
Faisal Qadir ( Department of Cardiology, Tabba Heart Institute,Karachi, Pakistan. )
Salman Farooq ( Medical Student, Ziauddin Medical University, Karachi, Pakistan. )
Moinuddin Khan ( Department of Cardiology, Tabba Heart Institute,Karachi, Pakistan. )
Bashir Hanif ( Department of Cardiology, Tabba Heart Institute, Karachi. )
Muhammad Shakir Lakhani ( Department of Cardiology, Tabba Heart Institute,Karachi, Pakistan. )
June 2010, Volume 60, Issue 6
Original Article
Abstract
Objective: To determine the correlation of cardiac troponin I (cTnI) 10 folds upper limit of normal (ULN) and extent of coronary artery disease (CAD) in Non-ST-elevation myocardial infarction (NSTEMI).
Methods: A cross-sectional study was conducted on 230 consecutive NSTEMI patients admitted in Tabba Heart Institute, Karachi between April to December 2008. cTnI was measured using MEIA method. All patients underwent coronary angiography in the index hospitalization. Stenosis > 70% in any of the three major epicardial vessels was considered significant CAD. Extent of CAD was defined as significant single, two or three vessel CAD. Chi-square test was applied to test the association between cTnI levels and CAD extent.
Results: Out of 230 patients, in 111 patients with cTnI levels < 10 folds upper limit of normal (ULN), 25 (22.52%) had single vessel, 40(36%) had two vessel and 34(30.6%) had three vessel significant CAD, whereas in 119 patients with cTnI levels > 10 folds ULN, 23(19.3%) had single vessel, 37(31.1 %) had two vessel and 55(46.2%) had three vessel significant CAD. The results suggest that there was an insignificant association between the cTnI levels and single vessel, two vessel and the overall CAD extent (p= 0.35, p= 0.21 and p= 0.13 respectively), however there was a statistically significant association between the cTnI levels and three vessel CAD (p < 0.04).
Conclusion: Higher cTnI levels are associated with an increased proportion of severe three vessel CAD involvement. Prompt identification and referral of this patient subset to early revascularization strategies would improve clinical outcomes (JPMA 60:423; 2010).
Introduction
Among patients presenting with acute coronary syndrome (ACS), multiple segments of the coronary arterial tree exhibit plaque disruption or frank rupture, which is possibly related to a pan-inflammatory process,1 hence it is uncommon to see non-obstructive coronary artery disease (CAD) or a normal coronary angiogram in patients undergoing coronary angiography for ACS.2 As the number of hospital admissions with acute coronary syndromes is increasing, there has been a concomitant increase in the incidence of multi-vessel CAD in the setting of non-ST-elevation myocardial infarction (NSTEMI). Recently, American College of Cardiology National Cardiovascular Database Registry reported that 42% of NSTEMI patients had multi-vessel CAD.3
The testing for cardiac troponins in the clinical setting of acute coronary syndromes is considered a class I indication for early risk stratification as per American College of Cardiology/American Heart Association (ACC/AHA) guidelines, as it improves clinical outcomes in these patients.4 Guideline updates of ACC/AHA and Spanish Society of Cardiology for the management of patients with NSTEMI have established that the magnitude of troponin elevation is a determining factor in prognosis, such that patients with markedly elevated troponin levels ( > 10 times the upper normal limit) should be stratified initially as high-risk patients.4,5
Both short and long term prognoses in patients with ACS are related to the magnitude of cardiac biomarker release.6 A group of patients with acute coronary syndromes have \'minor\' or borderline troponin elevation.7 It has been demonstrated that this subset of patients have extensive CAD and that they derive prognostic benefit from aggressive medical therapy as well as an early invasive strategy compared to patients with undetectable troponins.8,9
Fernandez and colleagues studied NSTEMI patients who underwent coronary angiography and stratified their study population into two groups based on the cardiac troponin I levels. They found patients with higher troponin I levels ( > 10 folds ULN) had more three vessel CAD involvement (39%), p = 0.001 on coronary angiography as compared to patients with troponin I levels <10 folds ULN.10 It is essential to further elucidate whether the degree of increase in troponin levels in the setting of NSTEMI equates with a greater proportion of such patients found to have severe multi-vessel CAD or significant left main coronary artery stenosis on coronary angiography? This finding will have important therapeutic and prognostic implications as early identification of severe and extensive CAD and subsequent referral to early coronary revascularization would result in clinical benefit. This would also help minimize the risk of major adverse cardiac events in the risky waiting period of initial medical therapy alone. To test this hypothesis, we sought to determine whether there is an association between cardiac troponin I levels and the extent of CAD in NSTEMI.
Patients and Methods
We conducted a prospective, cross sectional study of 230 consecutive patients admitted to coronary care unit of Tabba Heart Institute, Karachi between April 2008 and December 2008 with the diagnosis of non-ST-elevation myocardial infarction. Patients included had history of chest discomfort within the past 48 hours of presentation or angina equivalent symptoms and a positive cardiac troponin I test, defined as a level above the upper limit of normal (0.4 ng/ml) on admission. The exclusion criteria included ST-segment elevation on electrocardiography (ECG) indicative of acute ST elevation myocardial infarction, pathologic Q waves, new or presumed new left bundle branch block or paced rhythm, previous history of coronary artery disease, prior coronary revascularization procedures either CABG or angioplasty or coronary stenting, renal insufficiency - serum creatinine > 1.4 mg/dL (upper limit of normal), serious intercurrent disease and patients who refused to undergo coronary angiography during the hospitalization. Written informed consent was obtained in all cases for recruitment in the study and the procedures. Study protocol was approved by the ethical review committee.
NSTEMI was defined as positive biomarkers of myocardial necrosis (troponin-I) with or without electrocardiographic ST-segment depression (> 0.5 mm) or prominent T wave inversion in the absence of ST-segment elevation. All patients received standard medical therapy for NSTEMI. Blood samples for cardiac troponin I were immediately drawn in lithium heparin bottles upon presentation to the emergency room and a second sample was drawn 8 hours later after admission. Cardiac troponin I was determined using AxSYM Troponin-I ADV (Abbott Laboratories, Abbott Park, Illinois) which is a three-step assay, based on the micro-particle enzyme immunoassay (MEIA) technology with an analytical sensitivity of 0.02 ng/ml and a diagnostic cutoff for myocardial infarction of 0.40 ng/ml. The 99th percentile was 0.04 ng/ml as described by the manufacturer. The assay was designed to have a precision < 10% total coefficient of variation with 95% confidence for concentration from 0.27 ng/ml upto 4.00 ng/ml. All assays were done by technologists unaware of the clinical and angiographic data.
All recruited patients underwent invasive evaluation by coronary angiography within 72 hours of the same hospital admission. Diagnostic coronary angiography was performed via either the trans-femoral or trans-radial approach using standard techniques. Cine angiographic films were analyzed independently by two experienced operators who had no knowledge of the patients\' clinical information and cTnI status. Differences were mediated by consensus. The lesions were assessed in two orthogonal views that had the least vessel overlap and foreshortening. End-diastolic frames assessment was used and the projection revealing the smallest lumen diameter was selected for stenosis assessment. The mean of three measurements of minimal lumen diameter and angiographically normal reference diameters proximal and distal to the lesion were used to calculate the percent diameter stenosis.
Significant CAD was defined as > 70% stenosis in any of the three major epicardial coronary arteries or a left main coronary artery stenosis > 50%. Branch vessel CAD was defined as > 70% stenosis in a major side branch of an epicardial artery (if > 2 mm in diameter). Angiograms revealing coronary artery stenosis < 70% in major epicardial coronary arteries were termed as non-obstructive CAD. Extent of CAD was defined as significant single, two or three vessel CAD involvement.
A proforma was designed to record patient demographics including cardiac risk factors, ischaemic ECG changes, values of cardiac troponin I levels and the different coronary artery segments for stenosis documentation.
Statistical Analysis:
The collected data was entered and analyzed by the Statistical Package for Social Sciences version 15.0 Software (SPSS Inc., Chicago, Illinois).
Continuous variables such as age and troponin I levels were expressed as mean ± SD and categorical variables including diabetes, hypertension, dyslipidemia, cigarette smoking, positive family history of CAD, ECG ischaemic abnormality, extent of CAD , significant left main artery stenosis and number of occluded vessels were presented as frequencies and percentages.
Chi-square test was used to evaluate the relation between cardiac troponin I levels and CAD extent in the two cutoff levels of cardiac troponin I. All significance tests were 2 sided, and the results were considered statistically significant when p value > 0.05.
Results
A total of 230 patients were included in the study. There were 169 (73.4 %) males and 61 (26.5 %) females, age range 30-86 years, mean 59.35 ± 11.08 years and cTnI levels ranged between 0.41-88 ng/mL, mean 10.31 ± 15.91 ng/ml. 115 (50 %) patients had diabetes, 160 (69.5 %) had hypertension and 147 (63.9 %) had dyslipidaemia. There were 64 (27.8 %) smokers and 51(22.2 %) patients had positive family history of premature CAD. cTnI was > 10 folds ULN in 111 (48.2 %) patients and >10 folds ULN in 119 (51.7 %) patients. Cardiac troponins I levels ranged from 0.43 - 3.94 ng/ml, with mean 1.67 ± 1.06 ng/ml in the cTnI < 10 folds ULN group and ranged from 4.09 - 88 ng/ml, with mean 18.38 ± 18.83 ng/ml in the cTnI > 10 folds ULN group.
The frequencies of the variables including cardiac risk factors and ischaemic ECG changes are shown in Table-1.
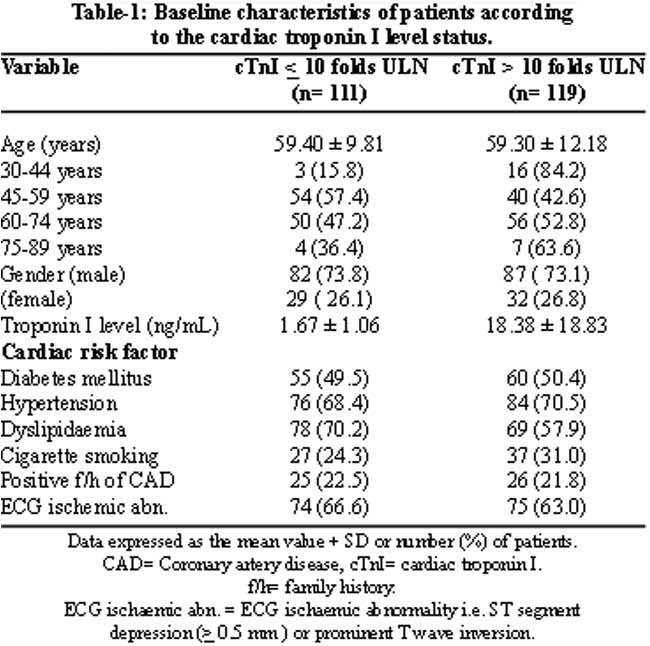
Patients with troponin I level < 10 folds ULN tend to be more dyslipidaemic 78 (70.2 %) versus 69 (57.9 %), while patients with troponin I level > 10 folds ULN had a higher incidence of cigarette smoking 37 (31.1 %) versus 27 (24.3 %), a higher proportion of younger patients (age less than 45 years), 16 (84.2 %) versus 3 (15.8 %) and also of older patients (age greater than 75 years), 7 (63.6 %) versus 4 (36.4 %). The two groups were otherwise similar.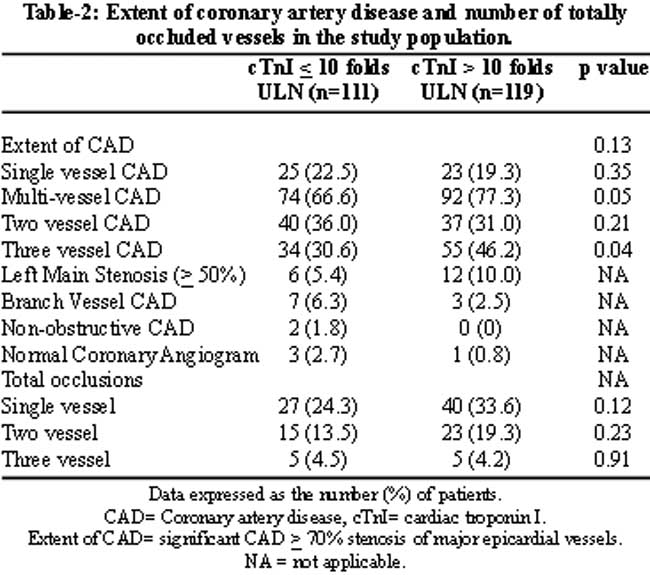
Table-2 compares the extent of CAD and the number of occluded vessels among the two cutoff levels of cardiac troponin I. At coronary angiography, among the 111 patients with cTnI levels < 10 folds ULN, the rates of significant (> 70% stenosis) single, two and three vessel CAD were 25 (22.5 %), 40 (36 %) and 34 (30.6 %) respectively. While among the 119 patients with cTnI levels >10 folds ULN, the rates of significant single, two and three vessel CAD were 23 (19.3 %), 37 (31.1 %) and 55 (46.2 %) respectively, (p= 0.35, p= 0.21 and p <0.04 respectively). When association of the two cutoff levels of cTnI with the overall extent of CAD was considered, this was not statistically significant (p= 0.13). Furthermore, in patients with cTnI > 10 folds ULN, there were also a greater proportion of patients with left main coronary artery stenosis (> 50% stenosis) and a greater number of totally occluded vessels.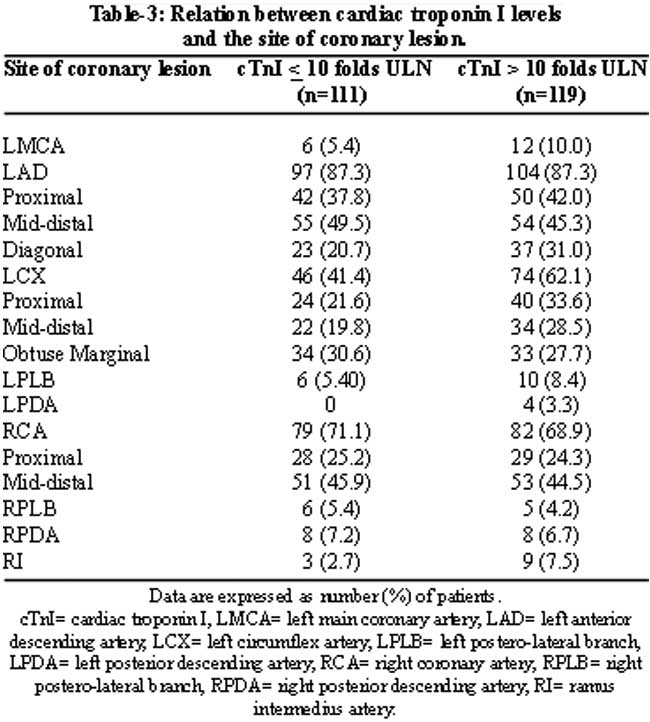
Table-3 summarizes the angiographic characteristics of patients in the two cutoff levels of cTnI with respect to the site of significance (> 70%) coronary stenosis. The left anterior descending artery (LAD) was the vessel most commonly involved with significant stenosis in both the groups. In patients with cTnI levels < 10 folds ULN, LAD was the commonest vessel 97 (87.3%), followed by right coronary artery (RCA) 79 (71.1%) and then left circumflex artery (LCX), 46 (41.4%). While in patients with cTnI levels >10 folds ULN, LAD was the commonest vessel, 104 (87.3%), followed by RCA 82 (68.9%) and then LCX artery 74 (62.1%). In patients with cTnI levels > 10 folds ULN, there was also more involvement of the diagonal branch, left posterior descending artery and left posterolateral branches.
Discussion
The present study provides insight into the association between the two cutoff levels of cardiac troponin I (< 10 folds ULN and >10 folds ULN) in NSTEMI and the number of major epicardial coronary vessels that have significant luminal narrowing (> 70 % stenosis). The study demonstrated that among patients with cTnI levels < 10 folds ULN, 22.5 % of the patients had single vessel, 36 % had two vessel and 30.6 % had three vessel significant for CAD, while among patients with cTnI levels > 10 folds ULN, 19.3 % of the patients had single vessel, 31.1 % had two vessel and 46.2 % had three vessel significant CAD. We found a statistically significant relationship only between cTnI level > 10 folds ULN and severely affected three vessel CAD.
The burden of NSTEMI is increasing globally as compared to ST-elevation MI.11 In acute coronary syndromes, it has been shown that plaque disruption or frank rupture occurs at multiple segments of the coronary artery tree, presumably related to a heightened thrombotic and inflammatory state.12 Despite the presence of studies which have evaluated the association of troponins to angiographic findings of culprit lesion morphology in the setting of ACS, studies evaluating angiographic correlations in terms of the number of significantly narrowed coronary arteries and the exact incidence of multivessel CAD with different cardiac troponin levels have been extremely limited in international literature and there is no local data for such an association. Cardiac specific troponins show small elevations above the ULN in small infarctions, eg. in NSTEMI compared with large infarctions characteristic of STEMI in which troponin levels can be more than 20-50 times ULN.4 Studies on plasma brain natriuretic peptide (BNP), another cardiac biomarker in ACS, have demonstrated a progressive increase in BNP levels in relation to the extent of coronary atherosclerosis. Palazzuoli and colleagues studied the relation of plasma BNP levels in NSTEMI and their association with the number of involved coronary vessels. They excluded patients with heart failure and ejection fraction <50%. Analysis of BNP levels in relation to the number of involved vessels showed significantly higher BNP levels in patients with three vessel than in those with single or two vessel coronary artery disease. There was also more left anterior descending artery involvement with higher levels.13 Whether such a relationship exists for different cardiac troponins I levels in NSTEMI needs to be fully explored.
Absence of CAD is an uncommon finding in patients undergoing coronary angiography for ACS.2 Our study revealed that 3 (2.7 %) patients with cTnI < 10 folds ULN and only 1 (0.84%) patient in the cTnI > 10 folds ULN group had a perfectly normal coronary angiogram. There were more females with normal coronary angiograms in the lower troponin I level group. The TACTICS-TIMI-18 sub study involving 895 patients revealed that in patients who present with symptoms of ACS and have no critical epicardial CAD angiographically, the presence of an elevated troponin was still associated with an adverse prognosis.14 The use of angiography provides an invasive approach to risk stratification. In patients with NSTEMI, angiographic data suggest that there are more acute and more complex plaques, more extensive or multivessel disease, more thrombi and reduced Thrombolysis in Myocardial Infarction (TIMI) flow grades when troponin levels are elevated.15,16 Fernandez et al10 studied 219 consecutive patients admitted with NSTEMI who underwent coronary angiography. Patients were divided into two groups based on a cut-off level of cardiac troponin I of 10 folds ULN. They analyzed clinical and angiographic variables and found patients with troponin I levels (< 10 folds ULN), frequently had higher Braunwald Class angina,17 more severe ECG changes, higher proportion of three vessel CAD (39%) involvement on coronary angiography and greater severity of the culprit lesion. However, only 41 (19%) patients constituted the higher troponin I level group and the majority 178 (81%) patients had lower troponin values. In contrast, the distribution of patients to both the troponin- I cutoff levels was almost equal in our present study.
The prognosis in patients with NSTEMI differs depending on cardiac troponin levels and a quantitative relationship exists between the amount of elevation of cardiac troponins and the risk of death.18 The elevated levels of troponins are an adverse prognostic indicator, even after adjustment for clinical predictors and electrocardiographic findings. These effects are both short term and long term.6 The optimal troponin thresholds for risk stratification and therapeutic decision making remain a subject of debate, however, in almost all series, even minor elevations in troponin levels presage short and long term events.8,19 The prognostic value of cardiac troponins I and T appear equivalent.20 The cardiac troponins have high sensitivity, as yet unsurpassed, for the detection of even microscopic zones of myocardial necrosis (less than 1 gram of myocardial tissue).8,21 One issue with the use of cTnI is the multiplicity of existing assays that have different analytical sensitivities, some being unable to detect lower values with a reasonable precision. Results obtained with different cTnI assays vary considerably because of differences in standardization and in the antibodies used.22 In the present study, we used a quantitative, third generation assay to determine the cTnI levels which conforms to the European Society of Cardiology/ American College of Cardiology (ESC/ACC) committee recommendations for the diagnosis of myocardial infarction (MI).23
Troponin elevation has important therapeutic implications as well. It permits the identification of high-risk patients and of subsets of patients who will benefit from specific therapies, e.g. platelet glycoprotein IIb/IIIa inhibitors.24 Randomized studies have confirmed that early coronary intervention also attenuates the adverse prognostic impact of troponin elevations.25 Although an early invasive strategy improves outcome in these patients, there are limited data on culprit-only stenting versus multivessel stenting in the NSTEMI. More recently, in the large ACC National Cardiovascular Database Registry report involving 105,866 patients with no prior bypass graft surgery, multi-vessel CAD was found to be present in 42% of patients with NSTEMI. In about one third of these patients, multi-vessel percutaneous coronary intervention (PCI) was performed and the remaining patients had culprit single vessel PCI only. With the exception of peri-procedural MI, none of the other complications were significantly different from those patients undergoing culprit single vessel PCI.3
Overall, the results of our study suggest that elevated troponin I levels are associated with a greater severity and extent of myocardial ischaemic territory during the index event of NSTEMI. Patients were excluded if they had a prior history of CAD or revascularization procedures; hence the reported findings represent the actual status of the CAD severity and extent, not confounded by progression of previously known coronary lesions.
The limitations of this study include that it represents a single institution experience. The severity and location of the coronary lesions was based on the operator visual estimation without quantitative or physiological evaluation, however inter-observer agreement between angiographic images was taken into account in order to minimize bias. The study evaluated the extent of CAD in terms of the number of severely diseased major coronary arteries and was not designed to identify the culprit vessel or to assess the coronary lesion morphology-complex lesions, presence of intra-coronary thrombus, TIMI flow grades or collateral vessels with respect to the two cutoff levels of cTnI. Our conclusions should not be extended to cardiac troponin T or to the other assays available for Troponin I without further validation.
Conclusions
In acute coronary syndromes, it is essential to know the cardiac troponin status of a patient as early as possible as this would enable rapid triage of these patients and improved utilization of intensive care facilities in terms of the length of stay. Early coronary angiography should be considered especially in NSTEMI patients having higher troponin levels. These patients tend to have severe multi-vessel CAD and need prompt coronary revascularization.
Further studies should evaluate the relationship between different levels of cardiac troponins in NSTEMI and the in-hospital or follow-up cardiovascular events, the length of hospital stay and referral for PCI versus CABG surgery.
Acknowledgement
We acknowledge the efforts of Dr. Hammad Ali Qazi and Mr. Iqbal Mujtaba for their statistical assistance.
References
1.Asakura M, Ueda Y, Yamaguchi O, Adachi T, Hirayama A, Hori M, et al. Extensive development of vulnerable plaques as a pan-coronary process in patients with myocardial infarction: an angioscopic study. J Am Coll Cardiol 2001; 37: 1284-8.
2.Rigatelli G, Rigatelli G, Rossi P, Docali G. Normal angiogram in acute coronary syndromes: The underestimated role of alternative substrates of myocardial ischemia. Int J Cardiovasc Imaging 2004; 20: 471-5.
3.Brener SJ, Milford-Beland S, Roe MT, Bhatt DL, Weintraub WS, Brindis RG. American College of Cardiology National Cardiovascular Database Registry. Culprit-only or multivessel revascularization in patients with acute coronary syndromes: an American College of Cardiology National Cardiovascular Database Registry report. Am Heart J 2008; 155: 140-6.
4.Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines or the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction): developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol 2007; 14: 50; e1-e157.
5.Lopez BL, Aros BF, Lidon RM, Cequier FA, Bueno H, Alonso JJ, et al. Update of the guidelines of the Spanish Society of Cardiology for unstable angina/without ST-segment elevation myocardial infarction. Rev Esp Cardiol 2002; 55: 631-42.
6.Ottani F, Galvani M, Nicolini FA, Ferrini D, Pozzati A, Di Pasquale G, et al. Elevated cardiac troponin levels predict the risk of adverse outcome in patients with acute coronary syndromes. Am Heart J 2000; 140: 917-27.
7.Henrikson CA, Howell EE, Bush DE, Miles JS, Meininger GR, Friedlander T, et al. Prognostic usefulness of marginal troponin T elevation. Am J Cardiol 2004; 93: 275-9.
8.Morrow DA, Cannon CP, Rifai N, Frey MJ, Vicari R, Lakkis N, et al. Ability of minor elevations of troponins I and T to predict benefit from an early invasive strategy in patients with unstable angina and non-ST elevation myocardial infarction: results from a randomized trial. JAMA 2001; 286: 2405-12.
9.Sabatine MS, Morrow DA, McCabe CH, Antman EM, Gibson CM, Cannon CP. Combination of quantitative ST deviation and troponin elevation provides independent prognostic and therapeutic information in unstable angina and non-ST-elevation myocardial infarction. Am Heart J 2006; 151: 25-31.
10.López-Fernández S, Cequier A, Iràculis E, Gómez-Hospital JA, Teruel L, Valero J, et al. Elevated troponin I levels in patients with acute coronary syndrome without ST elevation are associated with increased complexity of the culprit lesion. Rev Esp Cardiol 2004; 57: 291-8.
11.Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, et al. Heart disease and stroke statistics- 2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2007; 115: e69-171.
12.Buffon A, Biasucci L, Liuzzo G, D\'Onofrio G, Crea F, Maseri A. Widespread coronary inflammation in unstable angina. N Engl J Med 2002; 347: 5-12.
13.Palazzuoli A, Gennari L, Calabria P, MD, Quatrini I , Vecchiato L, De Paola V, et al. Relation of plasma brain natriuretic peptide levels in non-ST-elevation coronary disease and preserved systolic function to number of narrowed coronary arteries. Am J Cardiol 2005; 96: 1705-10.
14.Dokainish H, Pillai M, Murphy SA, DiBattiste PM, Schweiger MJ, Lotfi A et al, TACTICS-TIMI-18 Investigators. Prognostic implications of elevated troponin in patients with suspected acute coronary syndrome but no critical epicardial coronary disease: a TACTICS-TIMI-18 substudy. J Am Coll Cardiol 2005; 45: 19-24.
15.Jurlander B, Farhi ER, Banas JJ Jr, Keany CM, Balu D, Grande P, et al. Coronary angiographic findings and troponin T in patients with unstable angina pectoris. Am J Cardiol 2000; 85: 810-4.
16.Okamatsu K, Takano M, Sakai S, Ishibashi F, Uemura R, Takano T, et al. Elevated troponin T levels and lesion characteristics in non-ST-elevation acute coronary syndromes. Circulation 2004; 109: 465-70.
17.Hamm CW, Braunwald E. A classification of unstable angina revisited. Circulation 2000; 102: 118-22.
18.Antman EM, Tanasijevic MJ, Thompson B, Schactman M, McCabe CH, Cannon CP, et al. Cardiac-specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med 1996; 335: 1342-9.
19.Jaffe AS, Ravkilde J, Roberts R, Naslund U, Apple FS, Galvani M, et al. It\'s time for a change to a troponin standard. Circulation 2000; 102: 1216-20.
20.Babuin L, Jaffe AS. Troponin: the biomarker of choice for the detection of cardiac injury. CMAJ 2005; 173: 1191-202.
21.Jeremias A, Gibson CM. Narrative review: alternative causes for elevated cardiac troponin levels when acute coronary syndromes are excluded. Ann Intern Med 2005; 142: 786-91.
22.Panteghini M, Pagani F, Yeo KT, Apple FS, Christenson RH, Dati F, et al. Evaluation of imprecision for cardiac troponin assays at low-range concentrations. Clin Chem 2004; 50: 327-32.
23.Apple FS, Wu AH, Jaffe AS. European Society of Cardiology and American College of Cardiology guidelines for redefinition of myocardial infarction: how to use existing assays clinically and for clinical trials. Am Heart J 2002; 144: 981-6.
24.Boersma E, Harrington RA, Moliterno DJ, White H, Théroux P, Van de Werf F, et al. Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: a meta-analysis of all major randomised clinical trials.. Lancet 2002; 359: 189-98.
25.Bavry AA, Kumbhani DJ, Quiroz R, Ramchandani SR, Kenchaiah S, Antman EM. Invasive therapy along with glycoprotein IIb/IIIa inhibitors and intracoronary stents improves survival in non-ST-segment elevation acute coronary syndromes: a meta-analysis and review of the literature. Am J Cardiol 2004; 93: 830-5.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: