
Meharunnisa Khaskheli ( Department of Gynaecology & Obstetrics, Unit - IV, Liaquat University of Medical & Health Sciences, Jamshoro, Sindh. )
Shahla Baloch ( Department of Gynaecology & Obstetrics, Unit - IV, Liaquat University of Medical & Health Sciences, Jamshoro, Sindh. )
June 2010, Volume 60, Issue 6
Original Article
Abstract
Objective: To investigate women\'s own labour pain perception, experiences and satisfaction with health care providers at a referral hospital of Sindh.
Methods: A descriptive study conducted on 400 labouring women at Obstetrics and Gynaecology Department Unit-II and IV Liaquat University Hospital Hyderabad / Jamshoro from January 2006 to July 2006.
Four hundred full term labouring women in first stage of labour were included in the study. All the women with associated medical problems were excluded. Two questionnaires were completed containing demographic details, antenatal record, mode of onset of labour, labour duration, ambulation, use of various pharmacological agents and women\'s personal experiences regarding pain perception and future family planning. Data was collected and analyzed on simple percentage basis.
Results: This study shows an acceptable birth experience in 136 (34%) cases, while 264 (66%) patients found it an exhausting painful experience. Common factors which favour good experience included lower socioeconomic class 67 (57.98%), rural population (54.68%), multiparous women (68.08%), prior knowledge of labour pains (69.31%), spontaneous labour (86.89%), use of pharmacological agents (76.04%) and co-operative staff attitude (89.27%). Those who found labour pains an acceptable process, 87.5% had a positive attitude for future child bearing.
Conclusion: Childbirth can be a good experience with effective antenatal counseling. A highly professional attitude and tender loving care is the key to a pain free labour (JPMA 60:473; 2010).
Introduction
Perception of pain, including pain of uterine contraction, is a complex process that involves interaction of both central and peripheral mechanisms and continuous interchange of information among nociceptive and descending anti nociceptive pathways. Pain perception involves sensory, emotional, behavioural and environmental factors. Most women rate pain of childbirth as the most painful experience of their lives.1
Labour pain is nearly a universal experience for childbearing women but threshold of this pain varies between individuals. It may be different from other types of pain as there is an achievement of end product i.e. of having a baby. It can have deleterious effects on the mother, on the foetus and on labour outcome itself. Despite wide spread availability of pain intervention in childbirth, for most women childbirth is associated with Labour pain that exceeds expectation.2 The control of labour pain and prevention of suffering are major concerns of clinicians and their clients.3
To date accurate and objective measures of labour pains continue to be scarce.4 Furthermore the discrepancy in labour pain perception between parturient and health care providers remains challenging.5
The pain perception in child birth and satisfaction depends on various pre delivery and intrapartum factors. Pre delivery factors include social status, parity, prenatal education, counseling, while intrapartum factors influencing satisfaction are mode of delivery, duration of labour, medical intervention and personal support. Most of the studies done in this regard are from developed countries. The rationale of this study was to find out various factors influencing labour pain perceptions and satisfaction in our setup.
Subjects and Methods
This study was conducted at two units of gynaecology and obstetric department of Liaquat University of Medical and Health Sciences, Jamshoro from January 2006 To July 2006. During this study period four hundred full term, pregnant women in first stage of labour were included. All those women who were having associated medical problem or high-risk pregnancies and second stage of labour were excluded. In this study all primiparous women who had first delivery and multiparous women who had more then one delivery were included. The management of labour and its monitoring was according to the labour room protocol. The pharmacological agents used for the management of pain were spasmolytic agents, narcotic analgesics during 1st stage of labour and local anaesthetic agents were used during 2nd stage of labour when episiotomy was needed. Two pre-designed proformas were filled with their consent and proper counseling. First proforma was filled by the resident staff on duty containing demographic details, antenatal record, mode of onset of labour, labour duration, use of pharmacological agents, like injectable narcotic analgesic, spasmolytics and local anaesthetic agents including their effect. The second proforma was filled on 1st postnatal day. This proforma contained information of women\'s own experiences regarding labour pains, effects with different treatment modalities, out come, staff attitude and future obstetrical planning. The data was collected, and analyzed regarding birth experience as good and bad and the factors influencing the experience. Analysis was performed through SPSS version 10.0.
Results
Out of 400 women, birth experience was acceptable in 136 (34%) cases and it was unacceptable in 264 (66%) cases (Table-1).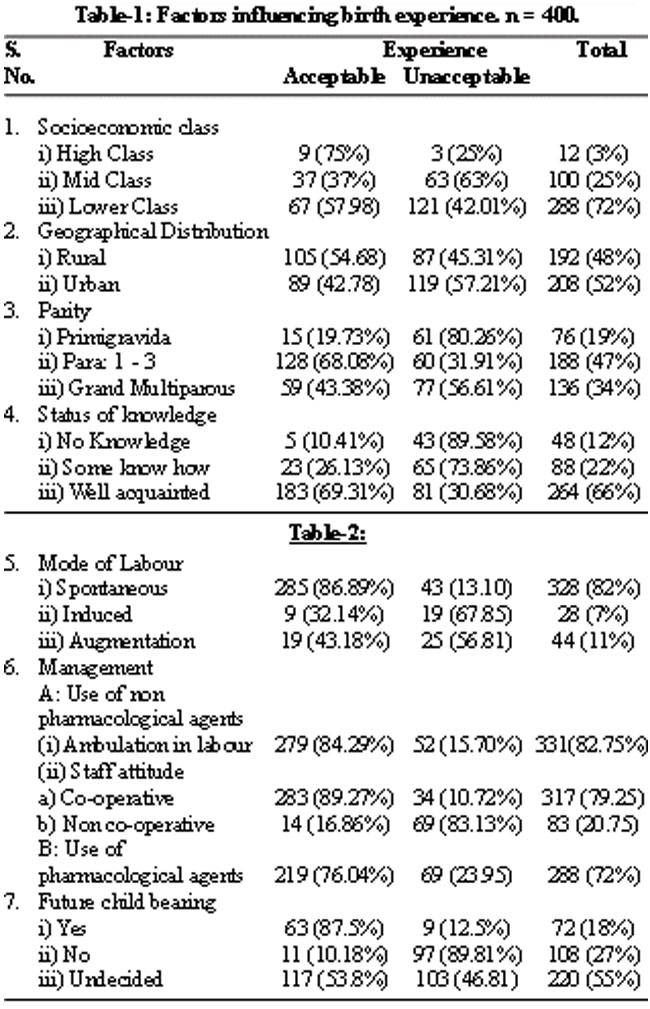
The factors influencing birth experience as acceptable were lower socio economic class in 67 (57.98%) cases, rural population in 105 (54.68%) cases, multiparous women (Para 2-3) in 128 (68.08%) cases, prior knowledge of labour pains in 183 (69.31%) cases, spontaneous onset of labour in 285 (86.89%) cases, ambulation during labour 279 (84.29%), use of pharmacological agents in 219 (76.04%) cases, co-operative staff attitude in 283 (89.27%) cases and future child bearing with yes response in 63 (87.5%) cases, while unacceptable response was seen in middle class in 63 (63%) cases, urban population in 119 (57.21%) cases, primigravidas in 61 (80.26%) cases, no prior knowledge of labour pain in 43 (89.58%) cases, labour induction in 19 (67.58%) cases, non cooperative staff attitude in 69 (83.13%) cases. Future child bearing with no response was reported in 97 (89.81) cases (Table-2).
Discussion
The concept of satisfaction with obstetric care is interpreted as a positive or a negative attitude or evaluation of the event.6 Most of the studies suggest pain as a contributing factor in reducing satisfaction.7 This study analyzed different factors influencing women\'s delivery experiences at referral hospital in our set up. Our study shows that antenatal knowledge of birth experience either self acquired due to the previous deliveries or antenatal counseling shows acceptable response in majority of the cases 183 (69.3%). This is consistent with another study where birth experience is viewed as positive particularly when women are provided with information8 and are able to feel in control during the process. The study by Amanda Henry et al9 showed that vast majority of women had antenatal information regarding intrapartum pain management from varied and multiple sources and most of the women had both positive and negative pain experience.
Our study revealed that birth experience was acceptable in spontaneous labour 285 (86.89%) and unacceptable in induced labour 19 (67.85%). Comparing with Seguin L et al.10 It was noted that intrapartum factors influencing satisfaction, include duration of labour and mode of labour. This could be due to the fact that spontaneous labour is smooth and less time consuming.
This study showed that staff attitude has a great influence on pain perception. With co-operative staff attitude birth experience was good in 283 (89.27%) cases, compared with the study of Abushaika L et al11 which showed that emotional support, holding the patients hands and being physically close to them made a difference during labour. The nurses interpersonal skills are perceived as more important than technical skills. Other studies have observed that pre delivery factors in child birth satisfaction include social status,7 prenatal expectations,12 prenatal education, class attendance and parity. Women need physical as well as psychological support during labour. They should be provided comfort through massage, healing touch, deep breathing exercises, and prayers so as to determine their mental satisfaction and have a positive outcome.
In the current study, majority 331 (82.75%) women had ambulation during labour and out of them 279 (84.29%) experienced acceptable response. Ambulation in labour is commonly believed to be of value in the establishment and progression of labour.13 The advantages of the ambulation in the upright position during labour include enhancement of the pelvic diameter, increased coordination, frequency and intensity of uterine contraction, increased maternal comfort and satisfaction and improved neonatal outcome, decreased perception of labour pain, decreased need for labour augmentation and decreased requirements for labour analgesia.14-16
This study noted that inspite of the use of pharmacological agents (non epidural) either injectable analgesics or local anaesthetic agents, 69 (23.95%) patients were dissatisfied with the pain relief which is consistent with other studies.17 Although, different narcotic analgesics are used for women in labour at different institutions, however, these are associated with a high frequency of adverse events.18 Another method of pain relief is epidural analgesia. Many studies have reported that epidural analgesia clearly provides effective pain relief for labour, but not all women will wish for epidural analgesia as their first choice of pain relief in labour.19,20 Furthermore with epidural Analgesia there are increased chances of prolonged labour, instrumental delivery and different complications.21,23 In our setup the facility of epidural analgesia is not available, which is an effective method of pain relief in labour.
The result of our study observed that out of 400 women, birth experience was unacceptable in majority 264 (66%) cases. This is because of unplanned pregnancy with less birth spacing, lack of education, none or little knowledge during antenatal period, decision making, mode of labour, staff attitude, ineffective analgesics and lack of epidural. Similar findings are reported by Henry A et al,24 that birth experience will be acceptable with overall management of all the above mentioned factors.
The support of health care personnel in labour, provision of information and maternal involvement in decision making are clearly central in achieving a positive child birth experience.
The current study has limitations as it is of a moderate size from a single institution and lacked other methods of pain relief like epidural and nitrous oxide. Further work is required to provide cross sectional data from a variety of institutions across the country to improve the result.
Conclusion
Childbirth is a pleasant experience for those well counseled, having spontaneous delivery with tender loving care in a hospital. It can be a nightmare for those who did not have any prior knowledge, had interventions and augmentation in labour and were not attended by the sympathetic medical personnel or those who did not have any medical analgesics.
References
1.Cheek TG, Gutsche BB, Gaiser RR, Chestnut DH. Obstetric anesthesia. Principles and Practice. 2nd ed. St Louis: Mosby 1999; 320-35.
2.Atherton MJ, Feeg VD, el-Adham AF. Race, ethinicity and insurance as determinant of epidural use: analysis of a national sample survey. Nurs Econ 2004; 22: 6-13.
3.Green JM, Baston HA. Feeling in control during labor: concepts, correlates, and consequences. Birth 2003; 30: 235-47.
4.Baker A, Ferguson SA, Roach GD, Dawson D. Perceptions of labour pain by mothers and their attending midwives. J Advanced Nursing 2000; 35: 171-9.
5.Mc Crea BH, Wright ME. Satisfaction in Labour and perceptions of personal control in pain relief during labour. J Advanced Nursing 1999; 29: 877-84.
6.Hodnett ED. Pain and women\'s satisfaction with the experience of childbirth: a systematic review. Am J Obstet Gynaeocl 2002; 186: 160-72.
7.Slade P, Mac Pherson SA, Hume A, Maresh M. Expectations, experiences and satisfaction with labour. Br J Clin Pychol 1993; 32: 469-83.
8.Waldenstrom U, Borgi IM, Olsson B, Skold M, Wall S. The Childbirth experience: a study 295 new mothers. Birth 1996; 23: 144-53.
9.Henry A, Nand SL. Women\'s antenatal knowledge and plans regarding intrapartum pain management at the Royal Hospital for Women. ANZJOG 2004; 44: 314-7.
10.Seguin L, Therrien R, Champagne F, Larouche D. The components of women\'s satisfaction with maternity care. Birth 1989; 16: 109-13.
11.Abushaikha L, Oweis A. Labour pain experience and intensity: A Jordanian perspective. Int J Nursing Practice 2005; 11: 33-8.
12.Green JM, Coupland VA, Kitzinger JV. Expectations, experiences and psychological outcomes of childbirth: a prospective study of 825 women. Birth 1990; 17: 15-24.
13.Vallejo MC, Firestone LL, Mandell Gl, Jaime F, Makishima S, Ramanathan S. Effects of epidural analgesia with ambulation on labour duration. Anaesthesiology 2001; 95: 857-61.
14.Albers LL, Anderson D, Cragin L, Daniels SM, Hunter C, Sedler KD, et al. The relationship of ambulation in labour to operative delivery. J Nurse Midwifery 1997; 42: 4-8.
15.Nageotte MP, Larson D, Rumney PJ, Sidhu M, Hollenbach K. Epidural analgesia compared with combined spinal - epidural analgesia during labour in nuliparous women. N Engl J Med 1997; 337: 1715-9.
16.Cefalo RC, Bowes WA Jr, Managing labour - never walk alone. N Engl J Med 1998; 339: 117-8.
17.Long J, Yue Y. Patient controlled intravenous analgesic with tramadol for labour pain relief. Chin Med J (Engl) 2003; 116: 1752-5.
18.Hussain SM. Nalbuperine for relief of Labor Pain in Primiparous Women. Mother & Child 1997; 35: 62-6.
19.Howel CJ Epidural versus non epidural analgesia for pain relief in labor (Cochrane review). In: The Cochrane library, issue 4, 2000. Oxford: update Software.
20.Khor LJ, Jeskins G Cooper GM, Paterson - Brown S. National obstetric anaesthetic practice in the UK 1997/1998. Anesthesia 2000; 55: 1168-72.
21.Naz F, Saeed M. Epidural Analgesia and Labour Mechanisms. Mother & Child 1998; 13: 132-5.
22.Tabassum H, Shahzad S, Sheraz S, Boota M. Epidural analgesia in labour; maternal and fetal outcome. Professional Med J 2008; 15: 9-12.
23.Siddiqi KJ, Atiq F, Ambreen A, Khan FM. Complications and outcome with epidurals for labour: Analysis of seven years experience. Ann King Edward Med Coll 2007; 13: 24-6.
24.Henry A, Nand SL. Intrapartum Pain management at the Royal Hospital for Women. Aust NZJ Obstet Gynaecol 2004; 44: 307-13.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: