failed to show any evidence of thrombophlebitis of the neck veins but the soft tissue infection of the arm is clearly suggestive of metastatic infection.
Lemierre\'s syndrome is extremely uncommon and the authors feel this report is educational for physicians unfamiliar with this clinical entity. A high index of suspicion is required to diagnose this potentially life-threatening condition.
Acknowledgement
We are grateful to Mr. Clive Brewis, consultant otolaryngologist, for allowing us to report this case.
References
1.Tewfik TL, Al Garni M. Tonsillopharyngitis: clinical highlights. J Otolaryngol 2005; 34: S45-9.
2.Lemierre A. On certain septicaemias due to anaerobic organisms. Lancet 1936; 1: 701-3.
3.Syed MI, Baring D, Addidle M, Murray C, Adams C. Lemierre syndrome: Two cases and a review. Laryngoscope 2007; 117: 1605-10.
4.Sinave CP, Hardy GJ, Fardy PW. The Lemierre syndrome: suppurative thrombophlebitis of the internal jugular vein secondary to oropharyngeal infection. Medicine (Baltimore) 1989; 68: 85-94.
5.Golpe R, Marin B, Alonso M. Lemierre\'s syndrome (necrobacillosis). Postgrad Med J 1999; 75: 141-4.
6.Shah SA, Ghani R. Lemierre\'s syndrome: a forgotten complication of oropharyngeal infection. J Ayub Med Coll Abottabad 2005; 17: 30-3.
7.Nakamura S, Sadoshima S, Doi Y, Yoshioka M, Yamashita S, Gotoh H, et al. Internal jugular vein thrombosis, Lemierre\'s syndrome; oropharyngeal infection with antibiotic and anticoagulation therapy - a case report. Angiology 2000; 51: 173-7.
8.Leugers CM, Clover R. Lemierre syndrome: postanginal sepsis. J Am Board Fam Prac 1995; 8: 384-91.
9.Moore BA, Dekle C, Werkhaven J. Bilateral Lemierre\'s syndrome: a case report and literature review. Ear Nose Throat J 2002; 81: 234-6.
10.Finegold SM, Bartlett JG, Chow AW, Flora DJ, Gorbach SL, Harder EJ, Tally FP. Management of anaerobic infections. Ann Intern Med 1975; 83: 375-89.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: