
Ahsan Yaqoob Khan ( Department of Psychiatry & Behavioral Health, University of Kansas School of Medicine, Wichita. )
Mohammad Rafique Shaikh ( Department of Psychiatry & Behavioral Health, University of Kansas School of Medicine, Wichita. )
Elizabeth Ablah ( Department of Psychiatry & Behavioral Health, University of Kansas School of Medicine, Wichita. )
June 2010, Volume 60, Issue 6
Original Article
Abstract
Objective: To examine the extent of compliance to the proposed monitoring protocol among practicing psychiatrists for second generation antipsychotics.
Methods: Questionnaire was sent through Survey Monkey to practicing psychiatrists in the states of Iowa, Kansas, Missouri, Nebraska, Oklahoma and Texas. Also paper surveys were distributed to individual psychiatrists of Kansas and Nebraska at their grand rounds, inpatient settings, and outpatient clinics.
Results: Ninety eight responses were received of which 51 participants completed the survey on Survey Monkey and 47 completed the paper surveys. Fifty-one percent reported that 25% to 50% of their patients were taking SGAs. About two thirds (69.4%) reported familiarity with the proposed protocol, 17.3% were unfamiliar, and 13% were not sure. Of those who were familiar, 63% percent reported their adherence to the protocol, 21% did not follow the protocol, and 16% were not sure. However, when their responses were closely examined, only five (5%) of the respondents were found completely adherent to the protocol.
Conclusions: Majority of participants were aware of the proposed protocol to protect their patients from metabolic side effects but many of them did not follow it completely. A large study at the national level needs to be done to replicate these findings (JPMA 60:446; 2010).
Introduction
Antipsychotic medications have been the mainstay of treatment for psychotic illnesses. Second Generation Antipsychotics (SGAs) have become widely used due to their efficacy in treating both positive as well as negative symptoms and favourable side effect profile compared to first generation antipsychotics. In 2003, representatives of the American Diabetes Association (ADA), American Psychiatric Association (APA), American Association of Clinical Endocrinologists (AACE) and the North American Association for the Study of Obesity (NAASO) developed a consensus position on the subject of antipsychotic drugs and metabolic syndrome. These were published and widely publicized among psychiatrists and family physicians using the SGAs.1,2
Recently, the baseline data from Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) revealed that prevalence of metabolic syndrome is higher than previously thought. Overall prevalence of metabolic syndrome was 43% among fasting cohort of CATIE subjects at baseline using diagnostic criteria for metabolic syndrome proposed by the American Heart Association (AHA).3 The diagnostic criteria of the metabolic syndrome as adopted from McEvoy JP et al are shown in Table-1.

Given the serious health risks, patients taking SGAs should receive appropriate screening and monitoring. Patient, family members and caregivers should be educated about these risks and the importance of monitoring. The patient may be referred to specialized services if problems with significant weight gain, new onset diabetes, or other cardiovascular risk factors occur. This will help reduce the likelihood of developing cardiovascular disease, diabetes, or other diabetic complications.4,5 Recommended monitoring protocol is shown in the Table-2.
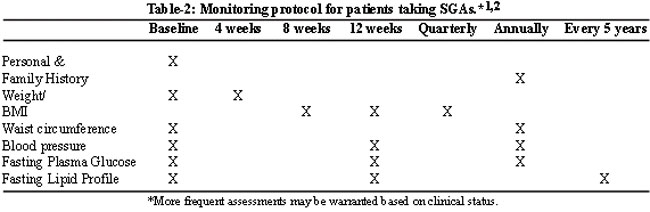
Some observers criticized the recommendations as impractical. Some thought that baseline tests were too involved and expensive. Others thought that fasting lipid to be monitored every 5 years was negligent and risky.6
Despite the availability of the monitoring protocol and the discussions and alerts published, the number of studies and case reports about serious metabolic effects associated with the use of SGAs continues to be on the rise.7-10 In 2003, Newcomer et. al. did a nationwide survey of randomly selected psychiatrists who routinely treat schizophrenia with SGAs. It was conducted to determine their practice patterns and knowledge about metabolic disturbances associated with SGA therapy. The results of this survey published in 2004, indicated that psychiatrists were aware of and concerned about metabolic risks with SGA use.11
Based on the results from the Newcomer`s survey and CATIE study, we designed a survey study to answer the following questions:
1) How many psychiatrists knew about the recommended protocol for SGAs use?
2) Of those who were aware of the protocol, how many of them were following the protocol completely, if not, to what extent?
3) Those who were non-adherent to the protocol, what were the reasons behind their non-adherence?
This report contains the data from the ninety eight responders of this survey. Answer to all these questions will help in modifying the protocol and make it more user-friendly which in turn will improve adherence to the protocol and reduce the likelihood of developing the metabolic syndrome.
Methodology
Practicing Psychiatrists from states of Iowa, Kansas, Missouri, Nebraska, Oklahoma and Texas were approached for this survey study.
The survey questionnaire requested the responder to answer seven questions. It was accompanied by a brief statement explaining the purpose of this survey study. The questionnaire was designed to determine the familiarity of the practicing psychiatrists with the monitoring protocol proposed in 2004, how many of them were following it completely and if not what were the reasons for them not to adhere to the protocol. They were also asked to mark which of the individual tests they performed at baseline before starting a patient on SGAs and which they repeated at 12 weeks into treatment. Finally, they were asked to report about the number of years they were in practice and what percent of their patients were taking SGAs.
After approval from the local Institutional Review Board (IRB), the survey questionnaire was sent in June 2007 through Survey Monkey to 80 psychiatrists on the e-mailing list of Kansas Psychiatric Society. Only three responses were received. Therefore another strategy to reach the target population was added. The practicing psychiatrists in Kansas and Nebraska were approached individually at varied locations such as grand rounds, faculty meetings, inpatient facilities and outpatient clinics. They were provided a paper version of the survey and were requested to fill out the surveys. Thus we received 47 responses making the total of 50 responses in December 2007. In February 2008, 363 email requests through Survey Monkey were sent to practicing psychiatrists in Iowa, Missouri, Nebraska, Oklahoma and Texas. Eighty seven of these emails returned with \'unable to deliver\' remark. After about 3 weeks, a round of 276 email reminders was sent through Survey Monkey. We obtained 48 responses by these efforts bringing the total of respondents to 98 participants.
Results
Ninety eight responses were received of which 51 responses were obtained via Survey Monkey while 47 responses were obtained in person.
More than two-thirds (69.4%) of respondents reported they were familiar with the monitoring protocol, 17.3% reported they were unfamiliar, and 13% reported they were "not sure." Of those who reported being familiar, 63% reported they adhere to the protocol, 21% reported they did not follow the protocol, and the remaining 16% were "not sure." Respondents who reported they did not adhere to the protocol provided a variety of reasons for their non-adherence (Figure).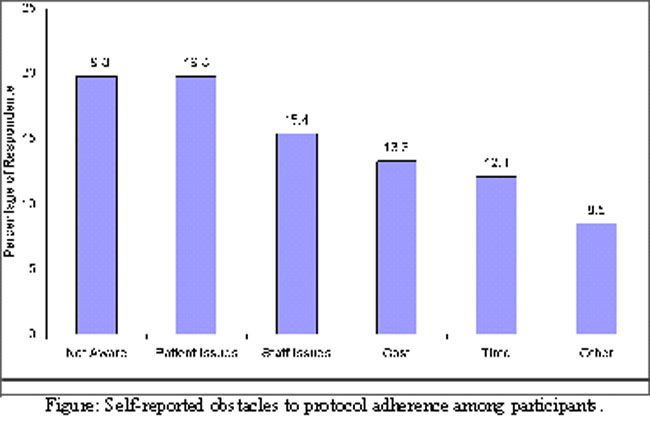
Respondents were provided an opportunity to indicate "other" reasons for non-adherence to the protocol. Responses included comments like, "I am comfortable with close follow up, and observation;" "I stick to the VA algorithm;" and "the PCPs I work with generally stay on top." "As a department we decided against waist circumference. We monitor other parameters but at no fixed schedule". "This protocol is burdensome.
In addition to respondents\' self-reporting familiarity with and adherence to the protocol, respondents also had the opportunity to select the tests they perform at baseline (before starting patients on a SGA) and at 12 weeks into treatment with SGAs (Table-2). Partial adherence to the protocol was noted between these 2 visits. While 44% of the respondents claimed adherence to protocol, only 5% were actually 100% adherent as derived from their self-reports of tests they performed at baseline and at 12 weeks after treatment with SGAs.
Of the total 98 respondents, 23.5 % reported being in practice for less than 5 years; 24.5% reported being in practice for 5 to 10 years, and 49% reported they had been in practice for more than 10 years and 3.1% did not answer this question. Nearly 51% of respondents reported that approximately 25% to 50% of their patients were prescribed SGAs.
Discussion
Results from this survey brought some interesting facts to the surface. Fifty one responses were obtained through survey monkey and the rest of the 47 responses were obtained via personal contacts. The rate of response was similar when Stanford University sent out a survey to determine perception of weight gain and bipolar pharmacotherapy at a national level to 7000 psychiatrists in 2005 and to a different group of 7000 psychiatrists in 2006 and got only 298 responses.12 Few possible reasons that may explain the poor response include technical issues such as inability to open attachment in the e-mail, lack of incentive to do the survey, time constraint, fear of litigation, disagreement with the survey, and lack of understanding about the purpose of the survey.
Interestingly, 69.4% of the respondents reported that they were familiar of the protocol proposed by the consensus panel of experts from ADA, APA, AACE, and NAASO. That suggests that 30.6% of the practicing psychiatrists from the representative sample reported to be unaware of this protocol in spite of wide publicity and publications in reputable professional journals.
Of those 69.4%, only 44% claimed that they followed the said recommendations. However, in the same survey, psychiatrists were asked to mark which tests they did or did not perform at baseline and at 12 weeks after starting SGA therapy. Based on their responses it was revealed that only 5% fully followed the protocol at these two junctures. This finding is also close to the findings of a study by Cuffel et al. which analyzed a nationwide database from 85 health plans to determine extent of increase in lipid and glucose monitoring in patients prescribe SGAs after release of the ADA and APA consensus statement in 2004. He reported that after consensus 8.5% and 22.5% of patients had their lipids and glucose tested as compared to 7.8 % and 20.6% before the publication of ADA/APA consensus protocol.13 In our survey, 62% reported performing fasting lipids and 68% reported performing fasting glucose at baseline. Although the percentage of psychiatrists performing fasting lipids and glucose was significantly higher in our survey study, our data is based solely on self reporting as compared to the chart review done in Cuffel study. Monitoring waist circumference at baseline was only 20% in our survey which is consistent with the findings of Atypical Antipsychotic Therapy and Metabolic Issues National Survey done in 2004.11
In our survey, those who admitted that they did not follow the protocol were asked to choose the reason of their non adherence from a list of options. The major reasons reported were patient issues (needle phobia, lack of insight, co-pay for the labs, time); clinicians issue including reimbursement factors, availability of staff member, natural resistance to change, and lack of system support. However; individually these made 20% or less of the total of respondents who were non adherent to the protocol. In summary, we can say that lack of incentives and reimbursement along with lack of coordination between medical and mental health systems makes the implementation of the protocol difficult.
From the results of our survey study, we would like to make following recommendations to protect our patients from preventable metabolic side effects of SGAs:
1.Psychiatrists who feel that monitoring and treatment of metabolic disorder don\'t fall within the scope of their expertise should collaborate with family physicians, endocrinologists, dietitians and other professionals to follow the monitoring protocol for SGAs.
2.Big treatment facilities like community health centers and university out patient clinics can develop a medication (SGAs) use review process. A committee of practitioners can initiate a procedure by which they can determine if any of the member physicians has deviated from recommended practice. This is then utilized to increase compliance to protocol by feedbacks and guidance.
3.Many non-psychiatrist professionals like primary care physicians also prescribe SGAs in significant proportions. They need to be made more aware of these potential metabolic risks and about the resources available to them and their patients so that these adversities may be prevented or circumvented.
4.Pharmacies filling the scripts of SGAs may provide some sort of educational alerts to the patients (e.g. did your doctor weigh you? Did they perform blood tests for sugar and lipids before they prescribed this medication?) as well as to the prescribing office through similar reminders.
5.Supporting staff at clinics and hospitals can educate the patients and their families the importance of integrating medical monitoring and psychiatric symptom monitoring.
6.Finally, make the monitoring mandatory for the clinicians through national drug approval authority, so no patient will get their SGAs without having pre-requisite labs. and other tests results send to the pharmacy. Similar protocol is in place for clozapine to monitor the bone marrow depression, a potential and deadly adverse effect of clozapine.
Following are some limitations to this preliminary report:
a) It was based on the data for the total of 98 responses. Thus, the sample was small.
b) It was a regional and not national study.
c) The study design included convenience sampling; this may not be representative of the target population.
d) The survey questionnaire included the questions regarding practices at the beginning and 12 weeks down the initiation of SGAs. It did not include the questions about the adherence to recommendations at 1 year or at 5 years.
e) The responses were taken at their face value. No verification of the reported practice was involved. Thus, the data was subject to recall bias.
Conclusions
Psychiatrists seem to be well aware of the metabolic side effects related to the use of SGAs. However many of them are not aware of the protocol recommended to protect their patients from these side effects. Of those who are aware of this monitoring protocol, majority of them are not following it completely. That is why; incidence of metabolic syndrome is on the rise in patients with mental disorders. Large study at national level needs to be done to replicate these findings. Efforts to improve adherence to protocol can be more successful if the mental and physical health caregivers are more integrated and the health systems foster this integration from the level of patient education to the level of care delivery. Results from the CAMP study will hopefully provide guidance to practitioners in selecting the appropriate SGA for a given patient.
References
1.Clark NG. American Diabetes Association. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care 2004; 27: 596-601.
2.American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, North American Association for the study of obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. J Clin Psychiatry 2004; 65: 267-72.
3.McEvoy JP, Meyer JM, Goff DC, Nasrallah HA, Davis SM, Sullivan L, et al. Prevalence of the metabolic syndrome in clinical antipsychotic patients with schizophrenia; baseline results from the Clinical Antipsychotic Trials of Intervention Effectiveness [CATIE] schizophrenia trial and comparison with national estimates from NHANES III. Schizophr Res 2005; 80: 19-32.
4.Moisan J, Grégoire JP, Gaudet M, Cooper D. Exploring the risk of diabetes mellitus and dyslipidemia among ambulatory users of atypical antipsychotics: A population-based comparison of risperidone and olanzapine. Pharmacoepidemiol Drug Saf 2005; 14: 427-36.
5.Lambert BL, Cunningham FE, Miller DR, Dalack GW, Hur K. Diabetes risk associated with use of olanzapine, quetiapine and risperidoneveterans health administration patients with Schizophrenia. Am J Epidemiol 2006; 164: 672-81.
6.Barrett E. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care 2004; 27: 2089-90.
7.De Hert MA, van Winkel R, Van Eyck D, Hanssens L, Wampers M, Scheen A, et al. Prevalence of the metabolic syndrome in patients with schizophrenia treated with antipsychotic medication. Schizophrenia Res 2006; 83: 87-93.
8.Marlowe K, Howard D, Chung A. New onset Diabetes with Ketoacidosis attributed to Quetiapine. Southern Med J 2007; 100: 829-31.
9.Perez-Iglesias R, Crespo-Facorro B, Amado JA, Garcia Unxieta MT, Ramirez Bonilla ML, Gonzalez Blanch C, et al. A 12 week Randomized clinical trial to evaluate metabolic changes in Drug-Naïve, First-Episode Psychosis Patients treated with Haloperidol, Olanzapine or Risperidone. J Clin Psychiatry 2007; 68: 1733-40.
10.Yamuchi T, Tice A. Metabolic abnormalities associated with atypical antipsychotics: a case report and alert. Hawaii Med J 2007; 66: 12-3.
11.Newcomer J, Nasrallah H, Loebel A. The Atypical Antipsychotic Therapy and Metabolic Issues National Survey: Practice patterns and knowledge of psychiatrists. J Clin Psychopharmacol 2004; 24: S1- 6.
12.Ketter TA, Haupt DW. Perception of weight gain and bipolar pharmacotherapy; result of a 2005 survey of physicians in clinical practice. Curr Med Res Opin 2006; 22: 2345-53.
13.Cuffel B, Martin J, Joyce AT. Lipid and glucose monitoring during atypical antipsychotic treatment: effects of 2004 ADA/APA consensus statement [Poster]. Presented at 159th annual meeting of the American Psychiatric Association 2006 May 20-25; Toronto, Ontario, Canada.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: