
Riffat Sultana ( Karachi Institute of Heart Diseases, F.B. Area Karachi, Pakistan. )
Nuzhat Sultana ( Karachi Institute of Heart Diseases, F.B. Area Karachi, Pakistan. )
Syed Zahid Rasheed ( Karachi Institute of Heart Diseases, F.B. Area Karachi, Pakistan. )
Muhammad Ishaq ( Karachi Institute of Heart Diseases, F.B. Area Karachi, Pakistan. )
Abdus Samad ( Karachi Institute of Heart Diseases, F.B. Area Karachi, Pakistan. )
June 2010, Volume 60, Issue 6
Original Article
Abstract
Objective: To evaluate the successful revascularization in chronic total coronary occlusion lesions and to examine the relationship between lesion characteristics and procedural success and the frequency of in-hospital major adverse cardiac events after percutaneous coronary intervention in these patients.
Methods: All patients subjected to percutaneous coronary intervention from 2006 to 2008 were identified. These patients had unstable angina ranging from 2 weeks to more than 3 months duration, and majority was subjected to stent implantation.
Results: A total of 110 consecutive patients were studied. They had been treated for chronic total coronary occlusion lesions during this period. There were 76 males and 34 females. Drug eluting stents (DES) were used in 84 patients whereas 26 received Bare metal stents (BMS). Successful revascularization was achieved in 103 lesions (94%). Only 6% patients showed unsuccessful results due to failure of the wire to cross the lesion. There was no recorded death during the procedure.
Conclusion: Due to latest guide wire technology, procedural techniques and operator experience, our study showed more than 90% success in percutaneous revascularization of chronic total coronary occlusion lesions, with an excellent survival rate (JPMA 60:420; 2010).
Introduction
Chronic total occlusion of the Coronary arteries (CTO) defined as, "an obstruction of a native coronary artery for more than 30 days with no luminal continuity and with thrombolysis in myocardial infarction (TIMI) and flow grade 0 or 1 which has been present for at least six weeks."1,2 The temporal criterion used to define a CTO requires the range from >2 weeks to >3 months.3,4 Acute myocardial infarction and occluded saphenous vein grafts have been excluded from the definition. CTOS are characterized by significant narrowing of atherosclerotic vessel with lumen compromise that results in either complete interruption of antegrade blood flow as assessed by coronary angiography (TIMI grade 0 flow), also known as "true" total occlusions, or with minimal contrast penetration though the lesion without distal vessel opacification TIMI grade 1 flow, frequently referred to as "functional" total occlusion.5 There are three methods for treatment of CTO\'s: percutaneous intervention, coronary artery bypass surgery (CABG) and medical management. Less than 10% of CTO cases are managed by percutaneous intervention. Approximately 40% of the CTOS are treated by surgery and 50% by medications alone.6,7 Patients with CTO undergoing PCI usually have symptomatic angina; in several large databases, only 11% to 15% of patients undergoing angioplasty for CTO were asymptomatic, Conversely, the proportion of patients presenting with unstable angina due to a CTO is also fairly low (9% to 18%).8 Growing body evidence suggests a prognostic and symptomatic benefit of re-opening coronary chronic total occlusions (CTOS).9,10 Crossing the occlusion is still a main cause of failure. On the other hand, poor clinical outcome may be due to use of a bare-metal stent (BMS) after crossing the lesion and balloon dilatation. of the lesion.11 The introduction of the drug-eluting stent (DES) has clearly reduced angiographic restenosis and target lesion revascularization rates compared to BMS in the treatment of CTOS.12 Operator experience and specific tips and tricks for more difficult cases are needed to achieve procedural success in the majority of situations.13 Predictors of procedural success in PCI\'S of CTO\'S include length of occlusion, duration of occlusion, presence of tapered entry configuration, bridging collaterals and calcification.14 In total occlusions, the recanalization equipment should be passed through the atherosclerotic plaque, and its texture is crucial for the success or failure of the intervention. Although serious complications are rare, they do occur. In general, the success rates in literature range from 42-73%.15
This study was undertaken to evaluate the successful revascularization in chronic total coronary occlusion lesions and to examine the relationship between lesion characteristics and procedural success and the frequency of in-hospital adverse cardiac events.
Methods
A retrospective analysis of all coronary angiograms performed at the cardiac catheterization laboratory of Karachi Institute of Heart Diseases (KIHD) was conducted. KIHD is a tertiary referral center, located in a densely populated area of Karachi. The patients studied had the procedure done between August 2006 and August 2008. The inclusion criteria was Single de novo lesion, Coronary Total Occlusion with a reference diameter of 2.7 mm to 4 mm. Patients with Left Ventriclar Ejection Fraction < 30%, Left main artery patency > 50%, coexisting chronic heart failure, valvular heart disease, chronic renal failure, and contraindication to anticoagulation, were excluded from the study. Patients were evaluated for the occurrence of major adverse cardiac events comprising death, acute myocardial infarction, and need for repeat revascularization with either coronary artery bypass surgery or PCI.
Results
Table-1 shows the demographics of the total study population. Hundred and ten patients were selected of whom 76 were males and 34 were females. All were more than 40 years of age. Each patient had a chronic total occlusion Most patients 81 (74%) were treated with Drug eluting stents (Table-1).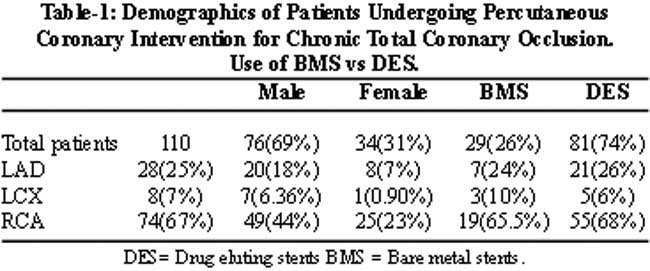
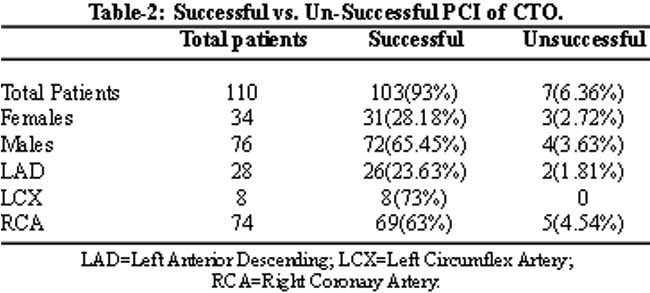
After high pressure balloon dilatation residual stenosis was reduced in all the cases. This facilitated stent deployment while post dilatation was required in a few cases. Successful revascularization was achieved in 103 lesions (94%), although stent implantation was used in 100%. The 6% patients who had unsuccessful results was due to failure of the wire to cross the lesion, long duration of CTO, abrupt missing stump, bridging collaterals, occluded length more than 15mm, moderate to severe calcification or tortuosity and ostial or distal location of CTO lesions. Due to limited resources IVUS (intravascular ultrasound) could not be performed. In the follow up period of 6 to 12 months, marked improvement of symptoms in majority of patients was noted (Table-3).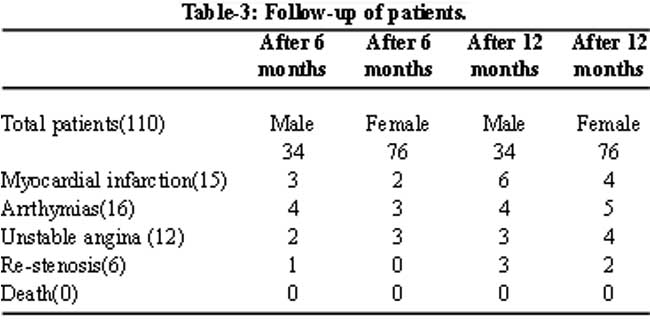
Fifteen patients suffered from Myocardial infarction, 16 developed arrthymias, 12 had unstable angina and 6 had re-stenosis. There was no death during the procedure or in the follow-up period.
Discussion
The revascularization of CTOs is technically difficult and remains a challenge for percutaneous coronary interventions. Successful revascularization of CTOs leads to improved survival and decreased major adverse events.16 Success rates in multiple series range from 54-63%, with more current success rates being reported at more than 70%. Newer technological advances, which include stiffer, tapered-tipped, and hydrophilic wires, have in part been responsible for this increased success.17 DES implantation for CTO decreases the risk of mid-term restenosis and Major Adverse Cardiac Event (MACE). Small vessels and diffuse disease requiring the implantation of multiple stents and very long stents for full coverage of the target lesion are still associated with a relatively high risk of restenosis.18 In our study DES utilization was more then BMS. Crossing the complex lesion and reentering into the true lumen remains the key step that limits the overall success of percutaneous procedures. The availability of new specialized guide wires designed to cross occluded arteries has only modestly improved procedural success rates. Allemann reported a success rate of 64% using the Magnum wire.19 Reimers achieved a crossing success rate of 71% using the Athlete wire in synergy with a floppy hydrophilic wire and low-profile balloon. Trials utilizing the Terumo Crosswire have demonstrated procedural success in 42% of situations when conventional guidewires have failed.20 New research has proved that micro dissection catheters may facilitate the recanalization of a vessel occlusion when the standard initial approach with coronary guidewires fails.21 More specifically drug-eluting stents significantly reduce the incidence of restenosis and re-occlusion when compared to bare-metal stents or plain-old balloon angioplasty.22 All patients were asked to undergo clinical follow-up examination at 1 week to 6-months after the procedure. Symptom status at baseline and at every follow-up examination was recorded following the Canadian Cardiovascular Society (CCS) classification.23
Myocardial infarction, repeat revascularization procedure and deaths were all recorded as major cardiac events.24 The duration of occlusion emerges as a key factor for success in most studies. The length of the occluded segment strongly influences the success rate of the intervention. The estimated length of the occlusion is measured from the point of the chronic occlusion to the most proximal point of the distal vessel, which is visualized by antegrade or retrograde collateral filling with contrast.25 Retrograde approach via collateral channels in coronary angioplasty for chronic total occlusion (CTO) can improve the success rate. Most interventionists will meet a few cases where the retrograde approach will provide unequaled advantages, but many are held back from taking retrograde approach by lack of proper equipment and expertise.
Conclusions
The presented study achieved a high success rate due to the use of the latest guide wire technology, good procedural techniques and highly skilled and experienced operators in percutaneous revascularization of chronic total coronary occlusion. lesions, with an excellent survival rate. The use of Drug-Eluting Stents has provided an added advantage of marked reduction in re-stenosis.
The results of the follow up also proved that due to successful percutaneous recanalization of CTO there was improved survival, as well as enhanced left ventricular function, reduction in angina, and improved exercise tolerance.
Acknowledgement
The authors gratefully acknowledge the excellent assistance of all medical personnel in the catheterization laboratory of KIHD.We also thank Mr. Shah Amir Haq who helped us to successfully complete this study.
References
1.Galla JM, Whitlow PL. Coronary chronic total occlusion. Cardiol Clin 2010; 28: 71-9.
2.Park CS, Kim HY, Park HJ, Ihm SH, Kim DB, Lee JM, et al. Clinical, electrocardiographic, and procedural characteristics of patients with coronary chronic total occlusions. Korean Circ J 2009; 39: 111-5. Epub 2009 Mar 25.
3.Werner GS, Emig U, Mutschke O, Schwarz G, Pedersen KE, Hansen N, et al. Regression of collateral function after recanalization of chronic total coronary occlusions: a serial assessment by intracoronary pressure and Doppler recordings. Circulation 2003; 108: 2877-82.
4.Tamai H, Berger PB, Tsuchikane E, Suzuki T, Nishikawa H, Aizawa T, et al, for the MAJIC Investigators. Frequency and time course of reocclusion and restenosis in coronary artery occlusions after balloon angioplasty versus Wiktor stent implantation. Am Heart J 2004; 147: E9.7.
5.Zidar FJ, Kaplan BM, O\'Neill WW, Jones DE, Sehreiber TL, Safian RD, et al. Prospective, randomized trial of prolonged intracoronary urokinase infusion for chronic total occlusions in native coronary arteries. J Am Coll Cardiol 1996; 27: 1406-12.
6.Stone GW, Kandzari DE, Mehran R, Colombo A, Schwartz RS, Bailey S, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part I. Circulation 2005; 112: 2364-72.
7.Abbott JD, Kip KE, Vlachos HA, Sawhney N, Srinivas VS, Jacobs AK, Holmes DR, Williams DO. Recent trends in the percutaneous treatment of chronic total coronary occlusions. Am J Cardiol 2006; 97: 1691-6. Epub 2006 Apr 21.
8.Rubartelli P, Verna E, Niccoli L, Giachero C, Zimarino M, et al Occlusioni Coronariche Investigators. Coronary stent implantation is superior to balloon angioplasty for chronic coronary occlusions: six-year clinical follow-up of the GISSOC trial. J Am Coll Cardiol 2003; 41: 1488-92.
9.Stone GW, Reifart NJ, Moussa I, Hoye A, Cox DA, Colmbo DS, et al. Percutaneous recanalization of chronically occluded coronary arteries: A consensus document: Part I. Circulation 2005; 112: 2364-72.
10.Stone GW, Reifart NJ, Moussa I, Hoye A, Cox DA, Colombo DS, et al. Percutaneous recanalization of chronically occluded coronary arteries: A consensus document: Part II. Circulation 2005; 112: 2530-7.
11.Ge L, Iakovou I, Cosgrave J, Chieffo A, Montorfanod M, Michev I, et al. Immediate and mid-term outcomes of sirolimus-eluting stent implantation for chronic total occlusions. Eur Heart J 2005; 26: 1056-62.
12.Nakamura S, Muthusamy TS, Bae JH, Cahyodi YH, Udayachalem W, Treskusol D. Impact of sirolimus-eluting stent on the outcome of patients with chronic total occlusions. Am J Cardiol 2005; 95: 161-6.
13.Rathore S, Matsuo H, Terashima M, Kinoshita Y, Kimura M, Tsuchikane E, et al. Procedural and in-hospital outcomes after percutaneous coronary intervention for chronic total occlusions of coronary arteries 2002 to 2008: impact of novel guidewire techniques. JACC Cardiovasc Interv 2009; 2: 489-97.
14.Noguchi T, Miyazaki S, Morii I, Dalkoku S, Goto Y, Nonogi H. Percutaneous transluminal coronary angioplasty of chronic total occlusions. Determinants of primary success and long-term clinical outcome. Catheter Cardiovasc Interv 2000; 49: 258-64.
15.Dong S, Smorgick Y, Nahir M, Lotan C, Mosseri M, Nassar H, et al. Predictors for successful angioplasty of chronic totally occluded coronary arteries. J Interv Cardiol 2005; 18: 1-7.
16.Christofferson RD, Lehmann KG, Martin GV, Every N, Caldwell JH, Kapadia SR. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol 2005; 95: 1088-91.
17.Ge JB, Zhang F, Ge L, Qian JY, Wang H. Wire trapping technique combined with retrograde approach for recanalization of chronic total occlusion. Chin Med J (Engl) 2008; 121: 1753-6.
18.Migliorini A, Moschi G, Vergara R, Parodi G, Carrabba N, Antoniucci D. Drug-eluting stent-supported percutaneous coronary intervention for chronic total coronary occlusion. Catheter Cardiovasc Interv 2006; 67: 344-8.
19.Kahler J, Koster R, Brockhoff C, Reimers J, Baldus S, Terves W, et al. Initial experience with a hydrophilic-coated guidewire for recanalization of chronic coronary occlusions. Cathet Cardiovasc Intervent 2000; 49: 45-50.
20.Whitbourn RJ, Cincotta M, Mossop P, Selmon M. Intraluminal blunt microdissection for angioplasty of coronary chronic total occlusions. Catheter Cardiovasc Interv 2003; 58: 194-8.
21.Tadros P. Successful revascularization of a long chronic total occlusion of the right coronary artery utilizing the Frontrunner X39 CTO catheter system. J Invasive Cardiol 2003; 15:3.
22.Iofina E, Radke PW, Skurzewski P, Haager PK, Blindt R, Koch KC, et al. Sirolimus- and paclitaxel-eluting stents in comparison with balloon angioplasty for treatment of in-stent restenosis. Catheter Cardiovasc Interv 2005; 64: 28-34.
23.Cox J, Naylor CD. The Canadian Cardiovascular Society grading scale for angina pectoris: is it time for refinements? Ann Intern Med 1992; 117: 677-83.
24.Suero JA, Marso SP, Jones PG, Laster SB, Huber KC, Giorgi LV, et al. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries: a 20-year experience. J Am Coll Cardiol 2001; 38: 409-14.
25.Olivari Z, Rubartelli P, Piscione F, Ettori F, Fontanelli A, Salemme L, et al. Immediate results and one-year clinical outcome after percutaneous coronary interventions in chronic total occlusions. J Am Coll Cardiol 2003; 41: 1672-8.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: